3187
Hyperpolarized Xe MRI to Evaluate Lung Function in Patients with History of BPD1Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States
Synopsis
Keywords: Hyperpolarized MR (Gas), Hyperpolarized MR (Gas)
Motivation: With improved neonatal care and increased survival of very preterm infants, the incidence of bronchopulmonary dysplasia (BPD, or chronic lung disease of prematurity) has increased.
Goal(s): To evaluate Xe gas-exchange MRI by investigating success rates, sensitivity, and correlations with clinical demographics and pulmonary function testing.
Approach: In 24 patients, Xe ventilation, restricted diffusion, and gas-exchange MRI were collected along with pulmonary function testing and electronic health records.
Results: We found hyperpolarized Xe-MRI detects ventilation, lung microstructure, and gas-exchange abnormalities in 53%, 59%, and 82% of patients, respectively. Additionally, ventilation obstruction worsened with age, and two imaging phenotypes were detected.
Impact: Hyperpolarized Xe-MRI detected significant ventilation defects in 53% and lung microstructure abnormalities in 59% of bronchopulmonary dysplasia patients. Gas-exchange MRI revealed two phenotypes, with abnormalities in membrane-uptake (82%), RBC-transfer (65%), and RBC:Membrane ratio (29%).
Introduction
Bronchopulmonary dysplasia (BPD) is a chronic lung disease associated with preterm birth and many patients have lung function impairment in adulthood(1). Recent results from Xe-MRI showed abnormalities in lung ventilation and lung microstructure(2), but Xe gas-exchange MRI, which quantifies gas transfer to the interstitial tissues (membrane) and red blood cells (RBCs), has not been investigated(3). In this ongoing study, we hypothesized gas-exchange MRI can be successfully collected in more patients than traditional pulmonary function tests, would be sensitive to lung-function abnormalities, and provides additional insight into the disease progression and/or phenotypes.Methods
24 school-age to young-adult patients with BPD were recruited (Figure 1) and imaged with consent/assent under an IRB-approved protocol (FDA IND-123,577). Xe was polarized to 20-40% via a Xe hyperpolarizer (Polarean 9820), and Xe MRI was acquired at 3.0T (Philips), using a commercial Xe chest coil (Clinical MR Solutions). Ventilation, restricted diffusion, and gas-exchange images were acquired. Successful breath-holds were determined by k0 signal in the gas-exchange acquisition and visual inspection of the images.Xe ventilation images were acquired using a 2D gradient-echo sequence with a resolution of 3×3×15mm. TE\TR were set to minimum [1.5-3.8ms\7.5-13.0ms]. Ventilation defect percentage (VDP) was calculated using a threshold of 60% of the mean signal, following N4 bias correction(5).
Xe diffusion images were acquired using a 2D GRE sequence with diffusion encoding (4 b-values: 0, 10, 20, 30 s/mm2) and a resolution of 5×5×15mm(3). TE\TR were 2.9ms\6.1ms. Images were reconstructed offline in MATLAB and voxel-wise apparent diffusion coefficient (ADC) maps were calculated.
Xe gas-exchange images were acquired using the 1-point, interleaved 3D-radial sequence previously published(4). Imaging parameters: FOV=325mm3, matrix=563, TR=15ms, TE90≈0.46ms. Images were reconstructed and quantified in MATLAB (4,6).
All imaging-derived metrics are reported as whole-lung means. VDP was compared to an internal healthy cohort of 36 patients; for ADC linear age dependence and confidence intervals were obtained from a previous publication(2). Mean and confidence intervals were calculated for gas-exchange using generalized additive models, with an internal healthy cohort of 81 patients(7). Kendall rank correlations were used to compare Xe-MRI metrics with age and chi-squared tests were used to assess disease sensitivity.
Results
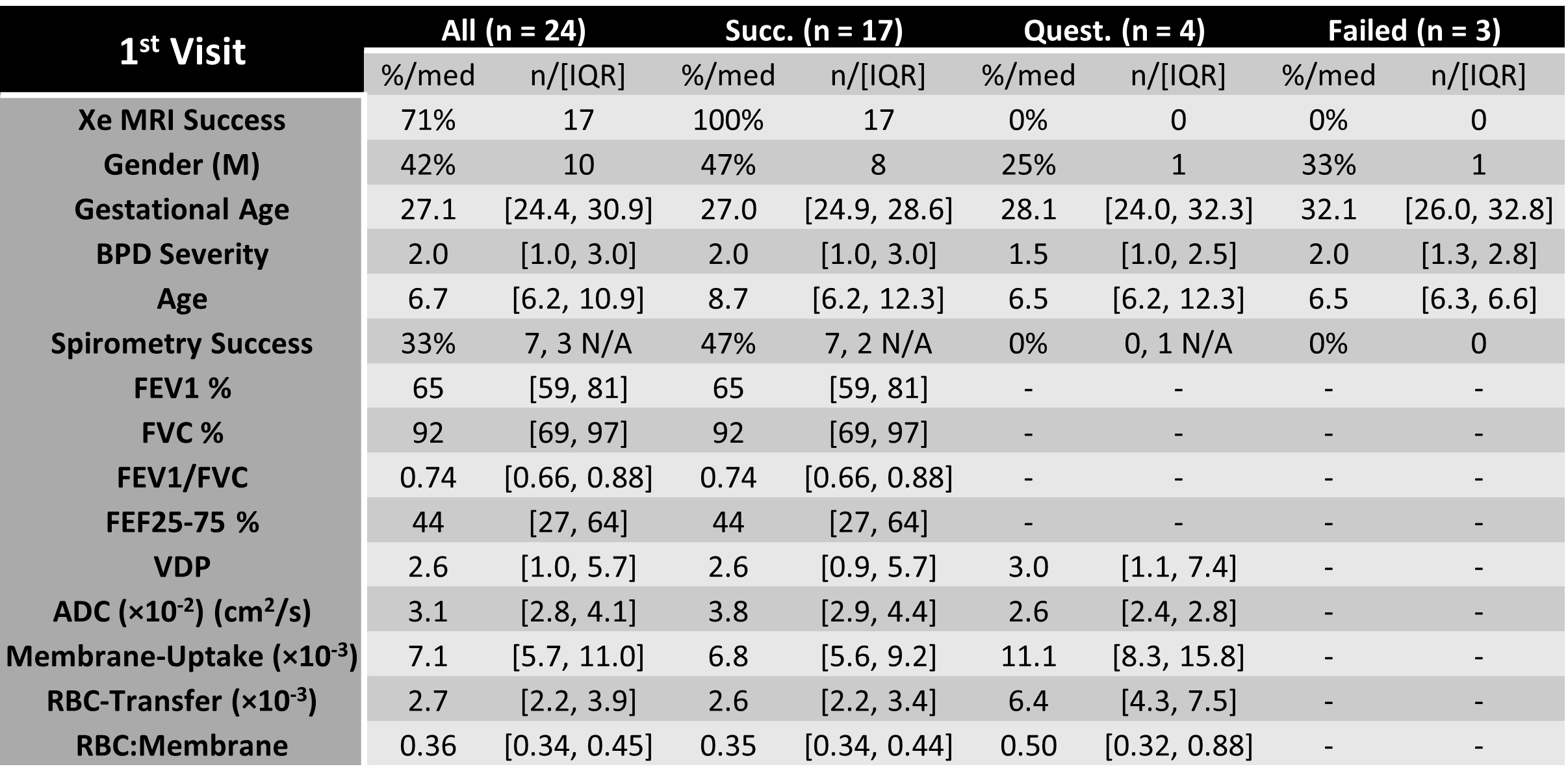
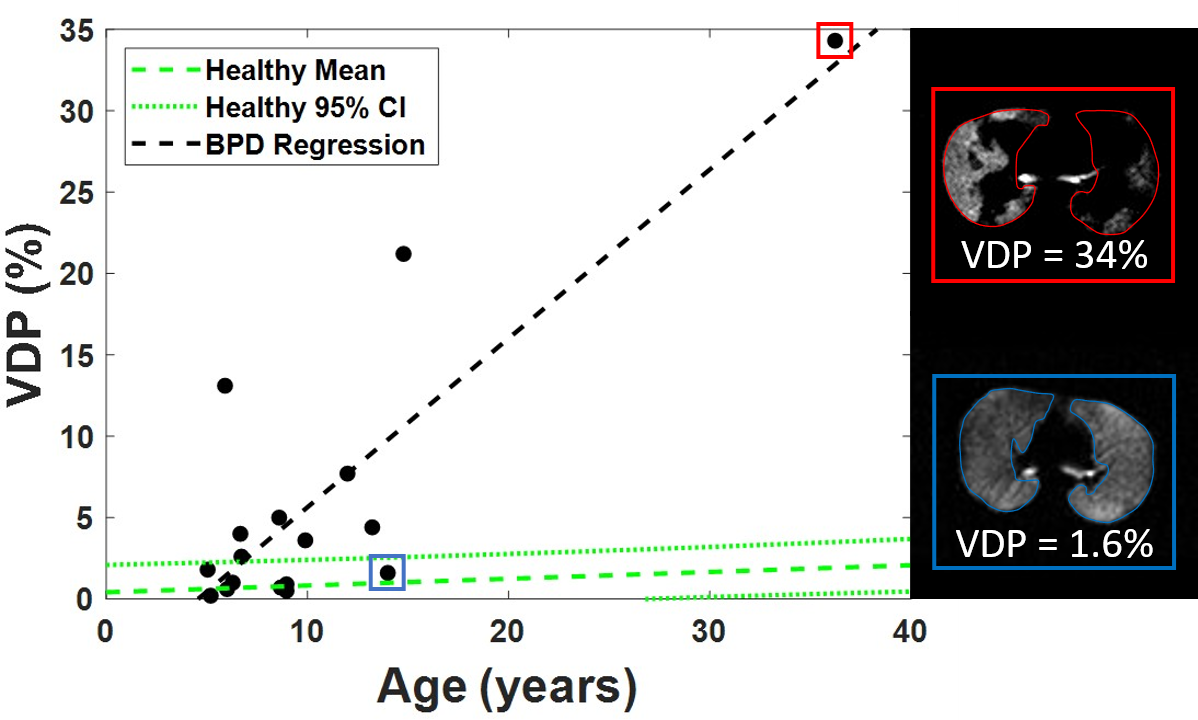
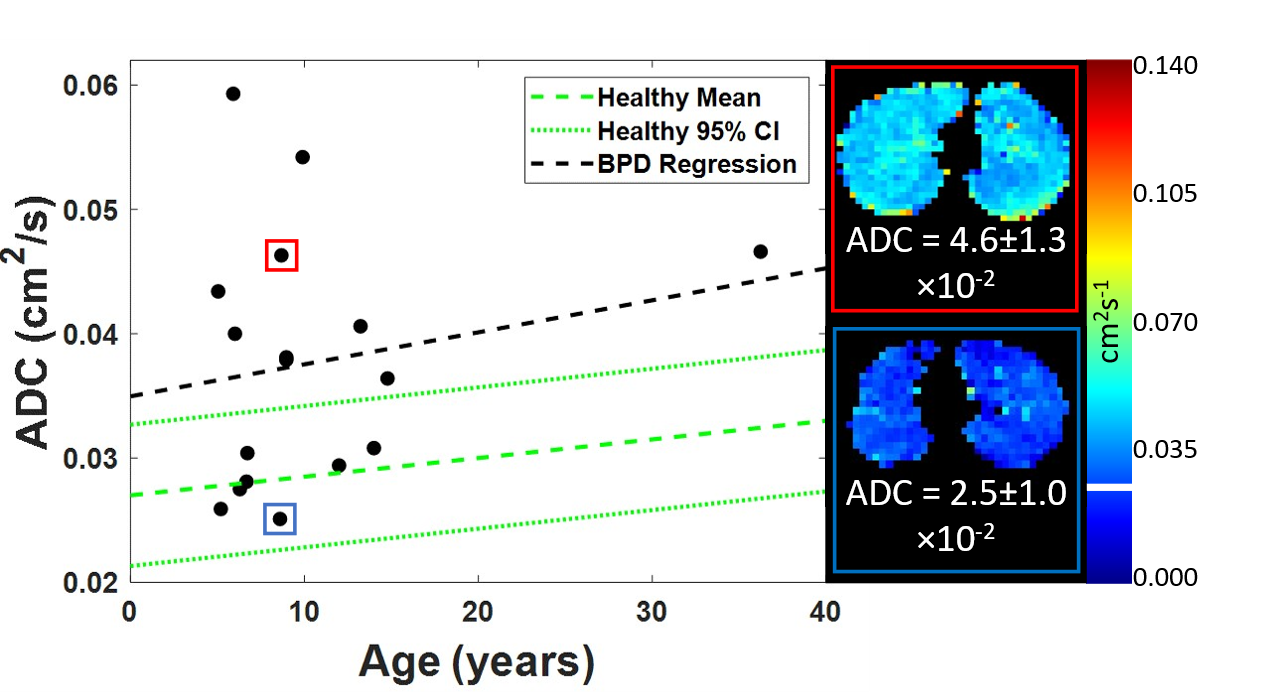
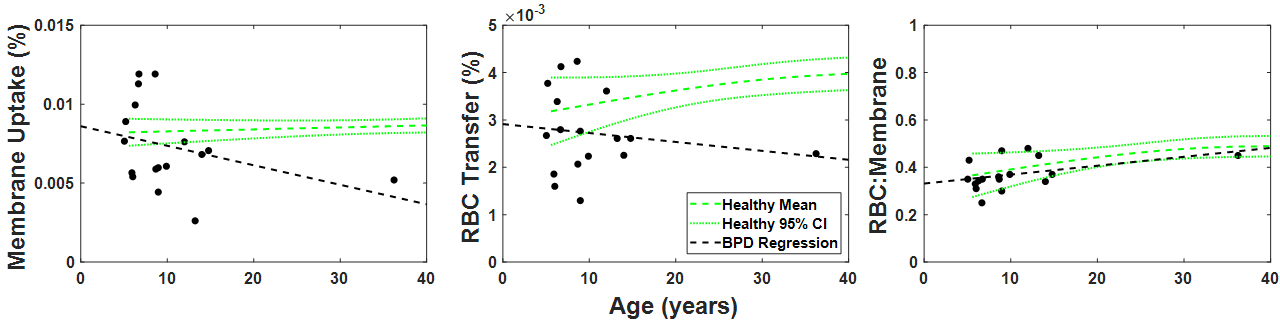
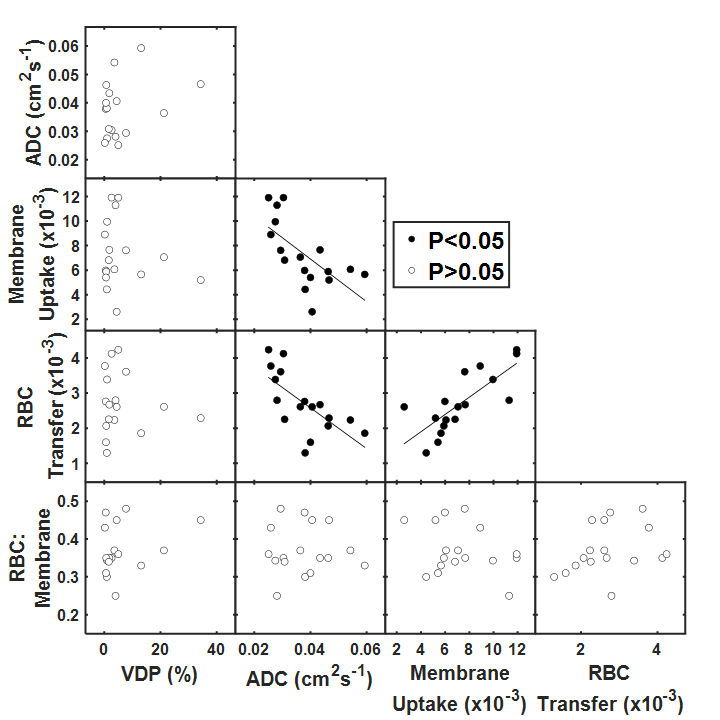
Figure 1 provides the medians and interquartile ranges for patient demographics, traditional pulmonary function testing, and Xe-MRI.Figure 2 shows the VDP of the BPD patients as a function of age and trends towards a positive correlation (P=0.058). ADC shows no correlation with age (P=0.51, Figure 3), and membrane-uptake, RBC-transfer, and RBC:membrane ratios demonstrate no significant correlation with age (P≥0.09, Figure 4).
Some Xe metrics were significantly correlated in Figure 5: ADC correlated with membrane-uptake (τ=-0.53, P<0.01) and RBC-transfer (τ=-0.57, P<0.01), while RBC-transfer correlated with membrane-uptake (τ=0.66, P<0.01).
Discussion
Out of 24 scans, 21 breath-holds resulted in adequate images, but 4 additional were excluded from subsequent analysis because of questionable breath-holds from variation in k0 (Figure 1). Most questionable and failed attempts were with patients significantly younger (6.5 vs. 8.7). Only one patient over the age of 7 did not have a successful breath-hold. Of the failed/excluded attempts, no reported PFTs were to ATS standards (one having usable FEV1), indicating an inability to perform spirometry. The overall success rate for Xe-MRI (3 image set) was more than twice that of spirometry (71% vs. 33%).Significantly elevated VDP (overall mean=6.1%) was found in N=9/17(P<0.01) patients and N=10/17(P<0.01) had simplified alveolar microstructure (mean ADC=132%-predicted), suggesting that these patients do not have catch-up alveolarization as has been previously hypothesized. For gas exchange, membrane-uptake (mean=88%-predicted) was the most sensitive metric, finding N=14/17(P<0.01) of the cohort abnormal (RBC-transfer mean=82%-predicted, RBC:membrane=95%-predicted). Membrane-uptake was both abnormally high (N=4/17, P<0.01) and low (N=10/17, P<0.01), indicative of 2 potential phenotypes of interstitial inflammation/fibrosis and alveolar simplification.
Ventilation did not correlate with the other xenon metrics, likely due to it being mostly sensitive to airway obstruction but correlated with spirometry (P≤0.03). ADC significantly correlated with membrane-uptake and RBC-transfer (P≤0.03) and no patient with alveolar simplification, according to ADC, had increased membrane-uptake, likely indicative of alveolar simplification and a smaller surface-to-volume ratio for gas-exchange. RBC-transfer was strongly correlated with membrane-uptake (P<0.01), suggesting the two gas-exchange compartments are proportionally affected. Other correlations were insignificant, possibly due to the limited statistical power of the smaller cohort.
Conclusion
Xe gas-exchange provides insight into the structure and function of ongoing lung disease in patients with BPD and was more successful than traditional pulmonary function testing, especially in young children. Xe-MRI provides insight into disease phenotypes of this growing population and the potential to develop patient-specific strategies to optimize lung function and treat respiratory symptoms.Acknowledgements
The authors thank the following sources for research funding and support: National Heart, Lung, and Blood Institute R01HL164420, R01HL146689, and The Cincinnati Children’s Research Foundation.References
1. Hysinger EB, Woods JC. Seeing Premature Lung Disease: Hyperpolarized Xe Magnetic Resonance Imaging. Am J Respir Crit Care Med 2023;207(1):15-16.2. Chan H-F, Smith LJ, Biancardi AM, Bray J, Marshall H, Hughes PJC, Collier GJ, Rao M, Norquay G, Swift AJ, Hart K, Cousins M, Watkins WJ, Wild JM, Kotecha S. Image Phenotyping of Preterm-Born Children Using Hyperpolarized <sup>129</sup>Xe Lung Magnetic Resonance Imaging and Multiple-Breath Washout. American Journal of Respiratory and Critical Care Medicine 2023;207(1):89-100.
3. Niedbalski PJ, Hall CS, Castro M, Eddy RL, Rayment JH, Svenningsen S, Parraga G, Zanette B, Santyr GE, Thomen RP, Stewart NJ, Collier GJ, Chan HF, Wild JM, Fain SB, Miller GW, Mata JF, Mugler JP, 3rd, Driehuys B, Willmering MM, Cleveland ZI, Woods JC. Protocols for multi-site trials using hyperpolarized (129) Xe MRI for imaging of ventilation, alveolar-airspace size, and gas exchange: A position paper from the (129) Xe MRI clinical trials consortium. Magn Reson Med 2021;86(6):2966-2986.
4. Willmering MM, Walkup LL, Niedbalski PJ, Wang H, Wang Z, Hysinger EB, Myers KC, Towe CT, Driehuys B, Cleveland ZI, Woods JC. Pediatric (129) Xe Gas-Transfer MRI-Feasibility and Applicability. J Magn Reson Imaging 2022.
5. Roach DJ, Willmering MM, Plummer JW, Walkup LL, Zhang Y, Hossain MM, Cleveland ZI, Woods JC. Hyperpolarized (129)Xenon MRI Ventilation Defect Quantification via Thresholding and Linear Binning in Multiple Pulmonary Diseases. Acad Radiol 2022;29 Suppl 2(Suppl 2):S145-S155.
6. Wang Z, He M, Virgincar R, Bier E, Luo S, Driehuys B. Quantifying hyperpolarized 129Xe gas exchange MRI across platforms, field strength, and acquisition parameters. In: ISMRM, editor2019; Montreal Canada. ISMRM. p 4139.
7. Plummer JW, Willmering MM, Cleveland ZI, Towe C, Woods JC, Walkup LL. Childhood to adulthood: Accounting for age dependence in healthy‐reference distributions in 129Xe gas‐exchange MRI. Magnetic Resonance in Medicine 2022.
Figures