3189
129Xe MRS Biomarkers Predict 6-week Response to ICS/LAMA/LABA in Moderate Asthma1Department of Medical Biophysics, Western University, London, ON, Canada, 2Robarts Research Institute, London, ON, Canada, 3School of Biomedical Engineering, Western University, London, ON, Canada, 4Division of Respirology, Department of Medicine, Western University, London, ON, Canada
Synopsis
Keywords: Hyperpolarized MR (Gas), Hyperpolarized MR (Gas), asthma, gas-exchange, MRS, lung
Motivation: 129Xe MRS quantifies pulmonary gas-exchange by probing inhaled 129Xe transfer from the alveolar-membrane to the red-blood-cells (RBC). Recent work suggested a vascular response to asthma therapy, quantifiable using 129Xe MRS.
Goal(s): We aimed to examine if 129Xe MRS measurements were predictive of significant 6-week response to ICS/LAMA/LABA in moderate asthma patients.
Approach: 129Xe MRS and pulmonary function measurements were acquired prior to and following 6-weeks of therapy.
Results: 129Xe RBC:membrane, measured prior to treatment, was predictive of response to ICS/LAMA/LABA at 6 weeks, measured using the fraction-of-exhaled nitric-oxide and the ratio of forced-expiratory-volume in 1-second to forced-vital-capacity.
Impact: For the first time, 129Xe MRS RBC:membrane has been shown to predict early (6-week) response to ICS/LAMA/LABA in moderate asthma. 129Xe MRS uncovered a novel pathophysiology in asthma patients, with potential for consideration as a new treatable target.
Introduction
Inhaled hyperpolarized MRI provides a way to measure airway, alveolar and pulmonary vascular function in the lung simultaneously and with relatively high spatial resolution. In people with asthma, ventilation abnormalities are quantified as ventilation defect percent (VDP)1 which has been shown to relate to airway inflammation2,3 and remodeling,4 independently predict asthma control,5 and sensitively respond to therapy.6,7 Recently, hyperpolarized 129Xe MRI and spectroscopy (MRS) have made it possible to interrogate gas-exchange abnormalities via the detection of 129Xe gas transfer into the alveolar-membrane and red-blood-cells (RBC).8 Abnormal gas-exchange has been quantified using the ratio of 129Xe signal in the RBC and alveolar membrane (RBC:membrane).9,10Asthma is considered an airways disease, although, the presence of a vascular component has been shown using CT measurements of the pulmonary vascular tree.11 Such pulmonary vascular abnormalities also normalized in patients with severe asthma following biologic therapy.12 Here we aimed to investigate patients with moderate asthma and whether 129Xe MRS gas-exchange measurements were related to 6-week response to ICS/LAMA/LABA (inhaled corticosteroid, long-acting muscarinic antagonist, long-acting beta-agonist).
Methods
Participants and Study Design:Participants with moderate asthma provided written informed consent to an approved protocol to receive daily inhaled fluticasone furoate, umeclidinium, and vilanterol (200/62.5/25µg) for 6-weeks. Participants completed pre-/post-bronchodilator (BD) spirometry, oscillometry, fraction of exhaled nitric oxide (FeNO) and 129Xe MRI/MRS at Week-0 and at Week-6.
MRI Acquisition:
Anatomical 1H and hyperpolarized 129Xe MRI/MRS were acquired using a 3T Discovery MR750 with broadband capability, as previously described.13-15 Anatomical 1H images were acquired using a fast-spoiled gradient-recalled echo (FGRE) sequence (total acquisition time=8s; TR msec/TE msec=4.7/1.2; flip-angle=30°; FOV=40×40cm2; bandwidth=24.4kHz; 128×80 matrix, zero-padded to 128×128; partial echo percentage=62.5%; 15-17 slices; slice thickness=15mm; no gap). Static ventilation images were acquired using a three-dimensional FGRE sequence (total acquisition time=14s; TR msec/TE msec=6.7/1.5; variable flip-angle; FOV=40×40cm2; bandwidth=15.63kHz; 128×128 matrix, zero-padded to 128×128; 14 slices; slice thickness, 15mm; no gap). 129Xe MRS was acquired using a free-induction-decay whole-lung spectroscopy sequence (200 dissolved-phase spectra, TR msec/TE msec=15/0.7; flip-angle=40°; BW=31.25kHz, 600μs 3-lobe Shinnar-Le Roux pulse). Participants were instructed to inhale and hold 1.0L of gas (100% N2 for anatomical scan, 400mL hyperpolarized 129Xe + 600mL 4He for static ventilation scan, 200mL hyperpolarized 129Xe + 800mL 4He for MRS scan) to ensure volume matched images. 129Xe gas was polarized to 20%-50%.16
Data Analysis:
MRS peaks were fit to three complex Lorentzian distributions to determine compartment frequency, full-width half maximum, and area under the curve (AUC). RBC:membrane ratio was calculated as the ratio of RBC AUC to membrane AUC. Gas-transfer MRI data were reconstructed using a re-gridding method for non-cartesian acquisition.17 Receiver phase-offset and local phase inhomogeneity were corrected, as previously described.8 MRI VDP was quantified using a semi-automatic method which normalizes the volume of ventilation defects to the total thoracic cavity volume.1 Temporal differences were evaluated using paired samples t-tests. Univariable relationships were evaluated using Pearson (r) correlations. Multivariable models were generated, using the backwards approach, to explain changes observed post-treatment. Results were considered statistically significant when the probability of making a type I error was less than 5% (P<.05).
Results
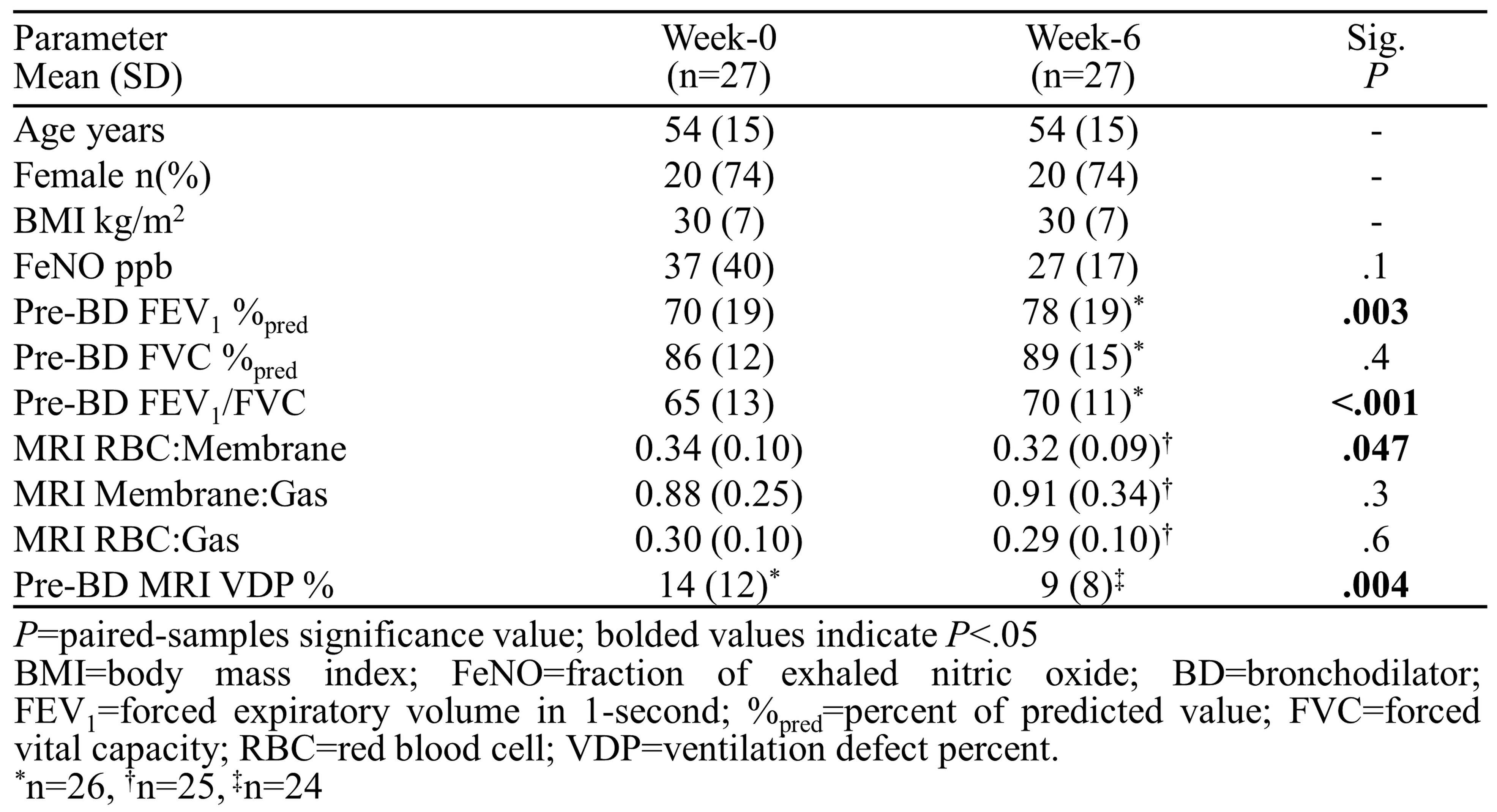
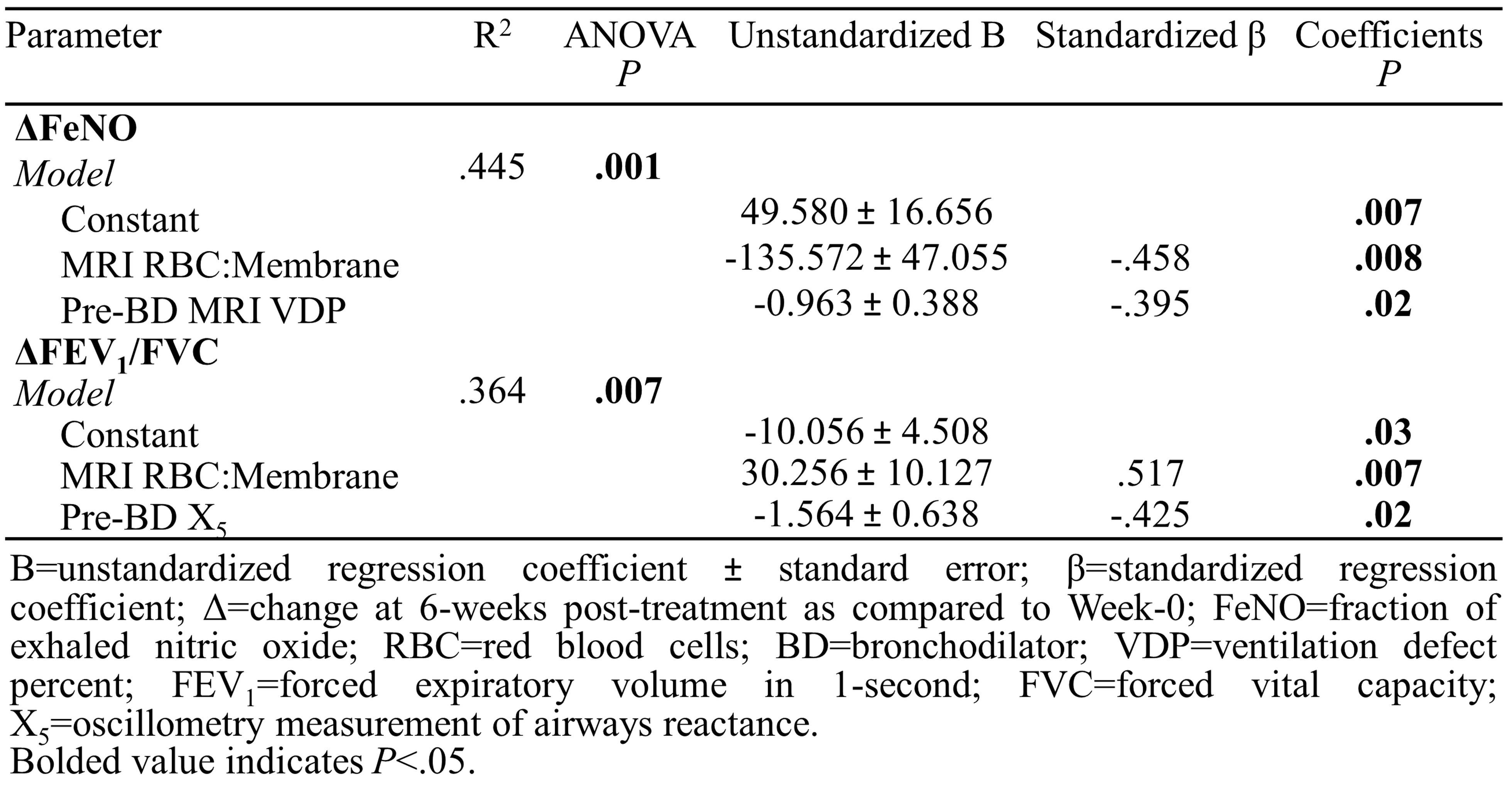
Table 1 provides demographic, pulmonary function, and imaging characteristics for 27 participants (mean age, 54±15 years). Forced expiratory volume in 1-second (FEV1, P=.003), the ratio of FEV1 to forced vital capacity (FEV1/FVC, P<.001), MRI RBC:membrane (P=.047), and VDP (P=.004) were different between Week-0 and Week-6. Table 2 shows MRI RBC:membrane (β=-.458, P=.008) and VDP (β=-.395, P=.02) measured at Week-0 predicted the change in FeNO, while RBC:membrane (β=.517, P=.007) and the oscillometry measurement for airways reactance (β=-.452, P=.02) predicted the change in FEV1/FVC. Figure 1 shows that, at Week-0, RBC:membrane correlated with FeNO (r=.56, P=.002), FEV1 (r=-.45, P=.02), and FEV1/FVC (r=-.60, P=.001).Discussion
Using 129Xe MRS, we identified that RBC:membrane, measured prior to treatment, was predictive of early response to ICS/LAMA/LABA treatment in moderate asthma. RBC:membrane correlated with markers of airway inflammation (FeNO) and obstruction (FEV1/FVC) and was a significant predictor of improvement in these same measurements following 6-weeks of therapy. This may suggest RBC:membrane is indicative of alveolar-membrane gas-exchange abnormalities driven by upstream airway inflammation and obstruction, as previously shown in obstructive lung disease.9 In this way, 129Xe MRS revealed novel vascular pathophysiology that may contribute to understanding the response to therapy in this group of patients.Conclusion
For the first time, 129Xe MRS measurements of pulmonary gas-exchange in the alveolar-membrane and red-blood-cells predicted early (6-week) treatment response to ICS/LAMA/LABA in moderate asthma patients. This finding helps frame a new paradigm for pulmonary vascular or gas-exchange treatable targets in asthma management.Acknowledgements
Study 217438 is a Supported Collaborative Study with GSK.References
1 Kirby, M. et al. Acad Radiol (2012).
2 Svenningsen, S. et al. Thorax (2014).
3 Svenningsen, S. et al. Am J Respir Crit Care Med (2018).
4 Eddy, R. L. et al. Am J Respir Crit Care Med (2020).
5 Svenningsen, S. et al. Eur Respir J (2016).
6 Svenningsen, S. et al. Chest (2020).
7 McIntosh, M. J. & Kooner, H. K. et al. Chest (2022).
8 Kaushik, S. S. et al. Magn Reson Med (2016).
9 Wang, Z. et al. Eur Respir J (2019).
10 Wang, J. M. et al. Thorax (2018).
11 Ash, S. Y. et al. Am J Respir Crit Care Med (2018).
12 McIntosh, M. J. et al. Am J Respir Crit Care Med (2023).
13 Parraga, G. et al. Invest Radiol (2007).
14 Svenningsen, S. et al. J Magn Reson Imaging (2013).
15 Matheson, A. M. et al. Radiology (2022).
16 Walker, T. G. & Happer, W. Rev Mod Phys (1997).
17 Robertson, S. H. et al. Concepts Magn Reson A (2015).
Figures
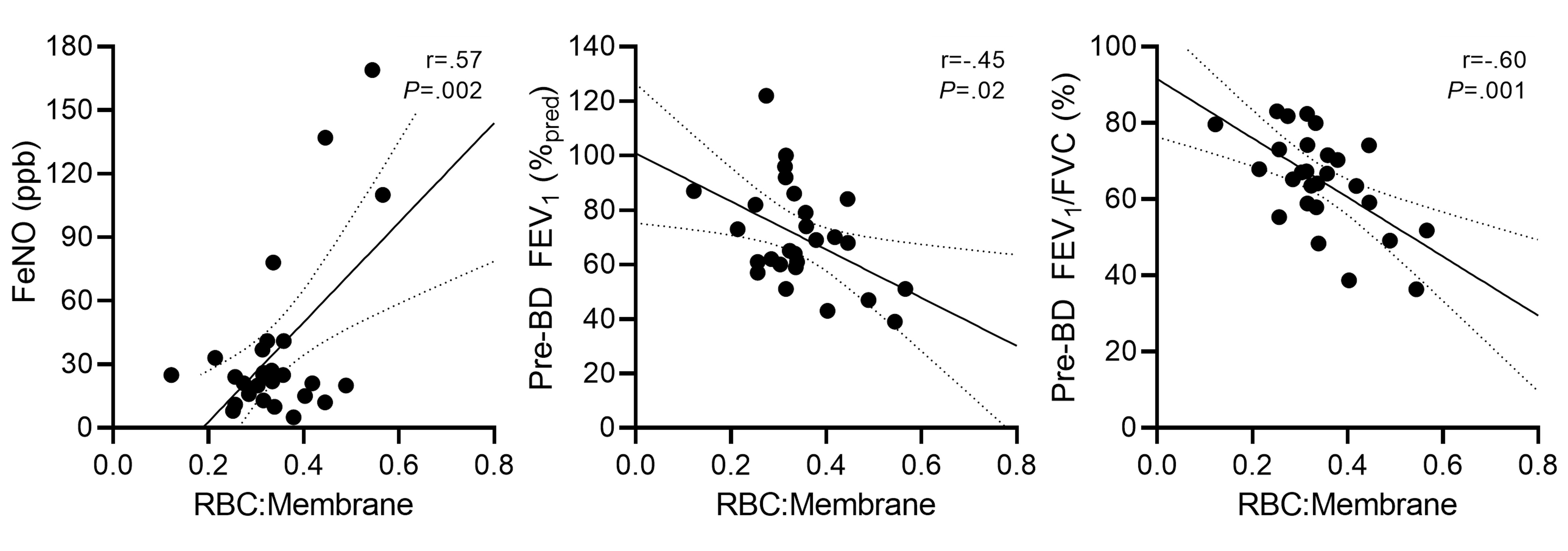
Scatter plots show RBC:Membrane correlates with FeNO (r=.56, P=.002), FEV1 (r=-.45, P=.02), and FEV1/FVC (r=-.60, P=.001).
RBC=red blood cells; FeNO=fraction of exhaled nitric oxide; FEV1=forced expiratory volume in 1-second; %pred=percent of predicted value; FVC=forced vital capacity.