3213
Ferumoxytol Dose Optimization for 3D Whole-Heart Congenital Heart Disease Imaging: Comparison Across Three Dosing Regimens.1Cardiology, The University of Texas Southwestern Medical Center, Dallas, TX, United States
Synopsis
Keywords: Contrast Agents, Contrast Mechanisms, Ferumoxytol
Motivation: Ferumoxytol is becoming more widely used as a contrast agent, yet the optimum dose for use in cardiac MRI remains unknown.
Goal(s): To evaluate whether reducing the contrast dose to 2 or 1mg/kg will affect the image quality and diagnostic accuracy.
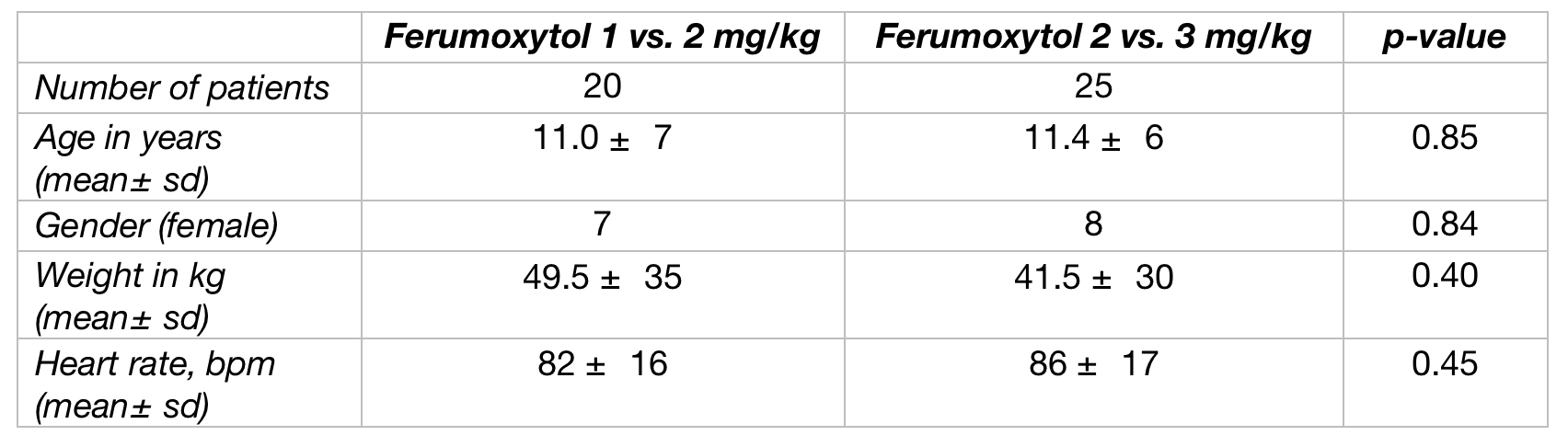
Approach: Forty-five patients with complex congenital heart disease had a 3D-IR-SSFP sequence performed at two different ferumoxytol doses. Twenty were in the ferumoxytol 1 vs. 2 mg/kg group, and twenty-five in the 2 vs. 3 mg/kg group.
Results: There was no significant difference in the RCA image quality score, RCA length, diagnostic accuracy nor CNR with the use of the reduced dosing.
Impact: Using reduced ferumoxytol dosing (1 or 2mg/kg), may lead to comparable image quality and diagnostic performance. The use of 2mg/kg lowers blood-T1 time to the extent that systolic imaging should not be precluded with the current 3D-IR Whole Heart Sequences.
Introduction
Ferumoxytol is a superparamagnetic iron oxide nanoparticle developed for iron replacement therapy. It is becoming more widely used as an off-label blood-pool contrast agent in pediatric cardiovascular disease1. Advantages to its use include the long intravascular half-life and its feasibility for use in patients with renal impairment2. The optimum dose for use in MR imaging is not known but commonly used between 3-5 mg/kg (IV) given over 15 minutes, as compared to the therapeutic dose for iron replacement of 8 mg/kg.Dasi et al. investigated the reduction of the contrast dose from 3 to 2 mg/kg, and found no statistical difference in signal-to-noise ratio with high qualitative scores for MRA and 4D flow across both groups3. However, the groups were separated and the comparison did not include direct image comparison within the same patient.
This study aims to compare image quality across three dosing regimens, down to 1mg/kg ferumoxytol dose. Additionally, images were obtained at two different doses, within the same cardiac MRI study for the same patient, allowing for a direct comparison. We hypothesized that reducing the contrast dose from 3 to 2 and even down to 1 mg/kg will not affect imaging quality (IQ) and diagnostic performance (DP) of three-dimensional (3D) Whole-Heart Congenital Disease imaging.
Methods
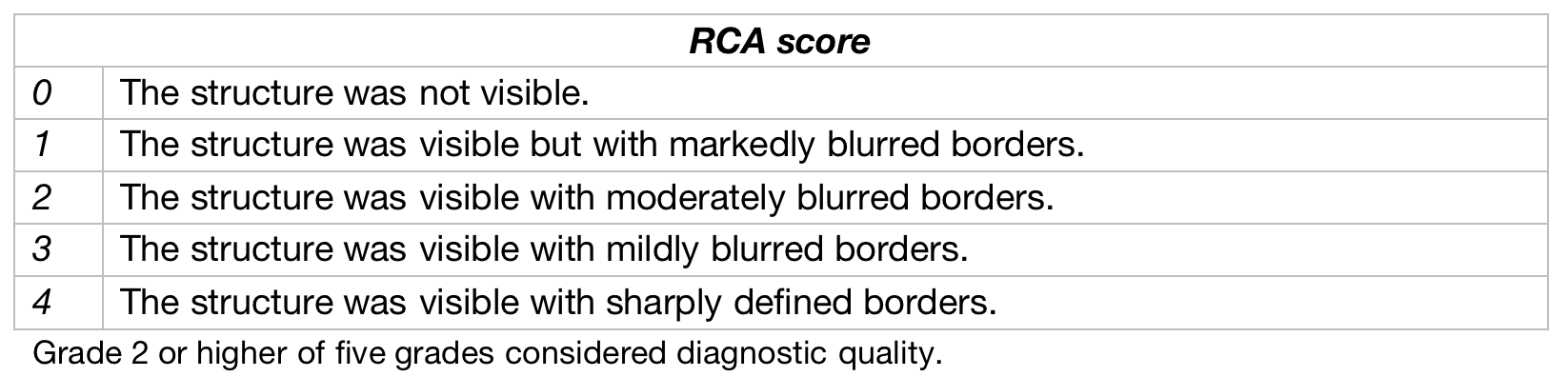
Forty-five patients with complex congenital heart disease were included. Each of those patients had imaging performed at two different ferumoxytol doses. Twenty patients were included in the ferumoxytol 1 vs. 2 mg/kg group, and twenty-five in the ferumoxytol 2 vs. 3 mg/kg group (Table 1). IQ and DP were compared amongst the images obtained at two different doses (1 vs. 2 and 2 vs. 3 mg/kg) using 3D inversion-recovery (IR) steady-state-free-precession (SSFP) sequence with respiratory navigator and EKG triggering. Sequence parameters included (FOV ~310 mm; Acquired resolution 1.4 to 1.8 mm3; Compressed Sense Factor 3.8-4.5; TE =1.8ms; TR=3.6ms). The optimum inversion time was chosen using a Look-Locker (LL) TI scout by choosing the image with the highest contrast between the blood and myocardium. Imaging was acquired during the end-systolic cardiac rest period determined using the reproducible method of velocity encoded mitral valve inflow cine4. Quantitative image quality was assessed by comparing contrast-to-noise ratios (CNR) and visualized RCA length. Qualitative image assessment was conducted by a five-point scoring scale (Table 2) applied to RCA images (Figure 1). Diagnostic performance was measured through the ability of each imaging method to reach complete diagnosis with the identification of all morphological segments including pulmonary veins and coronary arteries.Results
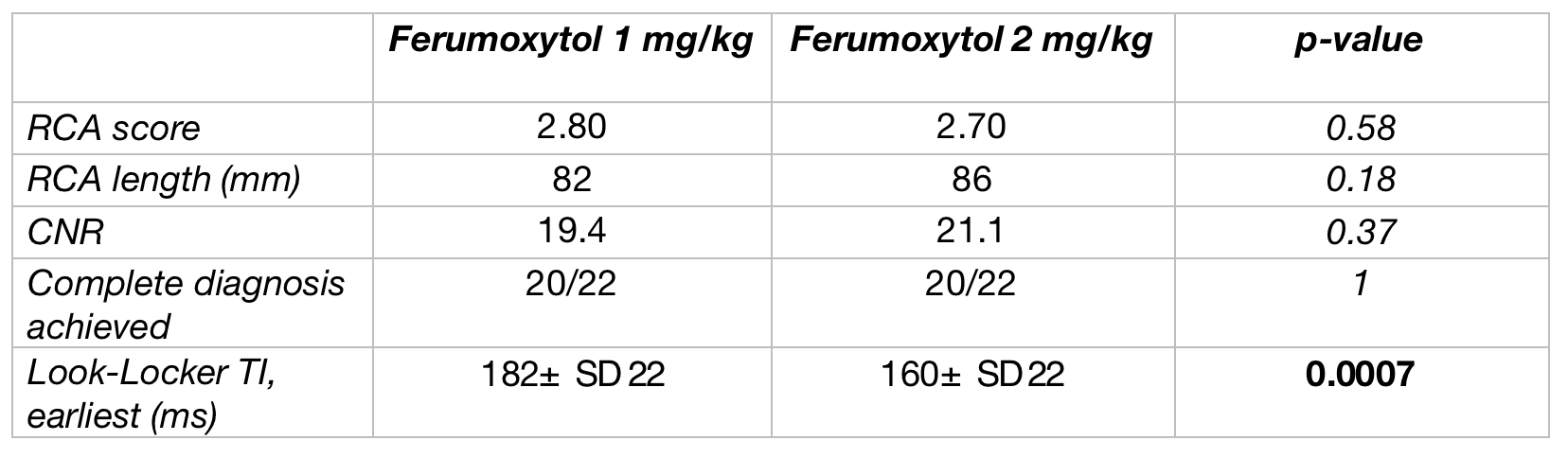
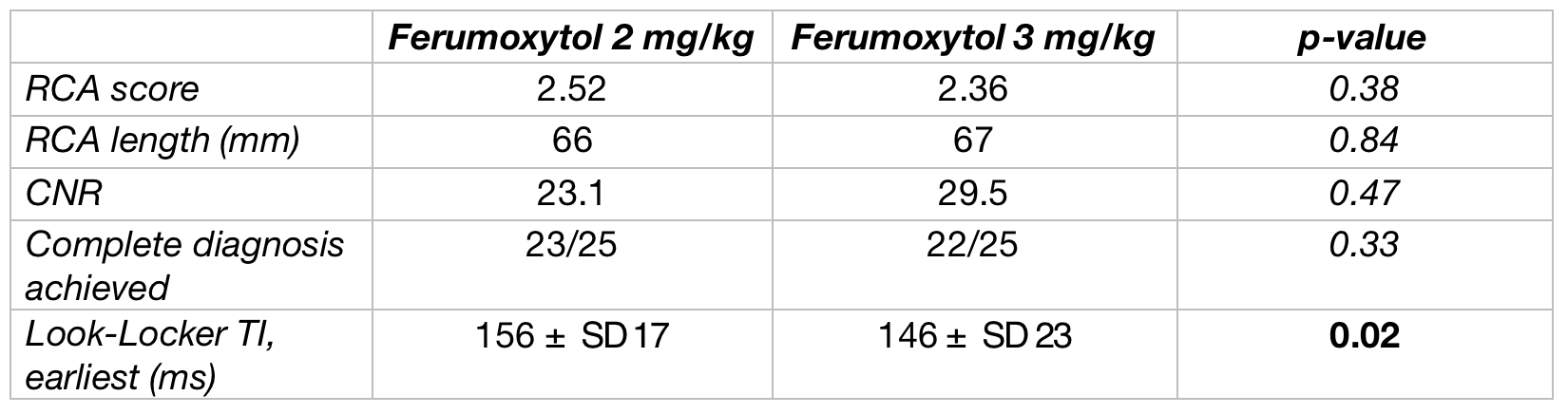
Using a reduced ferumoxytol dose produced comparable image quality and diagnostic performance. RCA score had no significant difference between doses; median=3, p=0.59 (1 vs. 2mg/kg), median=3, p=0.38 (2 vs. 3 mg/kg) using Wilcoxon signed rank test, and did not affect CNR (p=0.37 (1 vs. 2 mg/kg), p=0.47 (2 vs. 3 mg/kg) using paired t-test). The measured RCA length did not differ significantly. The mean RCA length was 82 vs. 86 mm for 1 vs. 2 mg/kg respectively (p=0.18), and 66 vs. 67 mm for 2 vs. 3 mg/kg respectively (p=0.84).The LL TI earliest times when the contrast between the blood and myocardium was first apparent, were between 135-212 ms with a mean of 182±SD 22 ms for 1 mg/kg vs. between 132-213 ms with a mean of 160±SD 22ms for the same patients at 2 mg/kg dose (significant difference; p=0.0007). The LL TI earliest times were between 111-187 ms with a mean of 156±SD 17 ms for 2 mg/kg vs. between 110-188 ms with a mean of 146±SD 23 ms for the same patients at 3 mg/kg dose (significant difference; p=0.02) (Table 3 & 4).
Discussion
Comparable image quality and diagnostic performance may be achievable with using a reduced ferumoxytol contrast dose down to 2 or 1mg/kg without affecting the CNR. This may be secondary to the reduction in occurrence of truncation artefact seen at lower doses of ferumoxytol. Infusing a lower dose can prevent unnecessary iron administration in patients and may allow for greater patient tolerance secondary to reduced reactions5.The earliest Look-locker time did not preclude systolic imaging at 2mg/kg. However, the upper limit of 95% confidence interval of the 1 mg/kg is above 220 ms which, according to clinical experience ,may interfere with the available systolic rest period for imaging.
Conclusion
The use of reduced ferumoxytol dose (1 or 2mg/kg), may lead to comparable image quality and diagnostic performance. The use of 2mg/kg lowers T1 time of blood to the extent that systolic imaging should not be precluded with the current 3D Inversion Recovery Whole Heart Sequences.Acknowledgements
No acknowledgement found.References
1.Toth GB, Varallyay CG, Horvath A et al. Current and potential imaging applications of ferumoxytol for magnetic resonance imaging. Kidney Int, 2017, 92:47–66.2.Kowalczyk, Mariusz, et al. “Ferumoxytol: A new era of iron deficiency anemia treatment for patients with chronic kidney disease.” Journal of Nephrology, vol. 24, no. 6, 2011, pp. 717–722, https://doi.org/10.5301/jn.5000025.
3.Dasi, Anoushka, et al. “Brand ferumoxytol vs. generic ferumoxytol comparison across two dosing regimens: A cardiac MRI image quality study.” Pediatric Radiology, 2023, https://doi.org/10.1007/s00247-023-05778-4.
4.Markus, Richard, et al. “Velocity encoded mitral valve inflow cine: A novel and more reproducible method to determine cardiac rest periods during coronary magnetic resonance angiography.” JRSM Cardiovascular Disease, vol. 11, 2022, p. 204800402210875, https://doi.org/10.1177/20480040221087556.
5.Lim, Wendy, et al. “Canadian expert consensus: Management of hypersensitivity reactions to intravenous iron in adults.” Vox Sanguinis, vol. 114, no. 4, 2019, pp. 363–373, https://doi.org/10.1111/vox.12773.
6.Dahl NV, Kaper RF, Strauss WE, Corvino FA, Zivkovic M. Cost-effectiveness analysis of intravenous ferumoxytol for the treatment of iron deficiency anemia in adult patients with non-dialysis-dependent chronic kidney disease in the USA. Clinico-econ Outcomes Res, 2017, 9:557–567.
Figures