3176
Development of PLGA-loaded ticagrelor magnetic microspheres: towards prevention of post PCI thrombosis.1Department of Radiology, Taiyuan Central Hospital of Shanxi Medical University, Taiyuan, China
Synopsis
Keywords: Molecular Imaging, Molecular Imaging, anti-thrombus
Motivation: After percutaneous coronary intervention, systemic dual antiplatelet therapy prevents thrombosis which may increase the bleeding risk, especially in populations at high risk of bleeding.
Goal(s): The aim of this study was to develop PLGA-Fe3O4-Ticagrelor microspheres (PFTm), for local infusing to injured artery wall for preventing thrombosis.
Approach: Firstly, the abdominal aorta of rabbits was injured by balloon, and PLGA-Fe3O4-Ticagrelor microspheres were infuded into the injured artery, and T2WI imaging was performed.
Results: PFTm was successfully developed, which can effectively prevent thrombosis.
Impact: This study provides a new concept of local infusion for prevention of thrombosis after PCI.
Introduction
Atherosclerotic coronary artery disease is the leading cause of death. Percutaneous coronary intervention ((PCI) combining stent implantation is the main therapeutic method for stable ischemic heart disease and acute coronary syndrome [1-3]. Coronary stents can effectively recanalize blood vessels and rescue ischemic myocardium. However, stenting procedure injures arterial intima, which lead to thrombogenesis. Dual antiplatelet therapy (DAPT), aspirin and one P2Y12 receptor inhibitor, is required to prevent thrombosis formation [4-8]. Routine DAPT may reduce the thrombosis risk but increase bleeding risk [9]. In addition, patients who underwent complex PCI is at higher risk of thrombosis [10-16], which can be reduced by prolonging DAPT. Nevertheless, prolonged use of antiplatelet aggregation drugs increases the risk of bleeding, especially in paitents at high bleeding risk [17-19]. In addition, some patients who require non-cardiac surgery during DAPT have to make hard decision between postpone surgery and stop DAPT. As we know, DAPT is administered systemically to prevent thrombosis locally. In this study, we hypothesized that local infusion of slow-release P2Y12 receptor inhibitor, ticargrelor, can prevent thrombosis without increase bleeding risk systemically.Methods
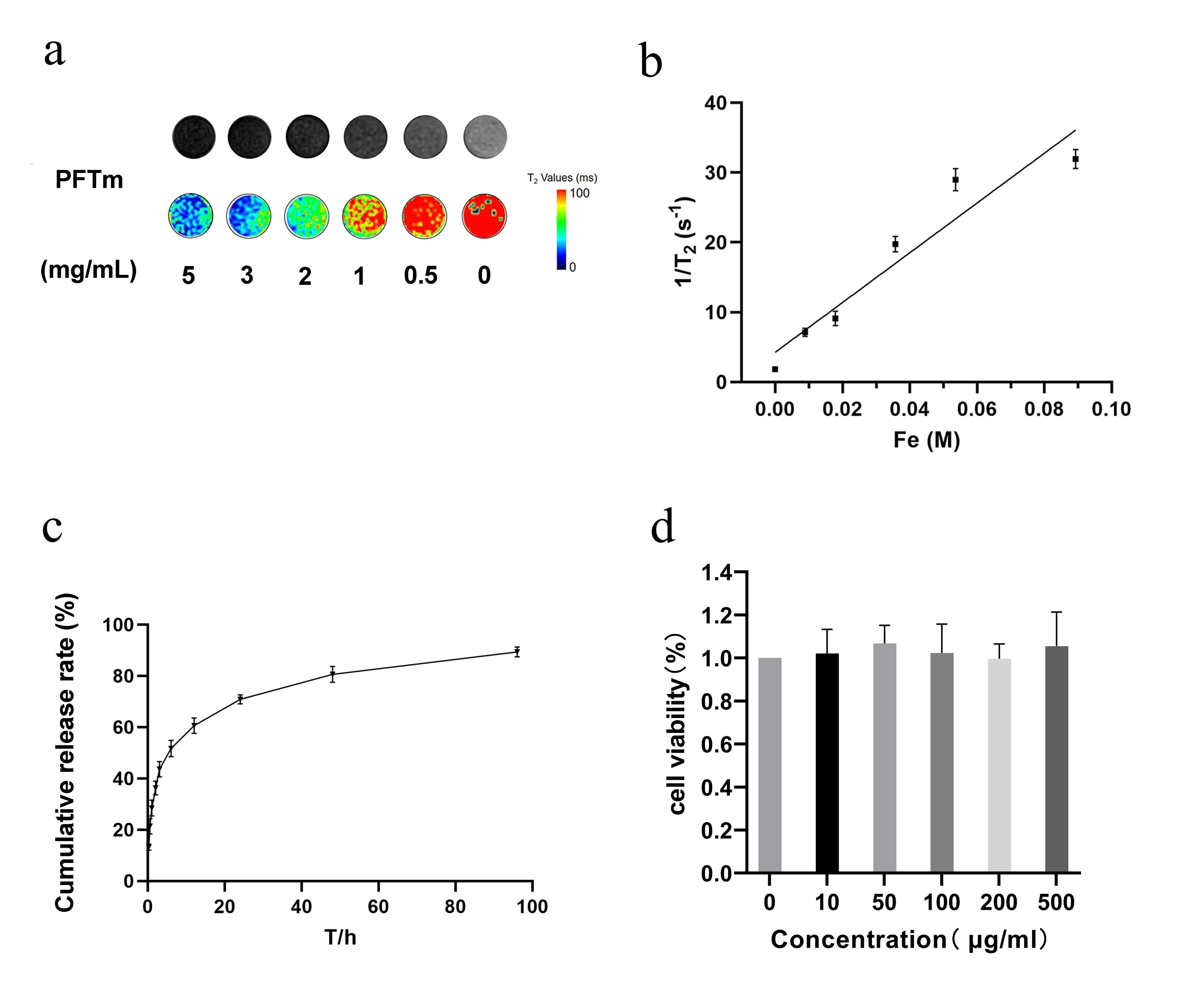
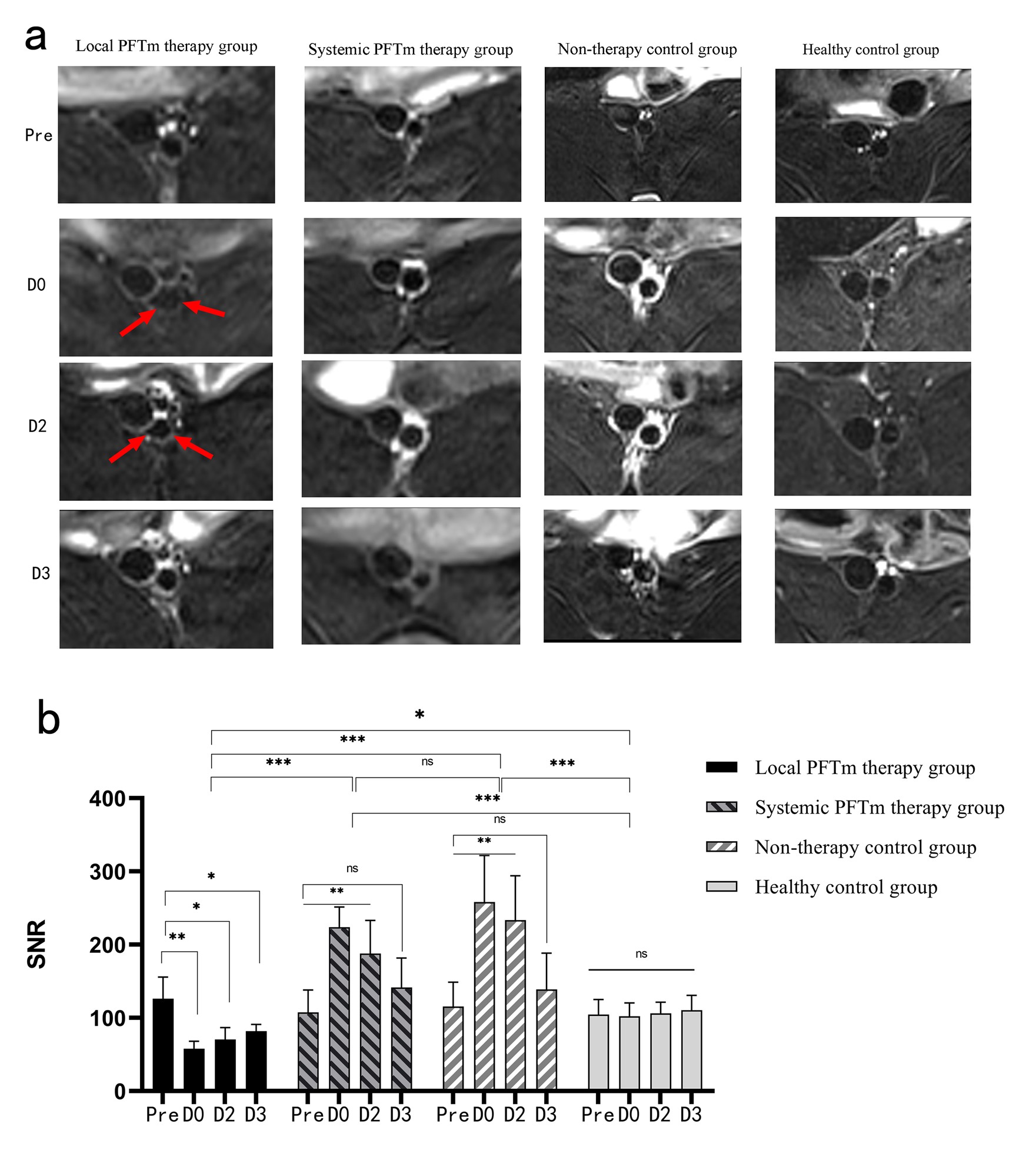
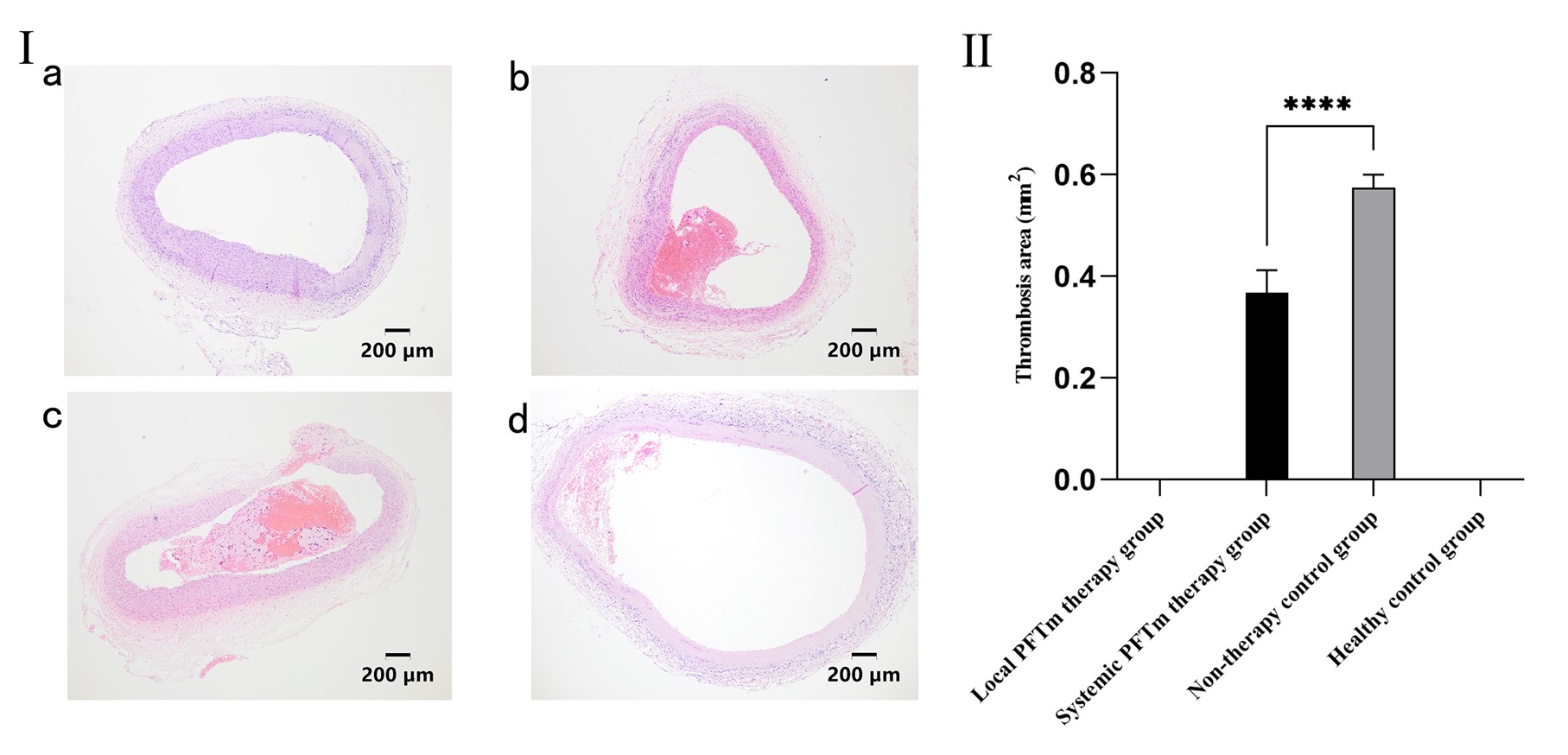
We designed a poly (lactic-co-glycolic acid) (PLGA) loaded with Fe3O4 and ticagrelor magnetic microspheres (PFTm) and prepared by improved emulsified solvent evaporation method. For in vitro study, the morphology, relaxation rate, drug release rate, encapsulation efficiency, and biocompatibility of PFTm were evaluated. For in vivo study, twenty Japanese rabbits were divided into four groups, including local PFTm therapy group(n=6), systemic PFTm therapy group(n=6), non-therapy control group(n=6), and healthy control group(n=6). The healthy control group and non-therapy control group shared one group of animals. The first three groups of rabbits underwent balloon injury for the abdominal aorta. The local PFTm therapy group received balloon PFTm infusion immediately after the injury, while the systemic PFTm therapy group received intravenous PFTm injection. The non-therapy control group and healthy control group did not receive treatment. MR T2 WI was performed pre-operation and post-operation at day0, day2 and day3 to detect PFTm distribution. Then, the animals were euthanized, and the targeted abdominal aorta segments were harvest for pathological sectioning and HE staining.Results
The characterization of PFTm showed it was spherical. The size of the PFTm was 930.5 ± 134 nm, with SPAN=0.35. The overall size of the PFTm was uniform. The drug encapsulation efficiency of the PFTm was 82% ± 2%, the release rate of ticagrelor from the microspheres reached 90% at 96 hours. The r2 of the PFTm was 332.0 mm-1s-1. The microspheres were confirmed to be nontoxic to the cells by CCK-8 (Figure 1). Twenty rabbits (3~4kg) were used for in vivo study. All rabbits were successfully established aorta injury model, in which the first two animals in the local PFTm therapy group were found intramural hematoma during PFTm infusion, resulting in animal death. The results of the eighteen animal experiments showed that PFTm was infused into aortic wall with no thrombus detected in the local PFTm therapy group. The thrombus area in the systemic PFTm therapy group was significantly smaller than that in the non-therapy control group (0.37 ± 0.04 mm2 vs 0.58 ± 0.03 mm2, P < 0.0001) (Figure 2). HE staining showed no thrombus in the local treatment group. Thrombus appeared in both systemic treatment group and non-treatment group (Figure 3).Discussion
This study is the first proof of concept of local perfusion of anti-platelet drug for preventing thrombosis. DAPT drugs are aspirin combined with clopidogrel or ticagrelor[20]. Clopidogrel is an antagonist of P2Y12 receptor, which is a prodrug that requires metabolism in liver. Ticagrelor is a non-prodrug that need no liver metabolism. The experiments proved the method of local administration through interventional procedure, which not only reduces drug consumption in systemic circulation, but also reduces a series of adverse reactions caused by systemic medication including bleeding. Because drug dosage is low and concentrated locall, it enables non-cardiac during DAPT. The limitation of this study is that the observation period after PFTm infusion is short, and the long-term effect remains unknown.Conclusion
This study proves a new concept of local infusion ticargrelor for prevention of thrombosis after PCI, which establishes new technology of antiplatelet local therapy for post-PCI to further reduce the bleeding risk.Acknowledgements
We would like to thank the funding of the project of Shanxi Provincial Science and Technology Department "Basic Research on the inhibition of Thrombosis after vascular Injury by Magnetic resonance Image-guided slow-release magnetic Nanodrug-carrying microspheres (No. : 202103021224003)".References
[1] Passer J Z, Loftus C M. Postoperative Anticoagulation After Neurologic Surgery. Neurosurgery Clinics of North America. 2018; 29(4): 575-583.
[2] Hoole S P, Bambrough P. Recent advances in percutaneous coronary intervention. Heart. 2020; 106(18): 1380-1386.
[3] Agewall S, Antunes M J, Bucciarelli-Ducci C, et al.2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. 2017.
[4] Giustino G, Chieffo A, Palmerini T, et al. Efficacy and Safety of Dual Antiplatelet Therapy After Complex PCI. Journal of the American College of Cardiology. 2016;68(17): 1851-1864.
[5] Colombo A, Chieffo A, Frasheri A, et al. Second-Generation Drug-Eluting Stent Implantation Followed by 6- Versus 12-Month Dual Antiplatelet Therapy. Journal of the American College of Cardiology.2014; 64(20): 2086-2097.
[6] Mehran R, Giustino G, Baber U. DAPT Duration After DES. Journal of the American College of Cardiology. 2015; 65(11): 1103-1106.
[7] Piccolo R, Giustino G, Mehran R, et al. Stable coronary artery disease: revascularisation and invasive strategies. The Lancet. 2015; 386(9994): 702-713.
[8] Capodanno D, Alfonso F, Levine G N, et al. ACC/AHA Versus ESC Guidelines on Dual Antiplatelet Therapy. Journal of the American College of Cardiology. 2018; 72(23): 2915-2931.
[9] Mauri L, Kereiakes D J, Yeh R W, et al.Twelve or 30 Months of Dual Antiplatelet Therapy after Drug-Eluting Stents. New England Journal of Medicine. 2014; 371(23): 2155-2166.
[10] Kirtane A J, Doshi D, Leon M B, et al. Treatment of Higher-Risk Patients With an Indication for Revascularization: Evolution Within the Field of Contemporary Percutaneous Coronary Intervention. Circulation. 2016; 134(5): 422-431.
[11] Giustino G, Mastoris I, Baber U, et al.Correlates and Impact of Coronary Artery Calcifications in Women Undergoing Percutaneous Coronary Intervention With Drug-Eluting Stents. JACC: Cardiovascular Interventions. 2016; 9(18): 1890-1901.
[12] Serruys P W, Takahashi K, Chichareon P, et al. Impact of long-term ticagrelor monotherapy following 1-month dual antiplatelet therapy in patients who underwent complex percutaneous coronary intervention: insights from the Global Leaders trial. European Heart Journal. 2019; 40(31): 2595-2604.
[13] Giustino G, Baber U, Aquino M, et al. Safety and Efficacy of New-Generation Drug-Eluting Stents in Women Undergoing Complex Percutaneous Coronary Artery Revascularization. JACC: Cardiovascular Interventions. 2016; 9(7): 674-684.
[14] Chen H, Power D, Giustino G. Optimal duration of dual antiplatelet therapy after PCI: integrating procedural complexity, bleeding risk and the acuteness of clinical presentation. Expert Review of Cardiovascular Therapy. 2018; 16(10): 735-748.
[15] Généreux P, Giustino G, Redfors B, et al. Impact of percutaneous coronary intervention extent, complexity and platelet reactivity on outcomes after drug-eluting stent implantation. International Journal of Cardiology. 2018; 268: 61-67.
[16] Giustino G, Mehran R. Navigating the complexity of percutaneous coronary intervention in patients at high risk for bleeding. EuroIntervention. 2018; 14(4): e383-e385.
[17] Généreux P, Giustino G, Witzenbichler B, et al. Incidence, Predictors, and Impact of Post-Discharge Bleeding After Percutaneous Coronary Intervention. Journal of the American College of Cardiology. 2015; 66(9): 1036-1045.
[18] Baber U, Dangas G, Chandrasekhar J, et al. Time-Dependent Associations Between Actionable Bleeding, Coronary Thrombotic Events, and Mortality Following Percutaneous Coronary Intervention. JACC: Cardiovascular Interventions. 2016; 9(13): 1349-1357.
[19] Baber U, Mehran R, Giustino G, et al. Coronary Thrombosis and Major Bleeding After PCI With Drug-Eluting Stents. Journal of the American College of Cardiology. 2016; 67(19): 2224-2234.
[20] Degrauwe S, Pilgrim T, Aminian A, et al. Dual antiplatelet therapy for secondary prevention of coronary artery disease. Open Heart. 2017; 4(2): e000651.
Figures