3198
Hyperoxic challenge combined with hyperpolarized 129-xenon dissolved-phase imaging in a porcine model of pulmonary embolism1MR Research Centre, Aarhus University, Aarhus, Denmark, 2GE HealthCare, Brøndby, Denmark, 3GE HealthCare, Munich, Germany, 4Aarhus University, Aarhus N, Denmark, 5The Department of Cardiological Medicine B, Aarhus University, Aarhus N, Denmark, 6POLARIS group, University of Sheffield, Sheffield, United Kingdom
Synopsis
Keywords: Hyperpolarized MR (Gas), Hyperpolarized MR (Gas)
Motivation: Pulmonary embolism (PE) is a leading cause of cardiovascular death. Timely diagnosis is crucial but challenging. Increasing inspired oxygen levels to 40% or above has proven an effective treatment in acute PE by altering pulmonary gas exchange.
Goal(s): Our goal is to determine if hyperpolarized 129-xenon gas can diagnose PE.
Approach: Hyperpolarized 129-xenon dissolved-phase imaging was evaluated by applying a hyperoxic challenge in a porcine PE model.
Results: Whole lung assessment of dissolved-phase imaging indicates regional pulmonary gas exchange increases with higher inhaled oxygen levels. Nevertheless, hyperoxic challenge effects did not diagnose PE.
Impact: The study shows great potential of a pulmonary gas exchange imaging with the application of dissolved-phase hyperpolarized 129Xe imaging throughout a hyperoxic challenge. Nevertheless, the method did not improve diagnosis of pulmonary embolism in our porcine animal model.
Introduction
Pulmonary embolism (PE) is a leading cause of cardiovascular death surpassed only by heart attack and stroke 1.Timely diagnosis is crucial, but challenging, as the clinical presentation of PE is unspecific and easily mistaken for other common medical emergencies. Optimal pulmonary gas exchange is vital in detecting acute PE.Hyperpolarized xenon-129 (129Xe) dissolved-phase imaging is sensitive to gas exchange and blood oxygenation 2–4. Oxygen is a potent vasodilator lowering pulmonary vascular resistance and is proven as effective treatment in acute PE at inspired oxygen levels (FiO2) of 40% or above 5,6. Previous studies evaluated reduction in blood oxygen saturation caused by apnea 4. Consequently, changes in gas transfer when increasing FiO2 above normal conditions (21% oxygen) may serve as a pulmonary disease indicator. Given the clinical treatment option for PE the diagnostic capabilities of dissolved-phase imaging may furthermore be improved by introduction of a hyperoxic challenge.
The porcine anatomy provides an opportunity to regulate and investigate physiological effects of oxygen gas transfer in PE 5. Improving feasibility of method developments for detection of pulmonary defects and effects of oxygen treatment in PE.
The aim of this study was to investigate dissolved-phase 129Xe imaging in detection of pulmonary defects in porcine lungs with embolisms using a hyperoxic challenge at inhaled oxygen levels of 40% and 100%.
Methods
For all experiments 129Xe gas was polarised using SEOP with a custom-built polariser (POLARIS, University of Sheffield). The gas mixture (3% enriched xenon, 10% N2, 87% He) was dispensed into a 1000 ml Tedlar bag and administered following a 1-2min walk to the MRI scanner. Xenon images were acquired on a 3T MRI scanner (MR750, GE Healthcare, Waukesha, WI, USA) using a 129Xe transmit-receive quadrature vest coil (Clinical MR Solutions, Brookfield, WI, USA) tuned to 35.3MHz.Dissolved-phase imaging was acquired with a 3D Cartesian CSI with a matrix size of 28x28x6 covering a field-of-view of 40x40x20 cm3. A spectrally tailored RF pulse with a duration of 1.2 ms and partial self-refocusing was designed to excite the dissolved and gas phases with flip angles of 10˚ and 0.1˚ and passbands of 500 Hz and 200 Hz, respectively 7. Repetition time was 7.4 ms resulting in a total acquisition time of 18 s. Cardiac and large pulmonary vessels dissolved xenon signal was saturated with 20 pulses with a flip angle of 30˚. Data was spectrally zero-filled to 256 samples at a bandwidth of 20 kHz and spatially zero-filled by a factor of 2.
The study included 8 pigs (4 healthy and 4 with pulmonary embolies) weighing 40 and 60 kg, respectively. Embolies was induced by drawing blood (180 ml) from a venous access divided into six non-heparin coated plastic tubes. The tubes are hung vertically for three hours to clot and form autologous emboli before injection. The anesthetized pigs were put on a mechanical ventilator at FiO2 of 40% and 100% during the scan session.
Results
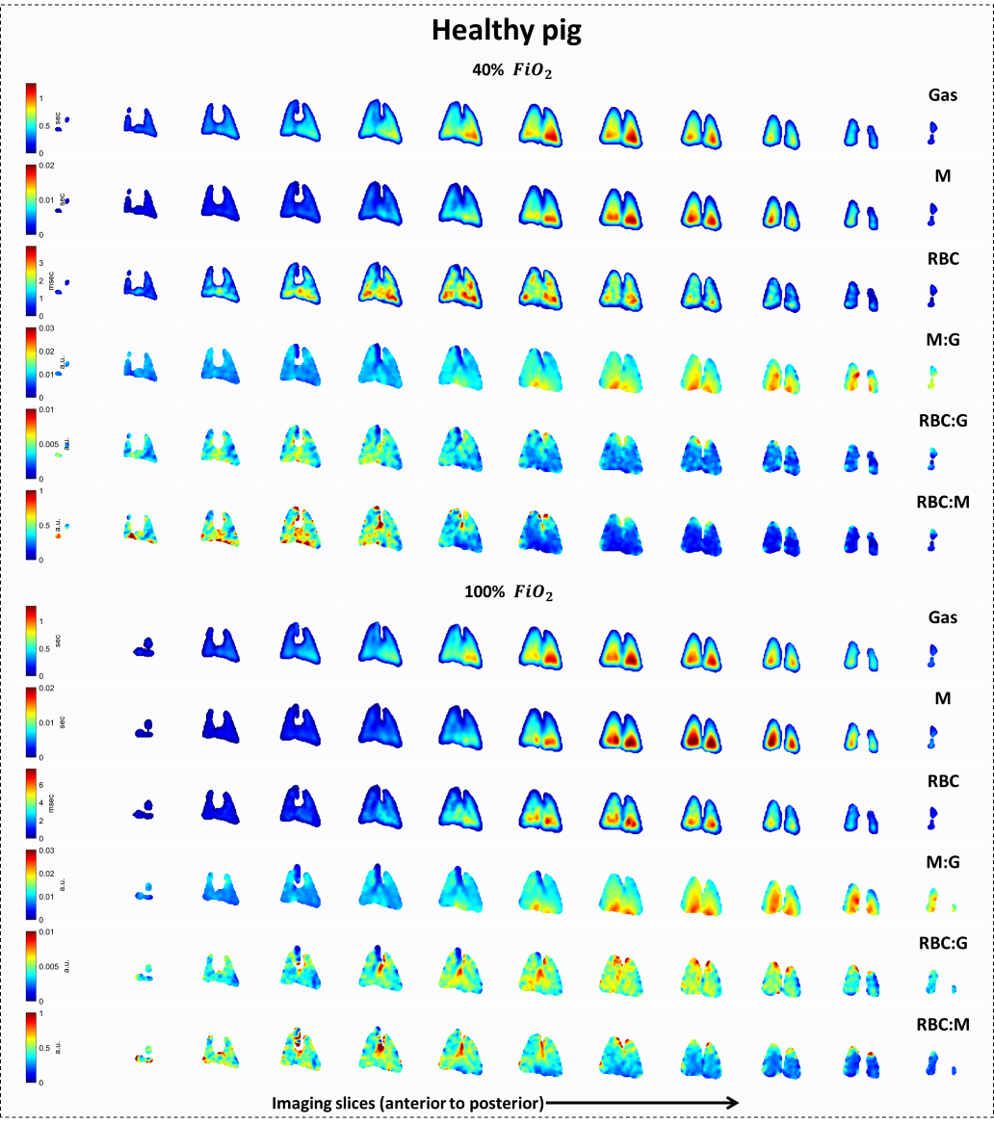
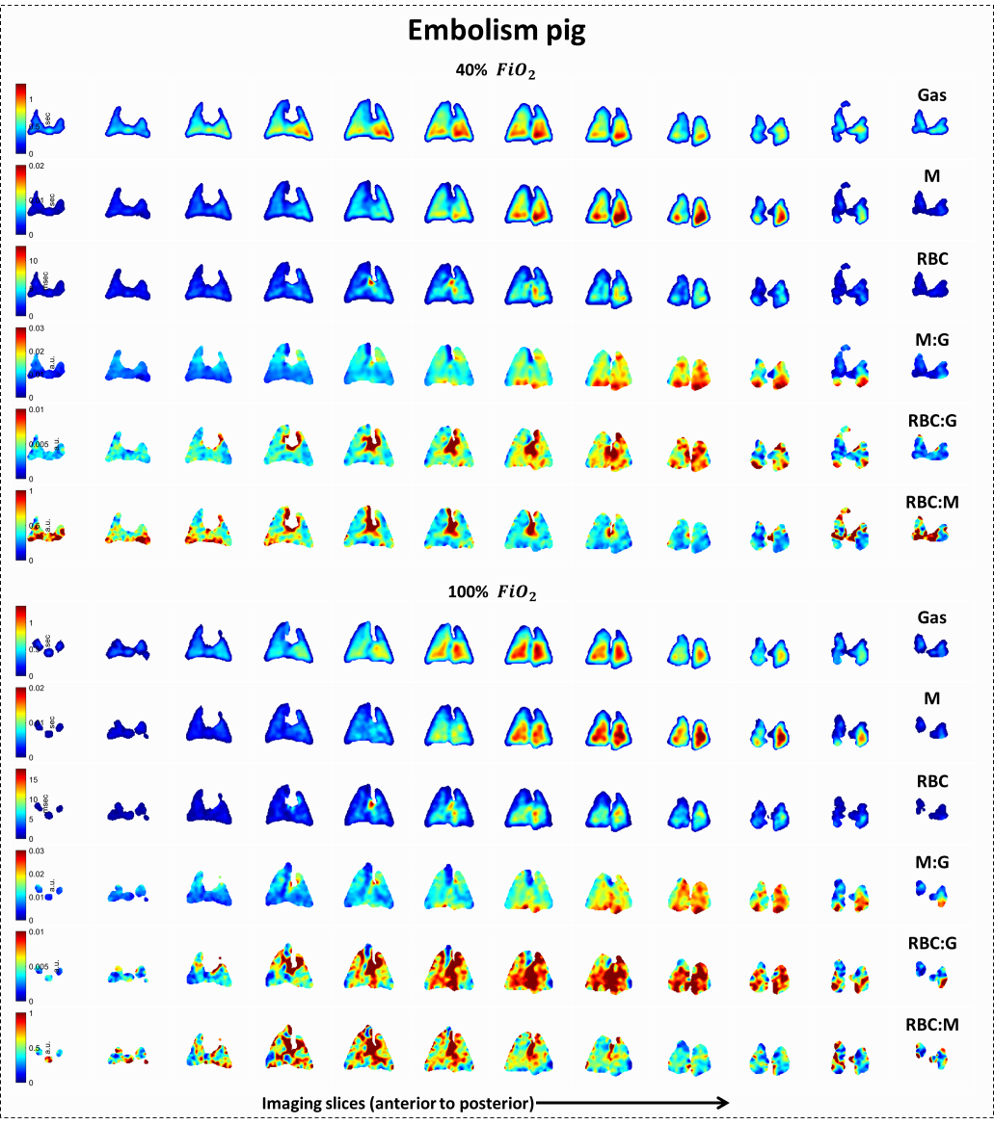
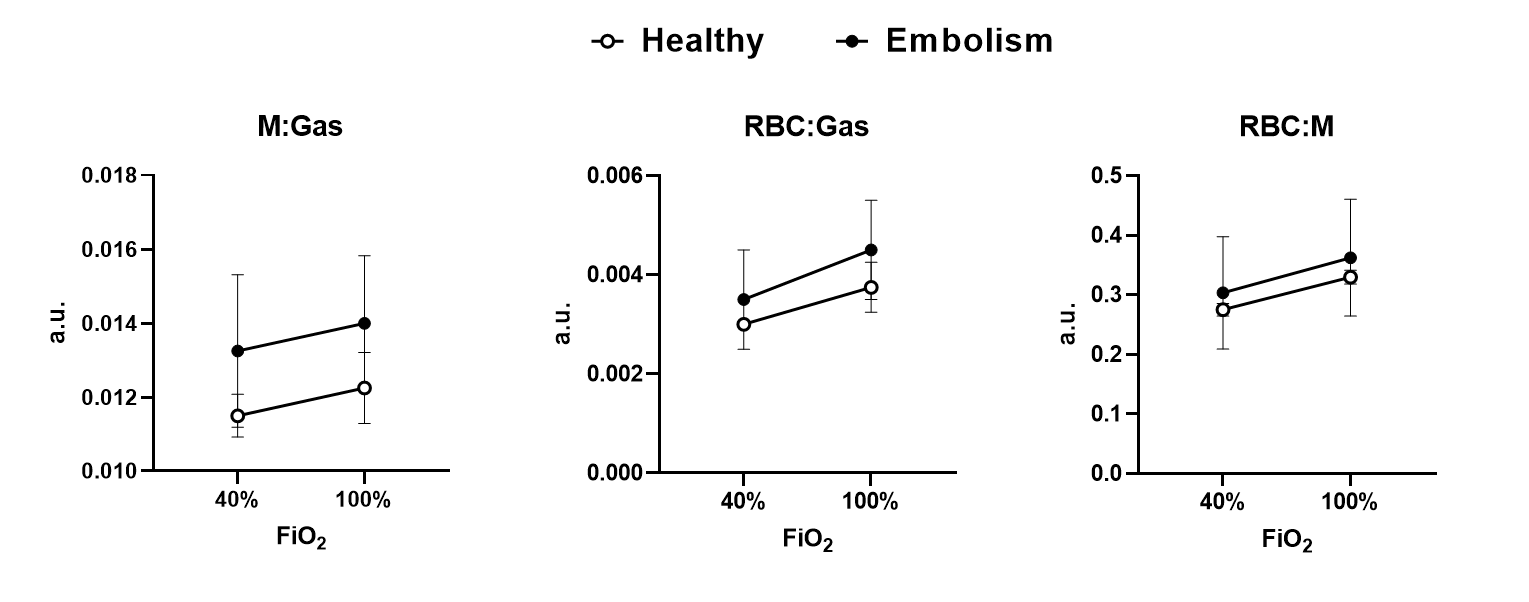
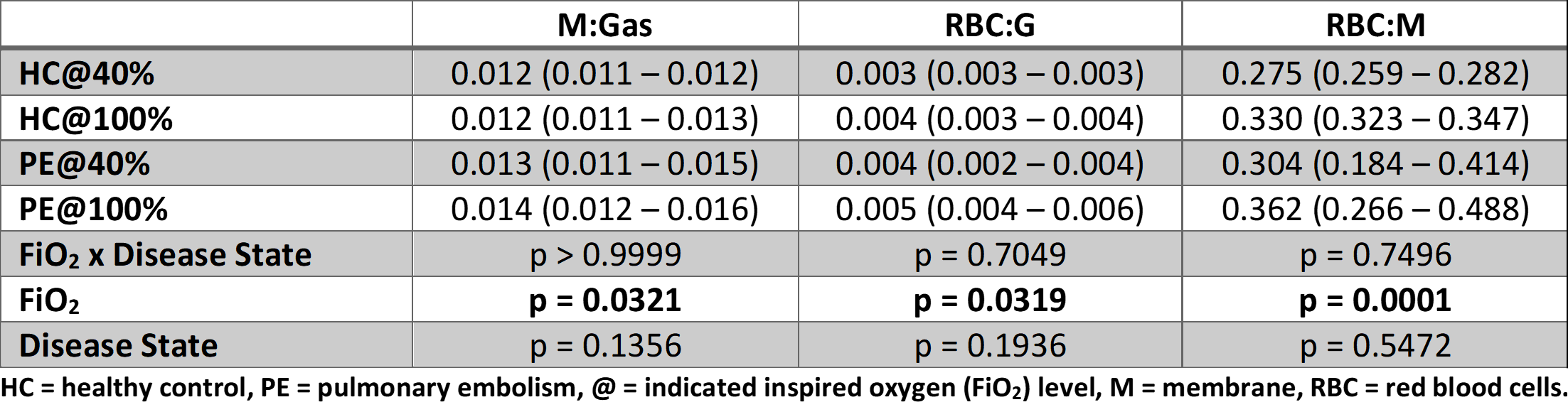
Dissolved-phase gas, membrane (M), and red blood cells (RBC) signal ratios (Fig. 1 + Fig. 2) were evaluated in two-way ANOVA analysis (Fig. 3 + Table 1) grouped by disease state (healthy (HC) vs emboli (PE)) and FiO2 (40% vs 100%) as repeated measure. Results indicate differences in oxygen levels M:Gas (p = 0.0321), RBC:Gas (p = 0.0319) and RBC:M (p < 0.0001) unaffected by disease state and effects of the oxygen challenge between disease state groups (FiO2 x Disease State).Discussion
An increase in gas exchange from gas to membrane and red blood cells was observed in healthy and in pigs with pulmonary embolism when increasing FiO2 from 40% and 100%. Nevertheless, when evaluating the hyperoxic oxygen challenge as a measure to determine disease state no significant differences were established.Dissolved-phase sensitivity to oxygen saturation levels has previously been described in detail via apnea. Nevertheless, apnea is an extreme condition where oxygen saturation is lowered past normal conditions and the reverse effect of increased FiO2 during normal blood oxygen saturation values (sO2 ~ 100%) has not been evaluated. Increasing FiO2 above 40% is a common treatment option of PE. In our study we only used whole lung measures to evaluate the hyperoxic challenge of 40% and 100% FiO2. Further analysis should include regional measures with confirmed embolism positioning to validate possible differences.
Conclusion
Whole lung assessments of the dissolved-phase hyperoxic challenge was not indicative of pulmonary embolism. Further regional analyses will evaluate if hyperoxic challenge can be used to differentiate focal PE pathology.Acknowledgements
The authors would like to thank radiographer Tau Vendelboe for contributing to scanning of the subjects.References
1. Wendelboe AM, Raskob GE. Global Burden of Thrombosis. Circ Res. 2016;118(9):1340-1347. doi:10.1161/CIRCRESAHA.115.306841
2. Wolber J, Cherubini A, Leach MO, Bifone A. Hyperpolarized 129Xe NMR as a probe for blood oxygenation. Magn Reson Med. 2000;43(4):491-496. doi:10.1002/(SICI)1522-2594(200004)43:4<491::AID-MRM1>3.0.CO;2-6
3. Wolber J, Cherubini A, Leach MO, Bifone A. On the oxygenation‐dependent 129Xe T 1 in blood. NMR Biomed. 2000;13(4):234-237. doi:10.1002/1099-1492(200006)13:4<234::aid-nbm632>3.3.co;2-b
4. Norquay G, Leung G, Stewart NJ, Wolber J, Wild JM. 129Xe chemical shift in human blood and pulmonary blood oxygenation measurement in humans using hyperpolarized 129Xe NMR. Magn Reson Med. 2017;77(4):1399-1408. doi:10.1002/mrm.26225
5. Schultz J, Andersen A, Gade IL, Ringgaard S, Kjaergaard B, Nielsen-Kudsk JE. A porcine in-vivo model of acute pulmonary embolism. Pulm Circ. 2018;8(1). doi:10.1177/2045893217738217
6. Lyhne MD, Hansen JV, Dragsbæk SJ, Mortensen CS, Nielsen-Kudsk JE, Andersen A. Oxygen Therapy Lowers Right Ventricular Afterload in Experimental Acute Pulmonary Embolism. Crit Care Med. 2021;49(9):e891-e901. doi:10.1097/CCM.0000000000005057
7. Collier GJ, Schulte RF, Rao M, Norquay G, Ball J, Wild JM. Imaging gas‐exchange lung function and brain tissue uptake of hyperpolarized 129Xe using sampling density‐weighted MRSI. Magn Reson Med. 2023;89(6):2217-2226. doi:10.1002/mrm.29602
Figures