3224
Detection of Hippocampal Sclerosis in Epilepsy using GRAPPATINI T2-relaxometry1Florey Institute, Melbourne, Australia, 2Department of Neurology, Austin Health, Melbourne, Australia, 3Department of Neuropsychology, Austin Health, Melbourne, Australia
Synopsis
Keywords: Epilepsy, Epilepsy, EEG, multi-echo
Motivation: Detecting hippocampal sclerosis (HS) makes effective surgical treatment a possibility for people with drug-resistant epilepsy. However, use of conventional hippocampal T2 relaxometry has been hampered by long acquisition times and complex post-processing.
Goal(s): To apply GRAPPATINI, an accelerated acquisition and T2 map reconstruction method, in the Australian Epilepsy Project for improved detection of HS.
Approach: Prospective observational cohort study in 206 people with epilepsy and 69 controls.
Results: GRAPPATINI hippocampal T2 values showed low variance in healthy controls, and marked increases with HS at the group-level. Inclusion in a binary classifier improved detection of HS over using volumetric data alone.
Impact: Measurement of hippocampal T2 in people with epilepsy, using GRAPPATINI and automated processing, enables improved quantitative assessment of hippocampal sclerosis. This study demonstrates the feasibility and potential additive benefit of this method in a real-world clinical population.
Introduction
Hippocampal sclerosis (HS) is characterized by neuronal loss and gliosis of the hippocampal subfields1, a pathology that is commonly found in people with drug-resistant temporal lobe epilepsy. In an individual with epilepsy, the radiological diagnosis of HS can be life-changing, as it raises possible causes of their epilepsy, and opens the possibility of effective treatment through epilepsy surgery. It has been recognised for more than 30 years that quantitative T2 relaxometry can improve detection and diagnosis of HS2, but this technology has seen limited uptake because of the challenges of long acquisition times for whole-brain coverage, and subsequent efforts have progressed automated processing and employed acquisitions with few sampled echoes3. GRAPPATINI is a recent method for accelerated model-based T2 mapping, based on a Carr–Purcell–Meiboom-Gill acquisition but combining k-space undersampling with parallel imaging4, and the advantage of on-scanner map reconstruction. In this study we adapted GRAPPATINI parameters for assessment of the hippocampus, and evaluate its performance in a large real-world clinical cohort of people with epilepsy.Methods
Participants: We studied 275 participants from the Australian Epilepsy Project (www.epilepsyproject.org.au), comprising people with a first unprovoked seizure (n=42), newly-diagnosed epilepsy (n=91) and drug-resistant focal epilepsy (n=73), in addition to healthy controls (n=69). Overall, median age was 34.5y (range 18-66y) with 59% female participants.GRAPPATINI acquisition: Images were acquired at a single site on a Siemens Prisma-fit 3T scanner. T2 maps were generated using GRAPPATINI4 (44 coronal oblique slices perpendicular to the hippocampal axis, voxel size 0.9 x 0.9 x 3.6mm, 16 echoes with TE1/ΔTE/TR=10.7/10.7/3910ms, flip angle 180°, 2 interleaved concatenations, 10% slice gap, bandwidth 219 Hx/px, low SAR RF pulse, GRAPPA x2, undersampling factor x5). Acquisition time was 3:17 min.
MRI clinical assessment: Additional AEP imaging included whole-brain 3d T1w-MPRAGE, T2w-FLAIR and 2d Coronal T2w-TSE, meeting ILAE guidelines5 for clinical assessment of epilepsy. Images were clinically reported by subspecialist epilepsy Neuroradiologists. A diagnosis of hippocampal sclerosis was noted in 18 people (10 left, 6 right, 2 bilateral).
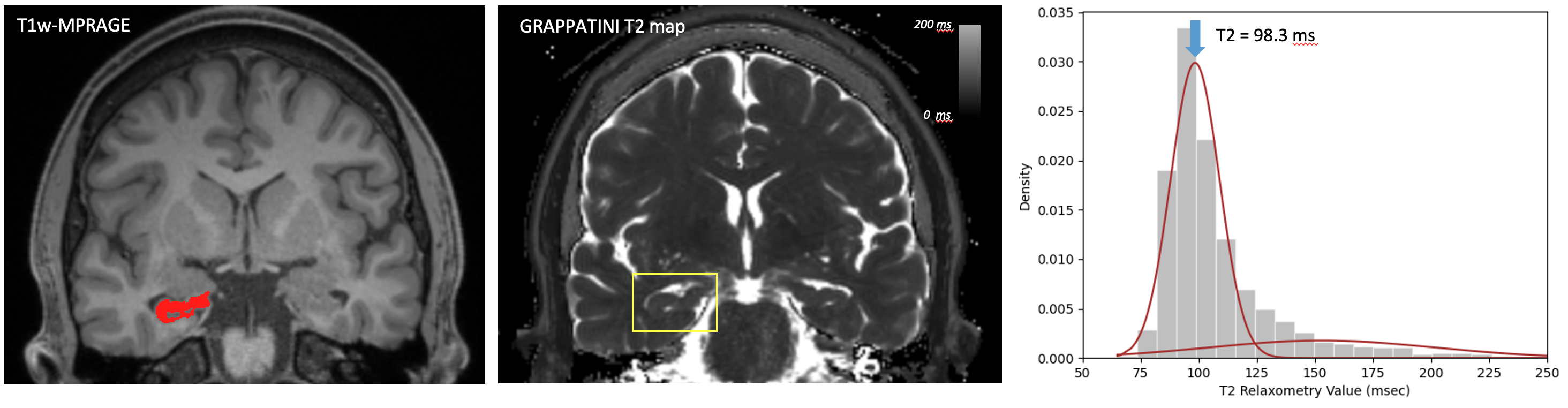
Image processing: Hippocampal subfield segmentation (FreeSurfer v7) was performed on T1w-MPRAGE and Coronal T2w-TSE images. The GRAPPATINI T2 map was registered to T1w image by rigid-body registration using ANTs. Voxelwise T2-relaxation times were extracted from the left and right hippocampus. A summary T2 value for each hippocampus was derived using a 2-gaussian mixture model, to account for CSF partial volume in some voxels (Fig.2). Hippocampal T2 values were adjusted for age and sex using a linear model derived from healthy controls, and hippocampal volumes similarly adjusted for age, sex and intracranial volume (eTIV).
Hippocampal sclerosis classifier: A binary naïve Bayes classifier was trained to distinguish people with versus without hippocampal sclerosis amongst the epilepsy cohort, using stratified 5-fold cross-validation and 10 repetitions. We compared predictions based on hippocampal volumes alone to those using hippocampal T2 only, and volumes plus T2 values combined.
Results
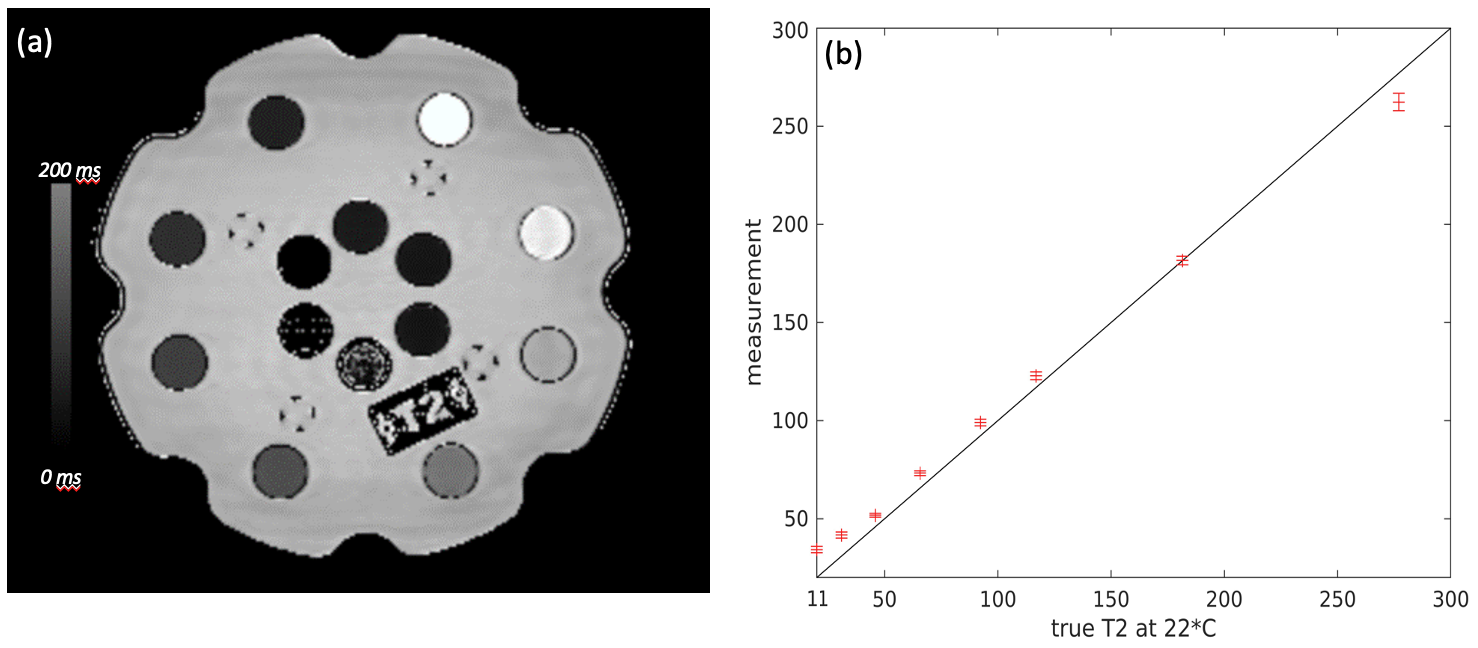
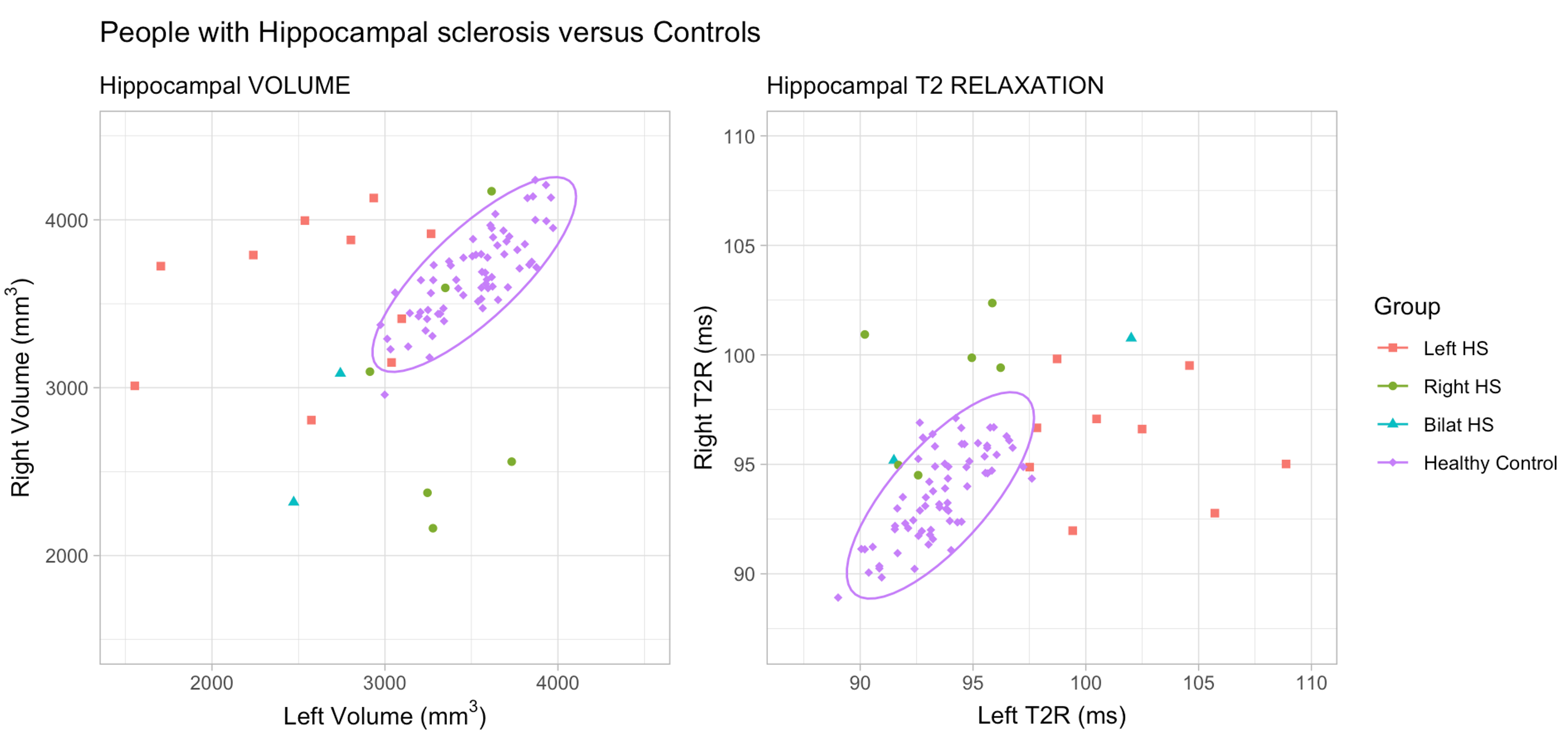
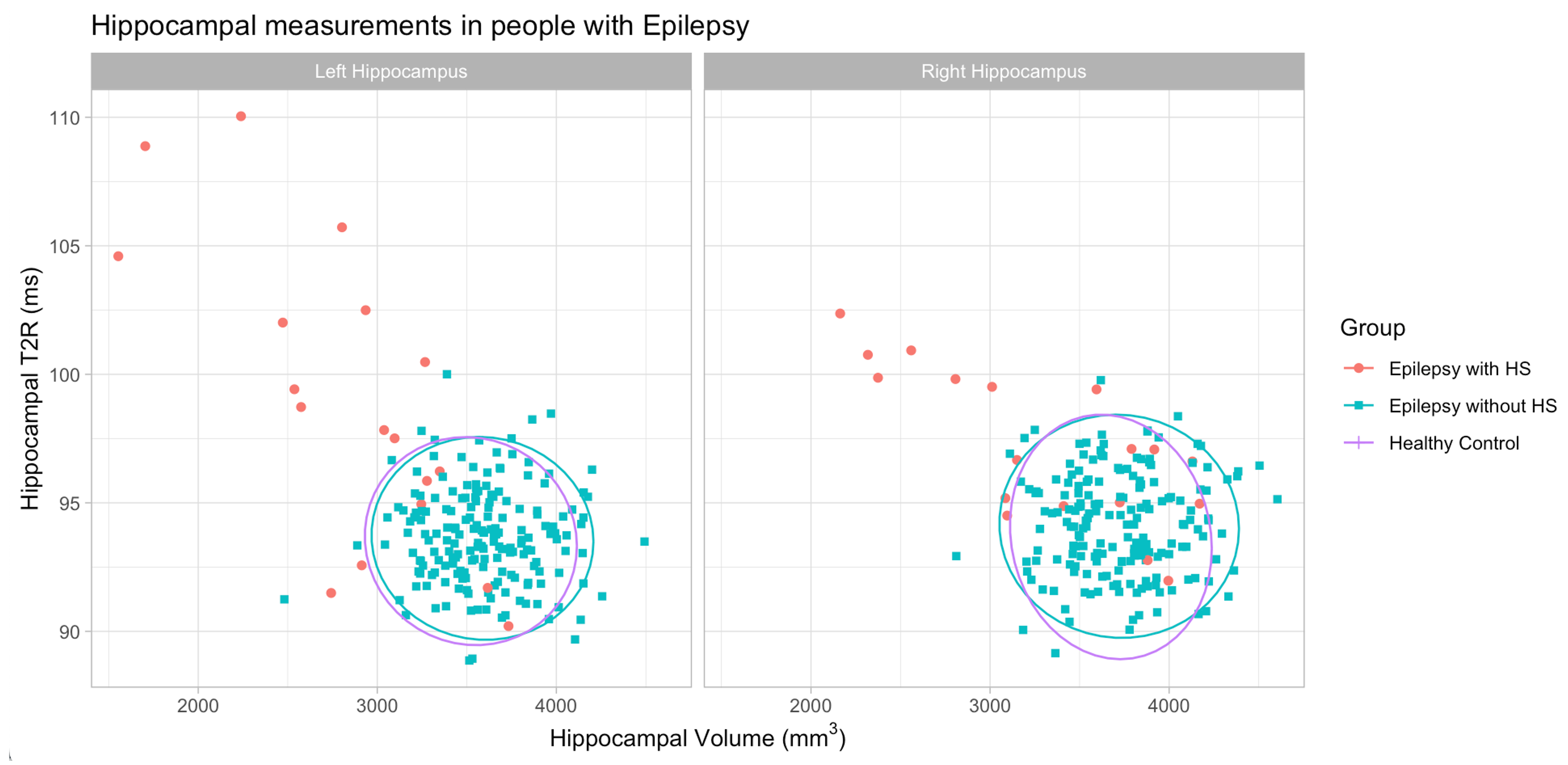
The GRAPPATINI acquisition applied to the NIST phantom (Fig 1) showed good concordance between true and measured T2 values, with RMSE=3.3ms over the demonstrated T2 range.In healthy controls, mean adjusted hippocampal T2 values were left 93.5±1.8 (s.d.) ms and right 93.6±2.1 ms (Fig 3). In people with epilepsy, left hippocampal T2 was increased with left HS (mean 101.6±5.2ms, p<0.001) and right hippocampal T2 was increased with right HS (mean 98.5±3.1ms, p=0.003) relative to healthy controls (Fig 3). In the remainder of people with seizures or epilepsy there was no significant difference in hippocampal T2 compared to controls (Fig 4).
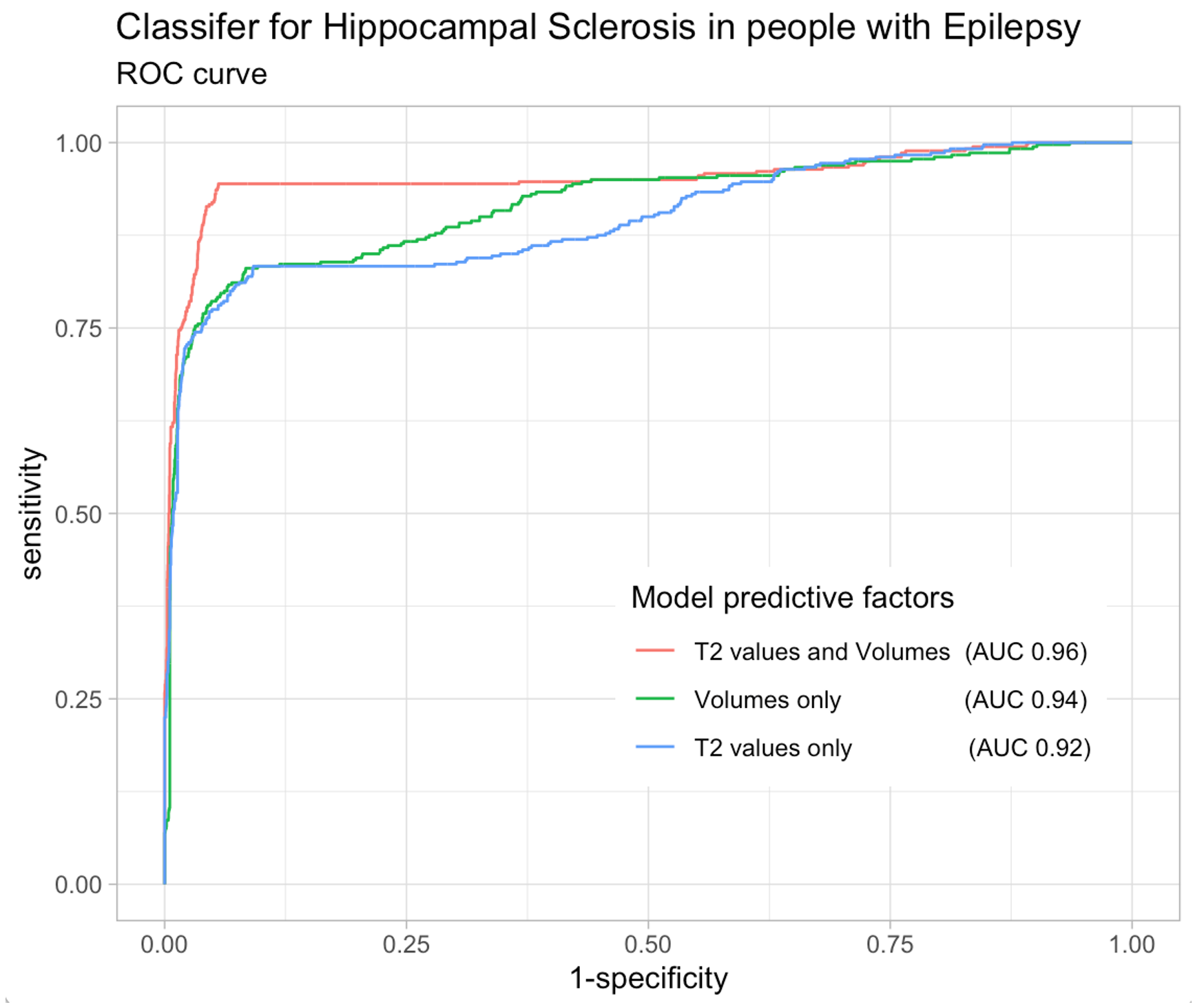
Binary classifiers to identify people with HS within the epilepsy cohort performed best when including both hippocampal T2 and volume as predictors (AUC 0.96 averaged over all folds, accuracy 96%, sensitivity 77%, specificity 99%). This was significantly better than predictions from hippocampal volume alone (average performance AUC 0.94, model difference p=0.01) and predictions using hippocampal T2 values alone (average performance AUC 0.92, model difference p=0.002).
Conclusion
Rapid whole-brain GRAPPATINI for assessment of hippocampal T2 relaxation time is feasible in a real-world cohort of people with seizures and/or epilepsy, with an acquisition time under 3½ minutes. The resulting automated hippocampal T2 values show relatively low variance in healthy controls, and at the group level a clear T2 increase in the presence of hippocampal sclerosis. Including hippocampal T2 values in a binary classifier for HS, along with hippocampal volumes, significantly improved the classifier performance, suggesting that this approach may assist the automated diagnosis of hippocampal sclerosis in people with epilepsy.Acknowledgements
We thank Tom Hilbert, Tobias Kober and Kieran O’Brien from Siemens Healthineers for their development and assistance with the GRAPPATINI sequence. The Australian Epilepsy Project receives funding from the Australian Government under the Medical Research Future Fund. We acknowledge the facilities and scientific and technical assistance of the National Imaging Facility, a National Collaborative Research Infrastructure Strategy (NCRIS) capability. We also acknowledge funding from the Victorian Government Operational Infrastructure Support Grant, support from the Victorian Biomedical Imaging Capability (VBIC), and from the MASSIVE high-performance computing facility.References
- Blümcke I, Thom M, Aronica E, et al. International consensus classification of hippocampal sclerosis in temporal lobe epilepsy: A Task Force report from the ILAE Commission on Diagnostic Methods. Epilepsia. 2013;54:1315–1329.2.
- Jackson GD, Connelly A, Duncan JS, Grünewald RA, Gadian DG. Detection of hippocampal pathology in intractable partial epilepsy: increased sensitivity with quantitative magnetic resonance T2 relaxometry. Neurology. 1993;43:1793–1799.3.
- Winston GP, Vos SB, Burdett JL, Cardoso MJ, Ourselin S, Duncan JS. Automated T2 relaxometry of the hippocampus for temporal lobe epilepsy. Epilepsia. 2017;58:1645–1652.4.
- Hilbert T, Sumpf TJ, Weiland E, et al. Accelerated T2 mapping combining parallel MRI and model-based reconstruction: GRAPPATINI. J Magn Reson Imaging. 2018;48:359–368.5.
- Bernasconi A, Cendes F, Theodore WH, et al. Recommendations for the use of structural magnetic resonance imaging in the care of patients with epilepsy: A consensus report from the International League Against Epilepsy Neuroimaging Task Force. Epilepsia. 2019;60:1054–1068.
Figures