3200
Analysis of Histogram Rescaling on Hyperpolarized 129Xe MRI Ventilation Distribution: A Deep Learning-Based Study of Trachea Segmentation1Medical Physics, Duke University, Durham, NC, United States, 2Duke University, Durham, NC, United States
Synopsis
Keywords: Hyperpolarized MR (Gas), Hyperpolarized MR (Gas)
Motivation: Hyperpolarized 129Xe MRI, pivotal for lung function analysis, faces challenges in standardizing ventilation distribution calculations, particularly regarding image rescaling and major airway inclusion.
Goal(s): To develop a deep learning-based method to segment the trachea and assess its impact on the ventilation distribution.
Approach: We trained and compared various deep learning models for robust segmentation.
Results: In patients with interstitial lung disease, the ratio of 129Xe signal in the trachea versus the distal lung is 2.5-fold higher than in healthy volunteers. If such signal is not segmented out before histogram rescaling, ventilation distributions may be substantially skewed in patients with restrictive disease.
Impact: This research paves the way for redefining the calculation of ventilation distribution in pulmonary imaging by incorporating large airways like the trachea, potentially leading to more precise imaging metrics and improved clinical outcomes for pulmonary diseases.
Introduction
Hyperpolarized 129Xe MRI has emerged as a powerful tool for comprehensive pulmonary functional imaging[1, 2]. However, quantifying pulmonary ventilation requires rescaling the 129Xe intensity histogram. This can be strongly affected by residual signal in the trachea, which can be enhanced in patients with interstitial lung disease (ILD) whose restrictive disease can lead to incomplete inhalation[3]. While trachea signal can be manually segmented out, this is labor-intensive and suffers from inter-observer variability. Deep learning offers a solution that overcomes the limitations of manual segmentation and thresholding techniques, which may not adequately differentiate between the trachea and adjacent structures or adapt to the variable signal intensities found. Although deep learning techniques have been increasingly employed in thoracic cavity volume (TCV) segmentation and exhibit commendable accuracy[4-6], such approaches have not been applied to segmenting the trachea. Here, we introduce a deep learning-based approach tailored for trachea segmentation. We then apply it to compute the trachea-to-TCV gas ratio and reveal the impact on its inclusion in rescaling the ventilation distribution.Methods
1. Imaging methodology and dataset generation: All subjects underwent 129Xe gas exchange MRI in accordance with consortium-recommended protocols[7]. Images were reconstructed using a fixed kernel sharpness and then manually labeled by an expert reader (Figure 1). Models were trained, validated, and tested on 95 images from across disease conditions. The resulting segmentations were used to calculate the trachea-to-TCV gas ratio in a separate cohort of 15 healthy subjects and 15 subjects with ILD.2. Training details and model architecture
We employed a 3D V-Net[8], 3D U-Net[9], and modified 3D DenseNet[10] architectures, known for their efficacy in biomedical image segmentation. The model was trained using the Adam optimizer[11] using the PyTorch framework on a single RTX 3090 GPU using the dice loss. The set of 95 images was split into a training-validation-testing set of 55, 20, and 20 images respectively. Data augmentation techniques, including random rotations, elastic deformations, and bias field variations, were applied to prevent overfitting. Input images were normalized to be between 0 and 1. We trained the model for 100 epochs, a batch size of 4, and a learning rate of 10-4. https://github.com/junlanlu/xenon-segmentation.
Results
The modified 3D DenseNet architecture outperformed the other models for segmenting the trachea, achieving a Dice similarity coefficient (DSC) of 0.618, a Matthews correlation coefficient (MCC) of 0.593, and a sensitivity of 0.779 (Figure 2). These metrics suggest that the model has a high true positive rate and achieved a moderate agreement between the automated segmentation and the ground truth.The application of our segmentation model revealed significant differences in the trachea-to-TCV gas ratio between healthy subjects and those with ILD. Specifically, the ratio was found to be 2.5 times higher in participants with ILD compared to healthy participants (p<0.001, Figure 3). We found that when tracheal signal was retained in the analysis of the ventilation distribution, resulting values changed significantly. In one illustrative case of a participant with ILD, the mean ventilation and defect percentage was calculated to be 0.59 and 2.2% respectively when excluding tracheal signal from rescaling, but dramatically changed to 0.24 and 25.8% when it was included (Figure 4).
Discussion
Deep learning methods for identifying and excluding tracheal signal may prove useful in improving the robustness of the recovered ventilation distribution in 129Xe MRI images. The superior performance of the modified 3D DenseNet model in trachea segmentation is likely attributable to its additional skip connections to capture complex features and patterns within the imaging data. Although the segmentation accuracy metrics only demonstrate moderate performance, this may be partly due to noisy training data along with inherent challenges of manually delineating such a small volume. Nevertheless, the ability to discern and segment the trachea with reasonable accuracy is a significant step toward more reliable and reproducible ventilation analysis.The observed differences in the trachea-to-TCV gas ratio between healthy and ILD subjects could serve as a marker to identify patients with a restrictive aspect of their disease. Moreover, the dramatic shift in both mean ventilation and defect percentage upon the inclusion of tracheal gas in the analysis is notable. This exemplifies the critical role of not only accurate segmentation but also the need for standardized methods for scaling the distribution.
Acknowledgements
R01HL105643, R01HL153872, NSF GRFP DGE-2139754References
1. Wang, Z., et al., Diverse cardiopulmonary diseases are associated with distinct xenon magnetic resonance imaging signatures. Eur Respir J, 2019. 54(6).
2. Ebner, L., et al., The role of hyperpolarized (129)xenon in MR imaging of pulmonary function. Eur J Radiol, 2017. 86: p. 343-352.
3. Selman, M., T.E. King, and A. Pardo, Idiopathic Pulmonary Fibrosis: Prevailing and Evolving Hypotheses about Its Pathogenesis and Implications for Therapy. Annals of Internal Medicine, 2001. 134(2): p. 136-151.
4. Astley, J.R., et al., Large-scale investigation of deep learning approaches for ventilated lung segmentation using multi-nuclear hyperpolarized gas MRI. Sci Rep, 2022. 12(1): p. 10566.
5. Tustison, N.J., et al., Convolutional Neural Networks with Template-Based Data Augmentation for Functional Lung Image Quantification. Acad Radiol, 2019. 26(3): p. 412-423.
6. Leewiwatwong, S., et al. Ventilation Defect Synthesis in Hyperpolarized 129Xe Ventilation MRI to Accelerate Training of Segmentation Models. in ISMRM. 2022.
7. Niedbalski, P.J., et al., Protocols for multi-site trials using hyperpolarized (129) Xe MRI for imaging of ventilation, alveolar-airspace size, and gas exchange: A position paper from the (129) Xe MRI clinical trials consortium. Magn Reson Med, 2021. 86(6): p. 2966-2986.
8. Milletari, F., N. Navab, and S.-A. Ahmadi, V-Net: Fully Convolutional Neural Networks for Volumetric Medical Image Segmentation, in 2016 Fourth International Conference on 3D Vision (3DV). 2016. p. 565-571.
9. Çiçek, Ö., et al. 3D U-Net: Learning Dense Volumetric Segmentation from Sparse Annotation. in Medical Image Computing and Computer-Assisted Intervention – MICCAI 2016. 2016. Cham: Springer International Publishing.
10. Bui, T.D., J. Shin, and T. Moon, Skip-connected 3D DenseNet for volumetric infant brain MRI segmentation. Biomedical Signal Processing and Control, 2019. 54: p. 101613.
11. Kingma, D.P. and J. Ba, Adam: A Method for Stochastic Optimization. 2015.
Figures
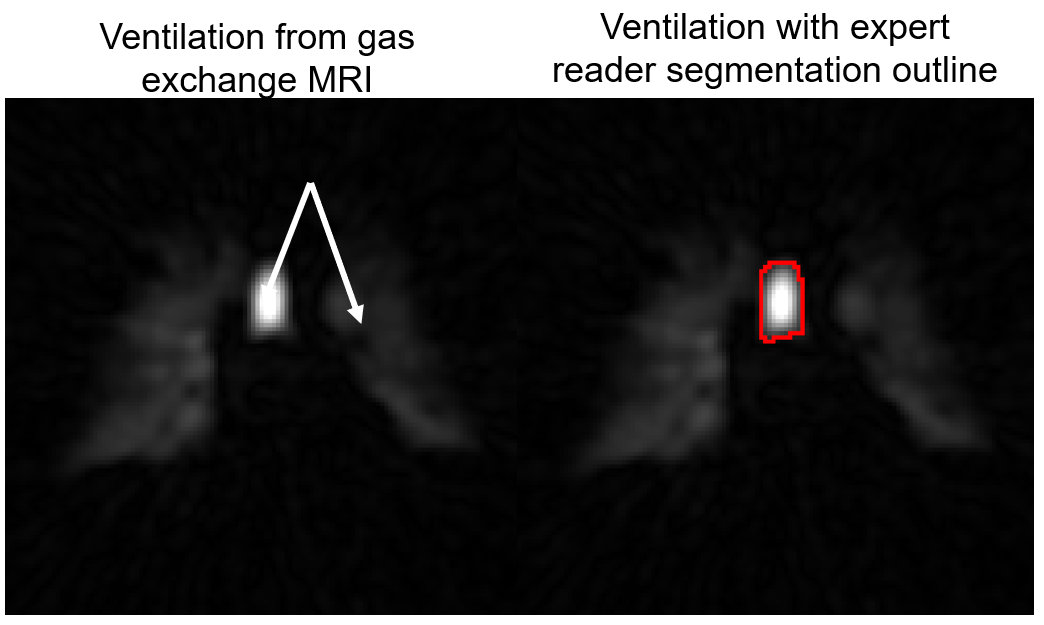
Figure 1: Gas-phase 129Xe MRI slice highlighting significant tracheal gas signal, with expert manual segmentation overlaid to demarcate tracheal boundaries.
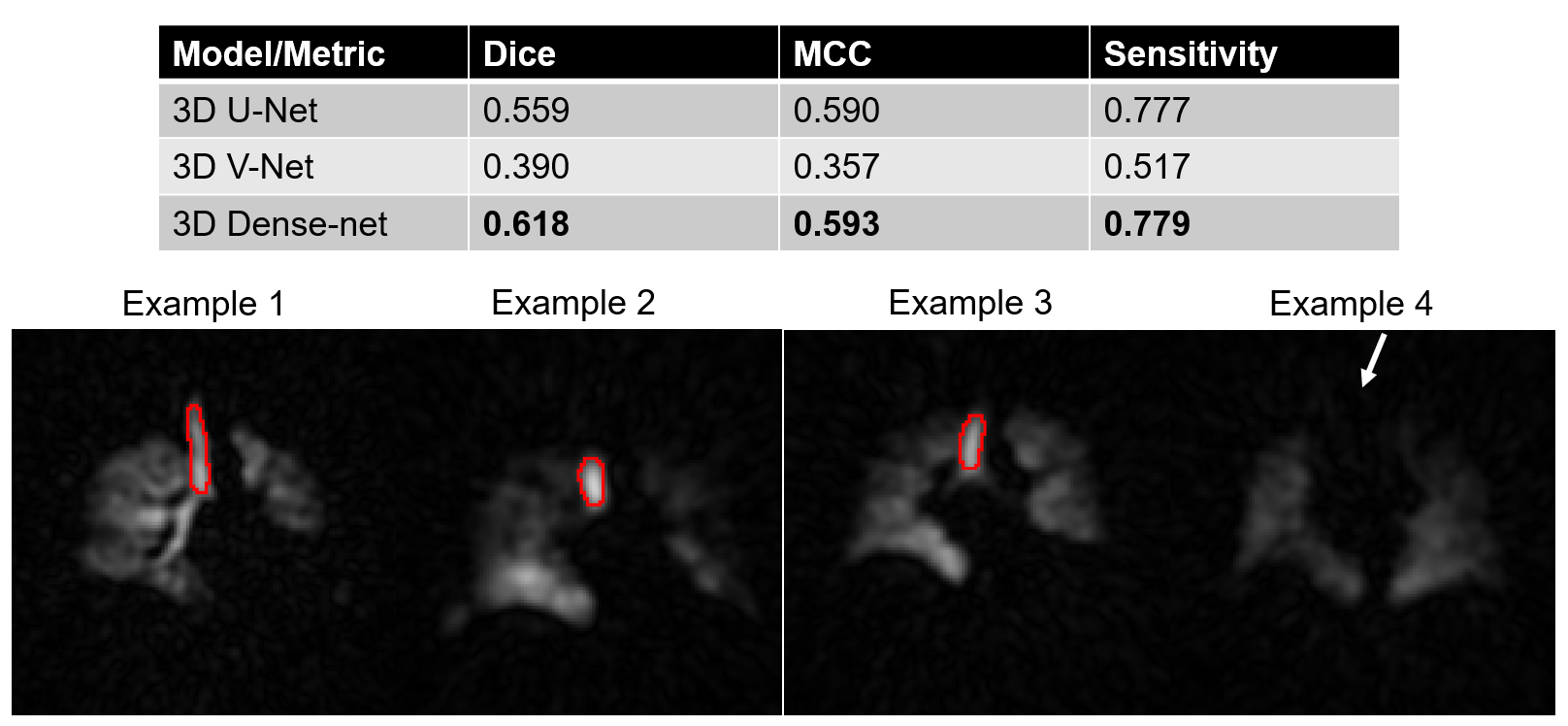
Figure 2: Comparative performance metrics for deep learning models with representative segmentations across four subjects using the modified 3D Dense-net model. Notably, the model demonstrates high accuracy in cases with clear tracheal gas signal but fails in images lacking such signal, such as example 4.
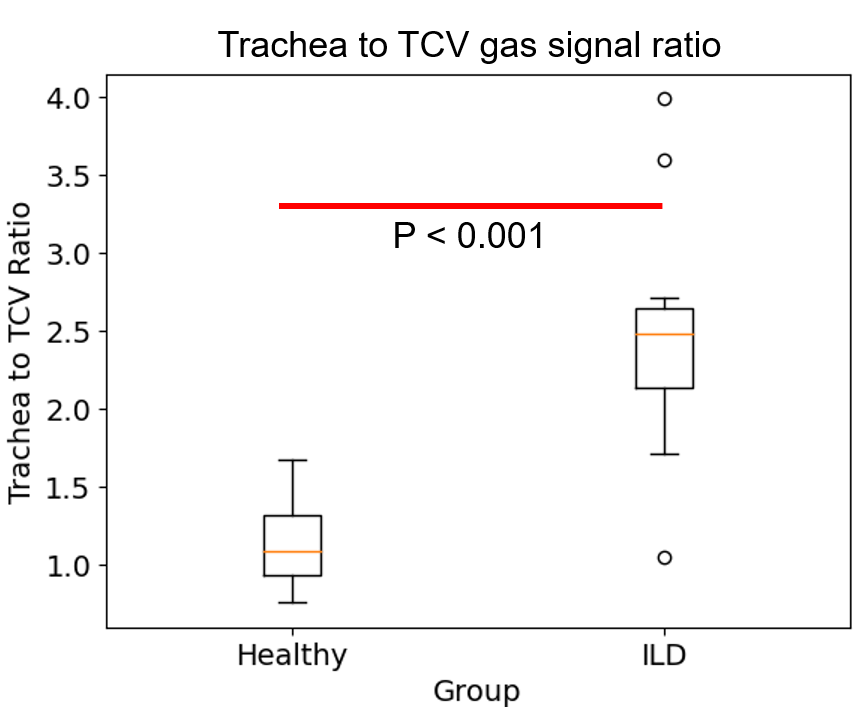
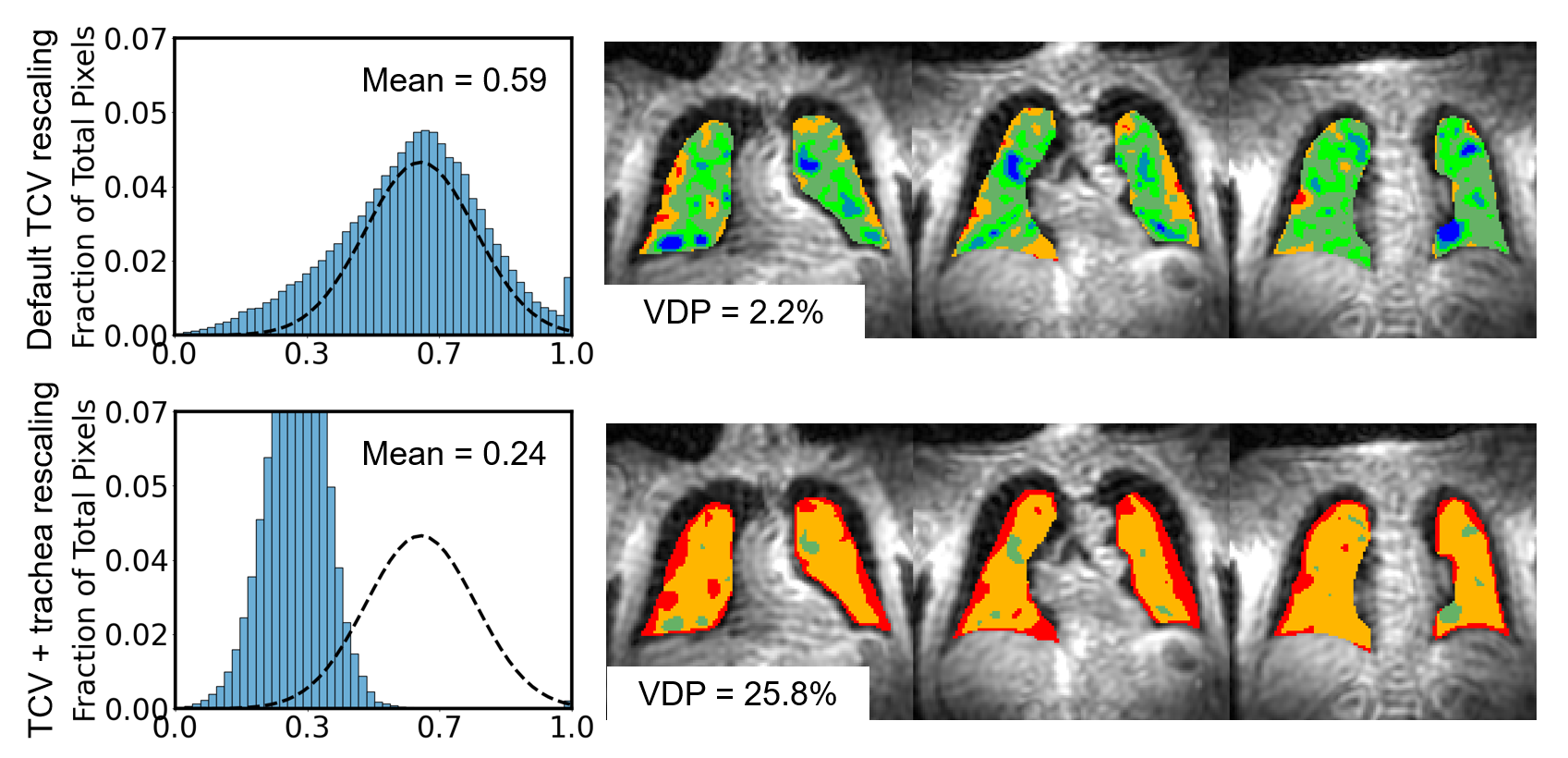
Figure 4: Ventilation histograms and representative binning maps in a participant with ILD, when top percentile rescaling is done including the trachea vs excluding it. Inclusion of tracheal segmentation markedly decreases the histogram mean and increases the apparent VDP.