3190
129Xe MR Spectroscopy reveals Abnormal Gas-exchange in Moderate and Severe Asthma1Western University, London, ON, Canada
Synopsis
Keywords: Hyperpolarized MR (Gas), Hyperpolarized MR (Gas), Lung, Asthma, Spectroscopy
Motivation: Airways disease in asthma is characterized by airway wall thickening, luminal obstruction and smooth muscle hyper-responsiveness. Abnormal CT pulmonary vascular pruning has also been reported. We wondered if 129Xe MRS could identify functional abnormalities related to the pulmonary vascular tree, via the measurement of gas-exchange across the alveolar-capillary membranes, into the red-blood-cells.
Goal(s): Measure and compare 129Xe MRS RBC:membrane in healthy volunteers, and patients with moderate or severe asthma.
Approach: 129Xe MRI, MRS and pulmonary function measures were acquired in healthy-volunteers and asthma participants.
Results: 129Xe MR RBC:membrane was significantly different in healthy-volunteers, moderate and severe asthma.
Impact: To our knowledge, this is the first demonstration of significantly different 129Xe MRS RBC:membrane values in healthy volunteers, and patients with moderate or severe asthma. Abnormal pulmonary gas-exchange may play a role in asthma, regardless of disease-severity.
INTRODUCTION:
Asthma is typically characterized by airway abnormalities,1,2 including inflammation, smooth muscle hyper-responsiveness and occlusions. Abnormal alveolar collagen deposits have also been described in poorly-controlled asthma, suggesting that inflammation may extend beyond the airways.3 Previous work also demonstrated pulmonary vascular remodeling in severe asthma,4 but it remains poorly understood.Hyperpolarized 129Xe MRI provides a way to quantify inhaled gas distribution (ventilation) as well as transmembrane diffusion (perfusion) into the alveolar-capillary interface and the red-blood-cells (RBC) via MR spectroscopy (MRS).5 Preliminary investigations using 129Xe MRS measurements identified gas-exchange abnormalities in chronic lung disease.6 Until now, these measurements have not yet been investigated in patients with mild or moderate asthma. Hence, here we aimed to acquire 129Xe MRS gas-exchange measurements in patients with moderate and severe asthma for direct comparison and with the same measurements in healthy volunteers.
METHODS:
Study Participants:We evaluated participants without chronic lung disease (n=24) and participants with asthma (n=45), who provided written informed consent to spirometry7 and 129Xe MRI/MRS. Participants with asthma were classified by Global Initiative for Asthma (GINA) report.8
MRI Acquisition:
Anatomical 1H and hyperpolarized 129Xe MRI/MRS were acquired using a whole-body 3T Discovery MR750 (GE Healthcare, Milwaukee, USA) with broadband imaging capabilities and a whole-body radiofrequency coil, as previously described.9-11 Anatomical 1H images were acquired using a fast-spoiled gradient-recalled echo (FGRE) sequence with a partial-echo (total acquisition time=8s; TR msec/TE msec=4.7/1.2; flip-angle=30°; FOV=40×40cm2; bandwidth=24.4kHz; 128×80 matrix, zero-padded to 128×128; partial echo percentage=62.5%; 15-17 slices; slice thickness=15mm; no gap). Static ventilation images were acquired using a three-dimensional FGRE sequence (total acquisition time=14s; TR msec/TE msec=6.7/1.5; variable flip-angle; FOV=40×40cm2; bandwidth=15.63kHz; 128×128 matrix, zero-padded to 128×128; 14 slices; slice thickness, 15mm; no gap). 129Xe MRS was acquired using a whole-lung free-induction-decay spectroscopy sequence (200 dissolved-phase spectra, TR msec/TE msec=15/0.7, flip-angle=40°, BW=31.25kHz, 600μs 3-lobe Shinnar-Le Roux pulse). Participants were instructed to inhale and hold 1.0L of gas (100% N2 for anatomical scan; 400mL hyperpolarized 129Xe + 600mL 4He for static ventilation; 200mL hyperpolarized 129Xe + 800mL 4He for spectroscopy).
Data Analysis:
MRS peaks were fit to a three-component Lorentzian model in MATLAB (2021b, Mathworks) to determine component full-width half maximum, phase, and frequency. RBC:membrane ratio was calculated as the ratio of RBC area-under-the-curve and membrane area-under-the-curve. MRI data reconstruction was performed by re-gridding radial k-space data to a Cartesian representation (kernel sharpness=0.32, over-gridding=3).12 Receiver phase-offset and local phase inhomogeneity were corrected.13 Intergroup differences were evaluated using analysis-of-variance (ANOVA) and univariate relationships were determined using Spearman (ρ) correlations. Results were considered statistically significant when the probability of making a type I error was less than 5% (p<.05).
RESULTS:
Table 1 provides demographic and imaging measurements for healthy volunteers (n=24), moderate (GINA-4, n=27), and severe (GINA-5, n=18) asthma. There were significant differences (p<.05) between the three subgroups in all measurements, except for blood eosinophil count and MRS membrane:gas ratio. There was a difference between GINA-4 and GINA-5 participants for RBC:membrane (p=.048). As shown in Figure 1, in healthy volunteers, RBC:membrane correlated with FEV1 (ρ=.63, p=.001), forced-vital-capacity (FVC; ρ=.62, p=.001), body-mass-index (BMI; ρ=.49, p=.04) and diffusing-capacity-of-the-lungs-for-carbon-monoxide (DLCO; ρ=.80, p<.001). In GINA-4 asthma, (Figure 2) RBC:membrane was correlated with FEV1/FVC (ρ=-.36, p=.04) and age (ρ=-.50, p=.005), and in GINA-5 with FVC (ρ=.48, p=.047) (Figure 3).DISCUSSION:
129Xe MRS measurements of alveolar gas-exchange were significantly different between healthy volunteers, moderate and severe asthma patients. RBC:membrane ratio was the only measurement that was different between asthma participants when grouped by GINA steps. The interpretability of RBC:membrane can be challenging, due to abnormalities in either the RBC or membrane compartment contributing to an impaired ratio. However, these differences appeared to be driven by RBC abnormalities, as there was no difference in membrane:gas signal between groups.The RBC:membrane ratio is believed to sensitively reflect abnormal gas-exchange,14 where abnormally low RBC:membrane has been reported in non-specific interstitial pneumonia,15 and was related to FVC in idiopathic pulmonary fibrosis.16 We extend these findings to asthma patients, where RBC:membrane was abnormally low and correlated with global measurements of airflow obstruction (FEV1, FVC, and FEV1/FVC) in asthma patients.
129Xe MRS provides sensitive measurements to interrogate individual components of the alveolar gas-exchange process and better understand the underlying pathophysiology that may drive symptoms and outcomes in patients with asthma.
CONCLUSIONS:
To our knowledge, this is the first demonstration of differences in 129Xe MRS gas-exchange measurements between healthy volunteers, mild-moderate and severe asthma. These 129Xe MRS findings agree with previous work suggesting pulmonary vascular remodeling in asthma.4 Thus, abnormal pulmonary gas-exchange may play a role in asthma regardless of GINA disease classification.Acknowledgements
No acknowledgement found.References
1 Dunican, E. M. et al. J Clin Invest (2018).
2 Park, J. W. et al. J Investig Allergol Clin Immunol (1997).
3 Weitoft, M. et al. Respir Res (2014).
4 Ash, S. Y. et al. Am J Respir Crit Care Med (2018).
5 Kaushik, S. S. et al. J Appl Physiol (2013).
6 Wang, Z. et al. Eur Respir J (2019).
7 Miller, M. R. et al. Eur.Respir.J. (2005).
8 Bateman, E. D. et al. Eur.Respir.J (2008).
9 Parraga, G. et al. Invest Radiol (2007).
10 Svenningsen, S. et al. J Magn Reson Imaging (2013).
11 Matheson, A. M. et al. Radiology (2022).
12 Robertson, S. H. et al. Concepts in Magnetic Resonance Part A (2015).
13 Kaushik, S. S. et al. Magn Reson Med (2016).
14 Matheson, A. M. et al. Radiology (2022).
15 Mummy, D. G. et al. Radiology (2021).
16 Wang, J. M. et al. Thorax (2018).
Figures
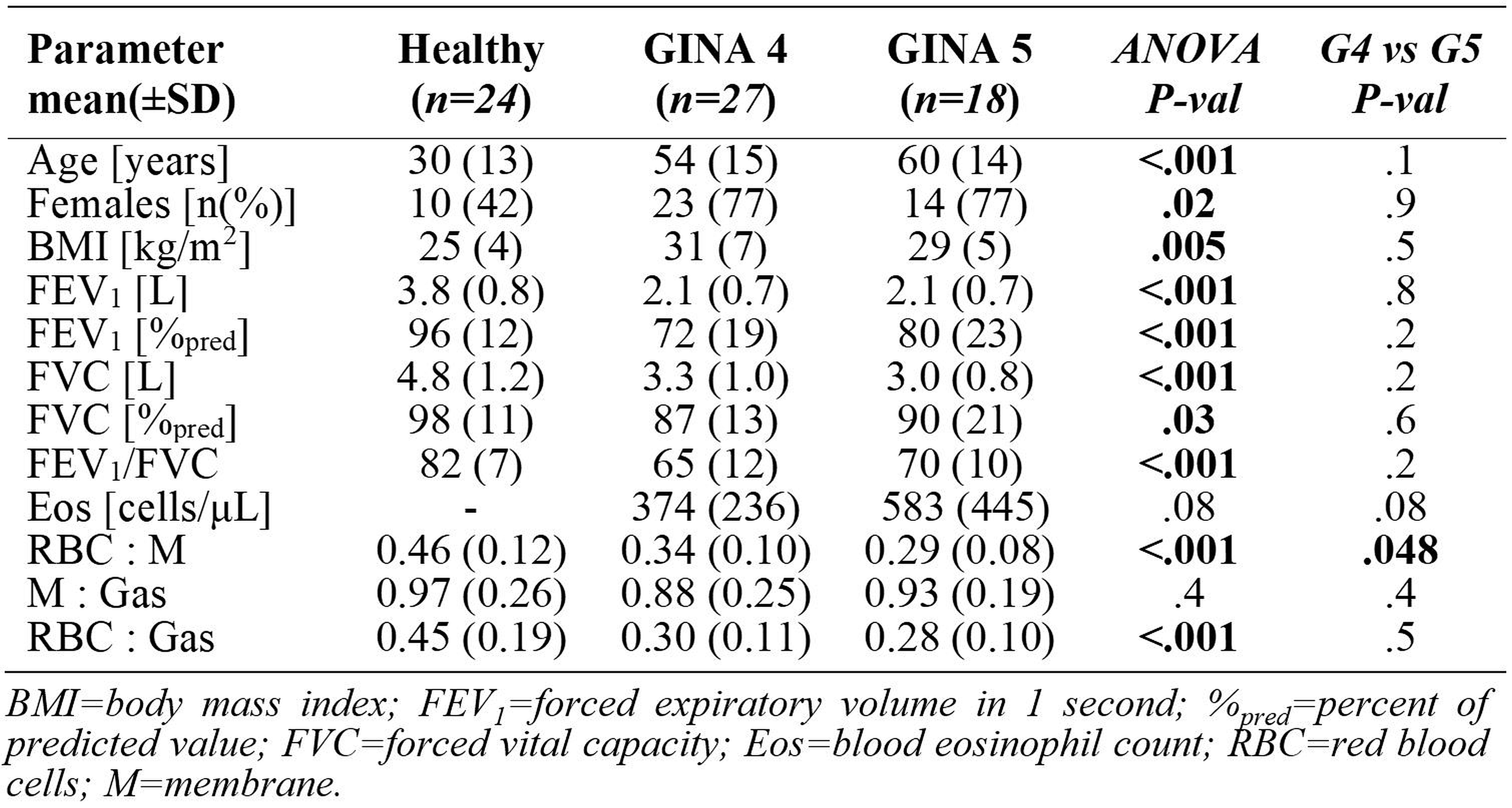
Table 1. Demographics, pulmonary-function and MR spectroscopy measurements in healthy controls, GINA-4 and GINA-5 asthma participants.
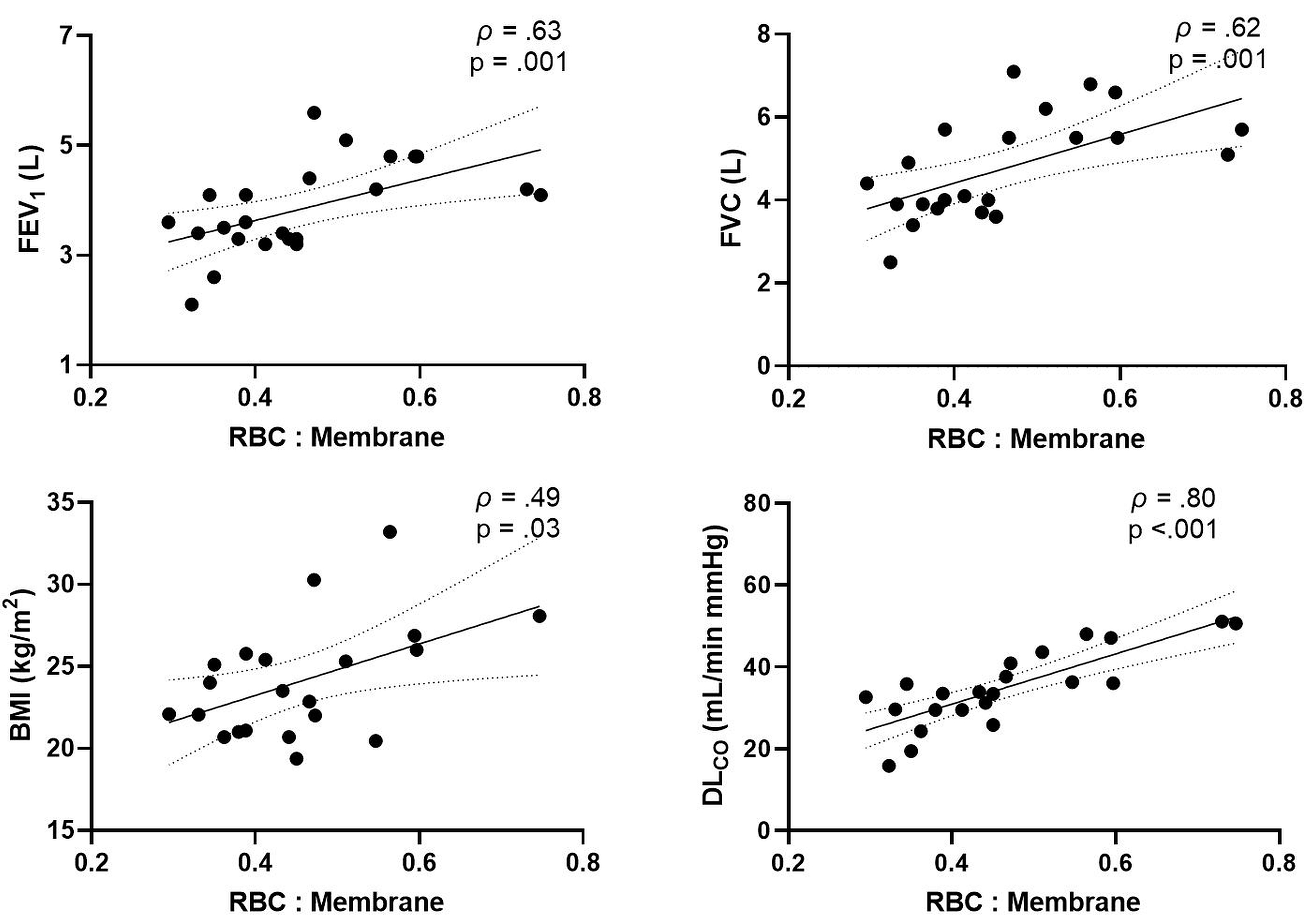
Figure 1: Spearman correlations for dissolved-phase RBC:membrane measurement in healthy volunteers. MRS RBC:membrane significantly correlated with FEV1 (ρ=.63, p=.001), FVC (ρ=.62, p=.001), BMI (ρ=.49, p=.03) and DLCO (ρ=.80, p<.001) measures.
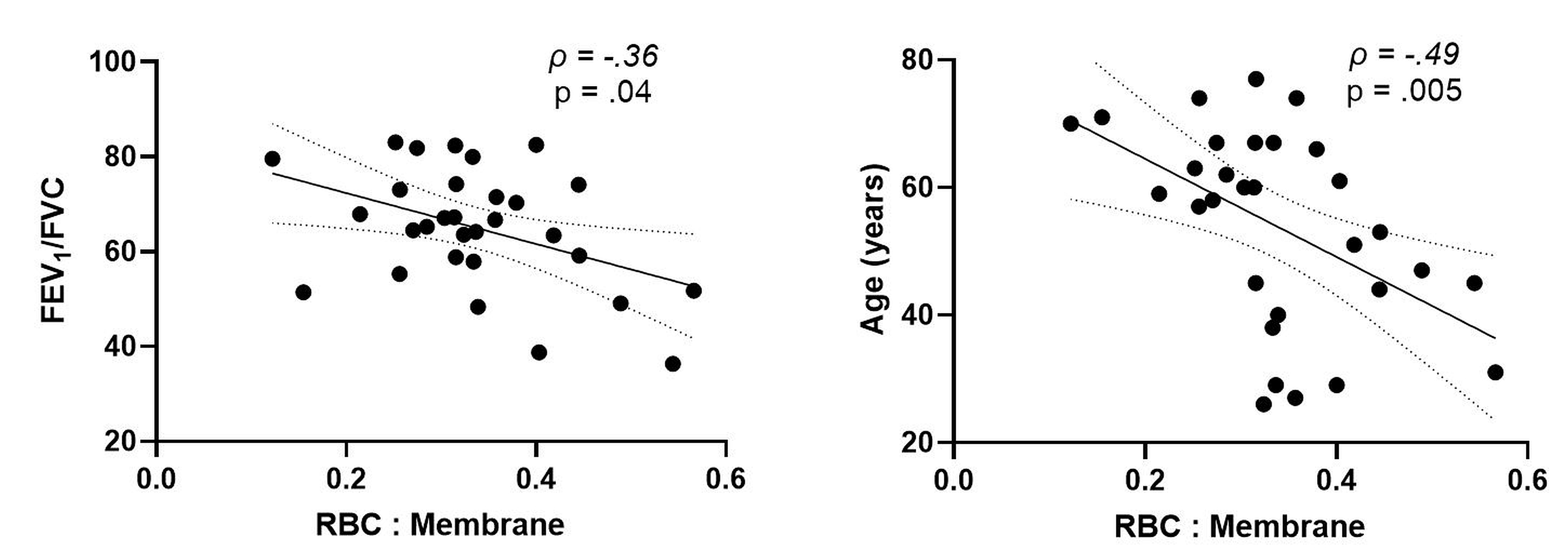
Figure 2: Spearman correlations for dissolved-phase RBC:membrane measurement in mild-moderate (GINA 4) asthma. MRS RBC:membrane significantly correlated with FEV1/FVC (ρ=-.36, p=.04) and age (ρ=-.49, p=.005) measurements.
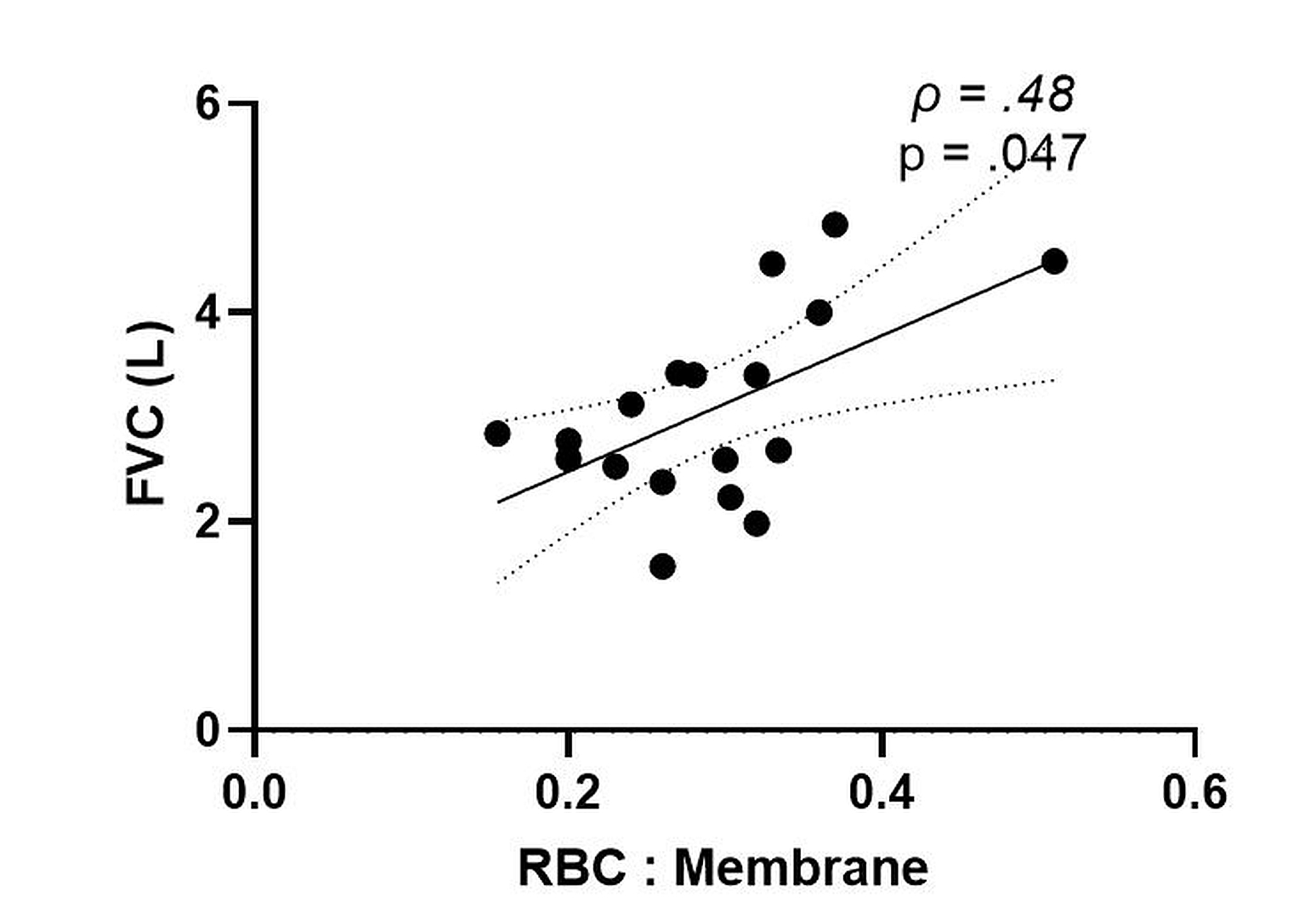
Figure 3: Spearman correlation for dissolved-phase RBC:membrane measurement in severe (GINA 5) asthma. MRS RBC:membrane significantly correlated with FVC (ρ=.48, p=.047) measurements.