3173
Accelerated High-Resolution 3D Gradient Echo with DL-Based Reconstruction Improves T2* Mapping for Oxygenation-Sensitive MRI1Department of Diagnostic and Interventional Neuroradiology, School of Medicine and Health, Klinikum rechts der Isar, Technical University of Munich, Munich, Germany, 2TUM-Neuroimaging Center, Klinikum rechts der Isar, Technical University of Munich, Munich, Germany, 3Institute of Machine Learning in Biomedical Imaging, Helmholtz Munich, Munich, Germany, 4School of Computation, Information and Technology, Technical University of Munich, Munich, Germany, 5Philips GmbH Market DACH, Hamburg, Germany, 6Clinic for Neurology, School of Medicine and Health, Klinikum rechts der Isar, Technical University of Munich, Munich, Germany
Synopsis
Keywords: Oxygenation, Neuro, quantitative BOLD
Motivation: Standard low-resolution 2D-GRE acquisition for T2* mapping in mqBOLD MRI may suffer from long scan durations and insufficient quantification accuracy.
Goal(s): Improving quantification accuracy by switching from 2D to high-resolution 3D multi-echo GRE while simultaneously reducing scan duration by applying compressed sensing (CS) acceleration with deep-learning-based reconstruction.
Approach: T2* maps from low-resolution 2D-GRE and high-resolution 3D-GRE with different acceleration factors were compared in 11 healthy volunteers based on visual inspection and VOI-analyses.
Results: 3D-GRE yields high-resolution parameter maps with improved T2* values for GM/WM in less than half the scan duration compared to standard 2D-GRE when using CS acceleration with DL-based reconstruction.
Impact: High-resolution 3D-GRE with compressed sensing acceleration and deep-learning-based reconstruction was compared to standard 2D-GRE visually and quantitatively. 3D-GRE enables clinically feasible scan durations with improved and reliable T2* mapping, which may add to the clinical applicability of oxygenation-sensitive mqBOLD MRI.
Introduction
Multi-parametric quantitative BOLD (mqBOLD) MRI allows for quantitative assessment of potentially clinically relevant biomarkers such as the regional oxygen extraction fraction (rOEF)1,2 and oxygen consumption (CMRO2).3,4 Its multi-parametric MRI protocol relies on accurate T2 and T2* mapping. While fast and reliable T2 mapping was already implemented using 3D multi-echo GRASE,2 T2* mapping is currently based on a 2D multi-slice multi-echo gradient echo (GRE) sequence which is affected by magnetic background field gradients (mBFG)5,6 and relies on redundant acquisition of k-space center for correction of subject motion.7 However, mBFG-related bias in T2* could be reduced by switching from 2D- to 3D-acquisition8 and reducing the voxel size,9 resulting in higher T2* values and reduced partial volume effects (PVE). Fully sampled, these adjustments would prolong imaging protocols over the limit of clinical feasibility. Therefore, this study aimed to implement and evaluate 3D high-resolution T2* mapping in comparison to the standard 2D-GRE technique with and without mBFG-correction. A deep learning (DL) integrated compressed sensing (CS) approach was applied with different acceleration factors to reduce scan duration and enhance image quality compared to traditional undersampling techniques.10Methods
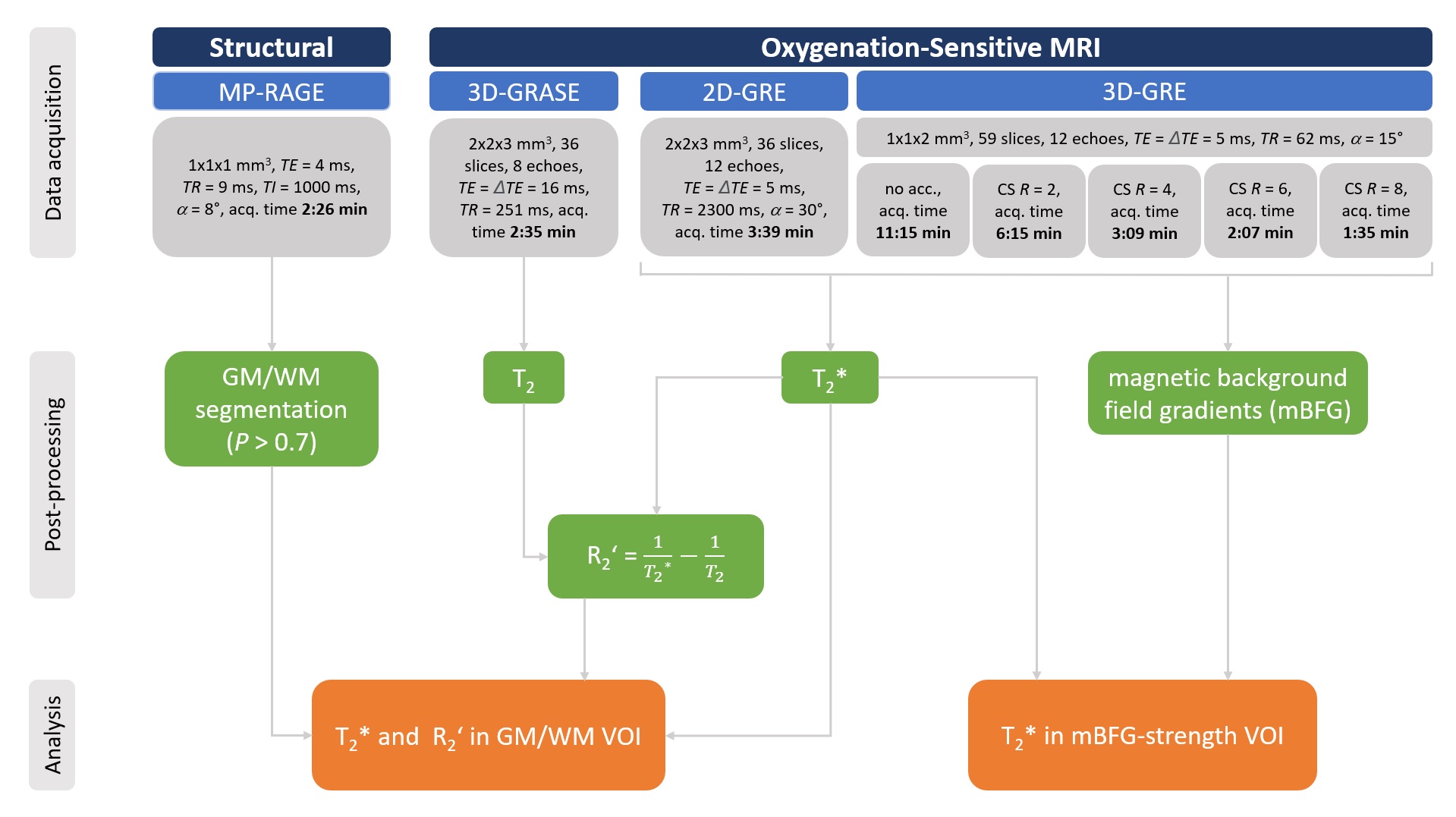
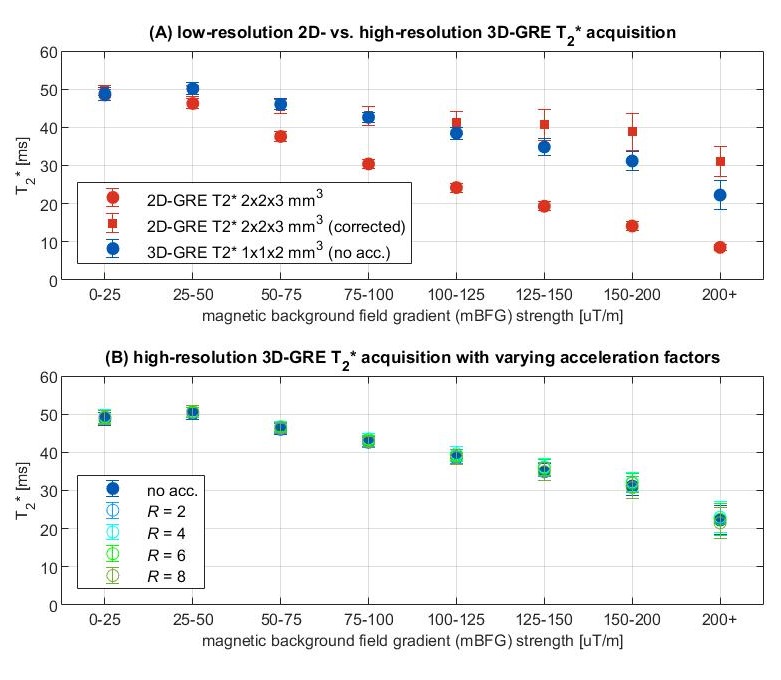
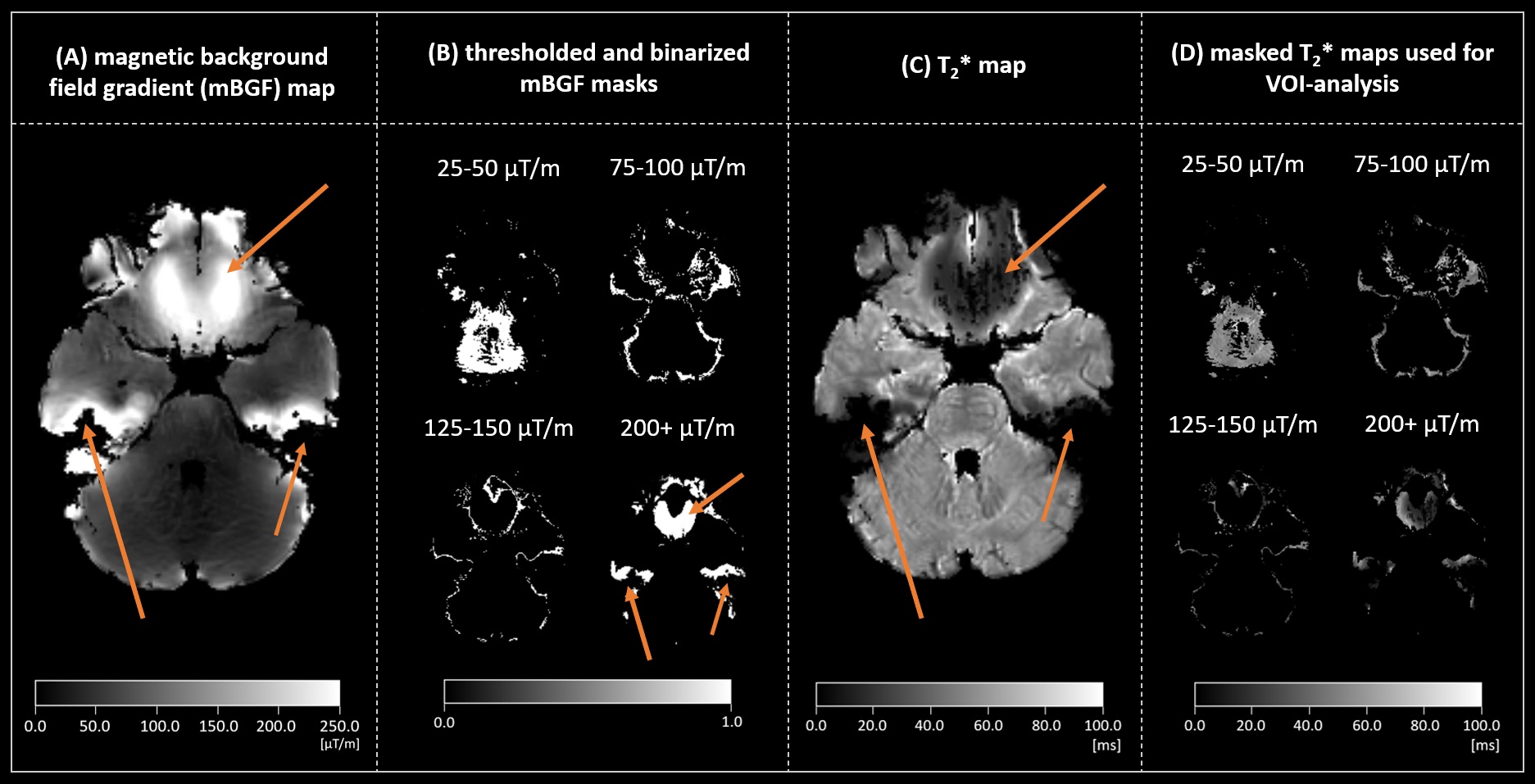
We evaluated data from 11 healthy subjects (27.5±2.7y, 8m) that underwent MRI on a 3T Philips Ingenia Elition X MR-scanner (Philips, Best, Netherlands) using a 32-channel head coil. The imaging protocol included structural and oxygenation-sensitive MRI, particularly T2* mapping by multi-echo 2D-GRE (voxel size 2x2x3mm3) and high-resolution multi-echo 3D-GRE (1x1x2mm3; Fig.1). 3D-GRE was accelerated by CS with an adaptive DL-based reconstruction10 (Philips SmartSpeed) with acceleration factors R=2/4/6/8. Data processing and analysis were performed using SPM1211 and custom MATLAB programs (R2021b, The MathWorks Inc., Natick, USA). T2 and T2* were calculated by exponential fitting of multi-echo data and used to calculate R2’. T2* maps were compared visually and quantitatively within whole-brain gray-/white-matter (GM/WM) volumes-of-interest (VOI). For 2D-GRE data, mBFG-maps were calculated and used for mBFG-correction of T2*.5,6 Additionally, masks of varying mBFG-strength were segmented (bins of 25/50µT/m) and used for VOI-analysis of the corresponding T2* maps to evaluate the dependency of T2* on mBFG-strength. Additional information on how this mBFG-bias analysis was conducted can be found in Fig.4.Results
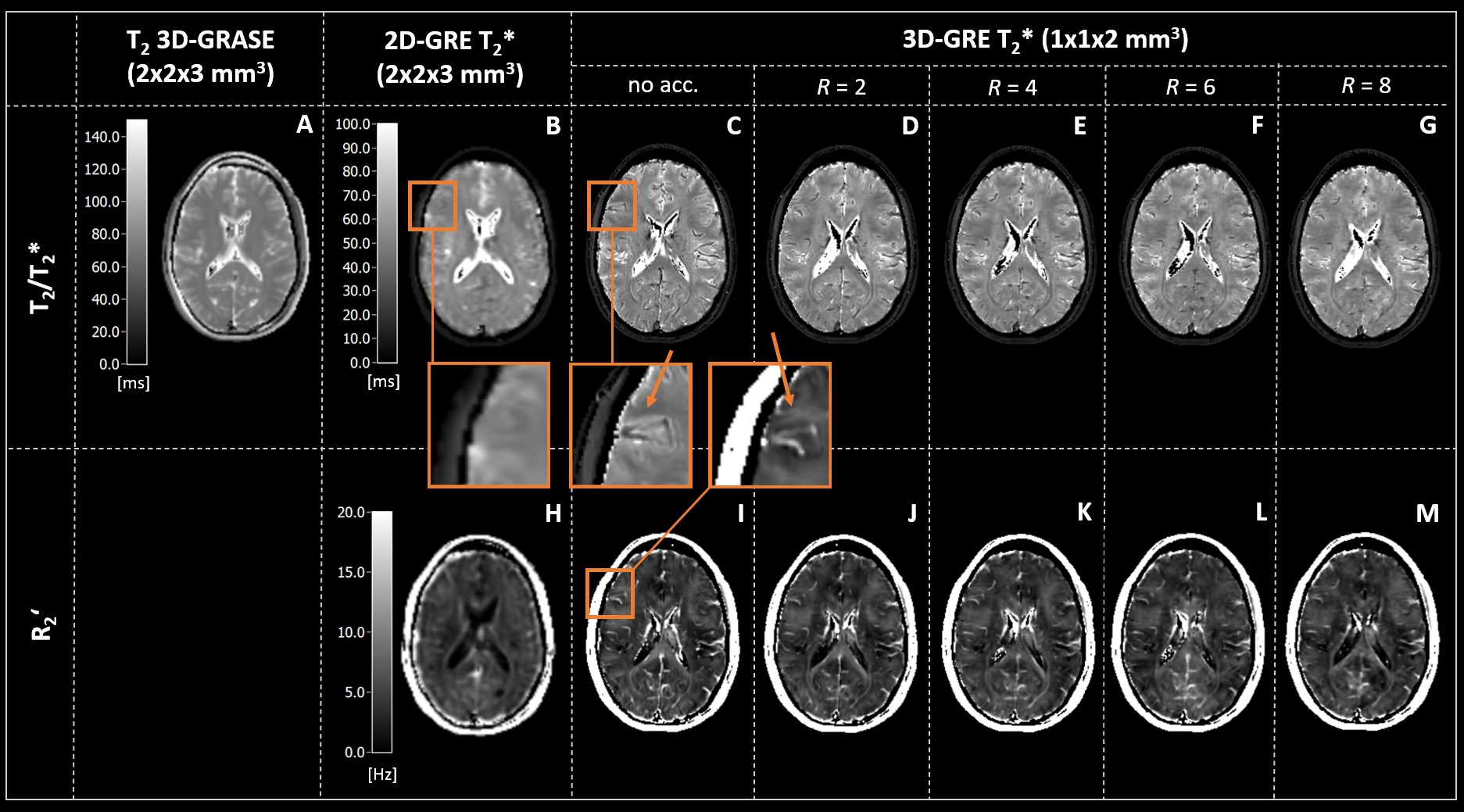
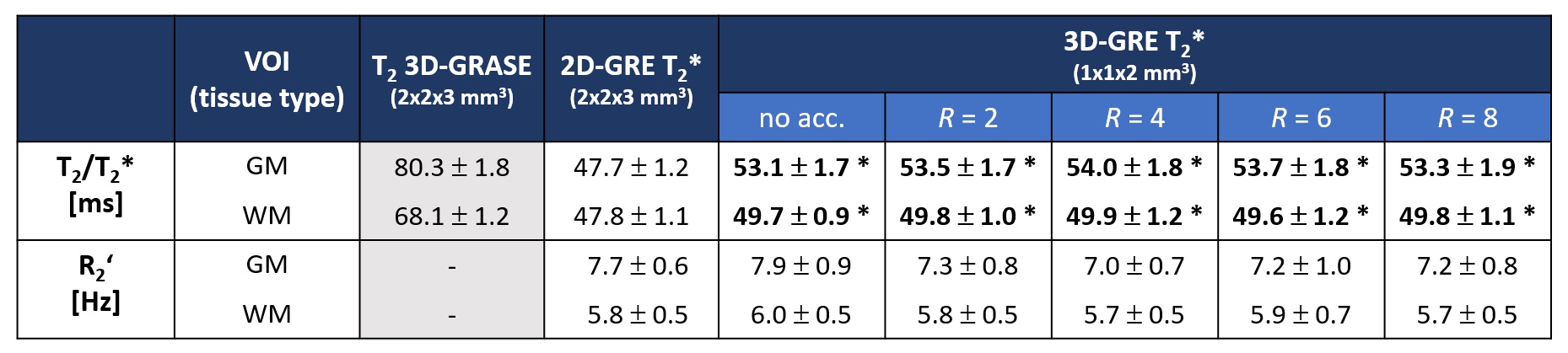
T2* maps (Fig.2B-G) exhibit a noticeable difference in spatial resolution between 2D (Fig.2B) and 3D data (Fig.2C-G). T2* and R2’ maps (Fig.2I-M) from 3D-acquisition appear highly comparable regarding their image quality with increasing acceleration factors R, without noticeable artifacts. The VOI-analysis (Tab.1) shows that GM and WM are well contrasted in 3D-based T2* maps, and mean values for both tissue types are significantly higher compared to standard 2D-GRE. For 3D-GRE, both T2* and R2’ values are stable across acceleration factors. Investigating the dependency on mBFG (Fig.3A), 2D- and 3D-GRE T2* are similar for weak mBFG (<100µT/m, around 96% of all relevant voxels), while for larger mBFG, T2* from 3D-GRE is in between corrected and non-corrected 2D-based T2*. T2* values derived from accelerated 3D-GRE resemble values from fully sampled 3D data (Fig.3B).Discussion
Multi-echo 3D-GRE with voxel size 1x1x2mm3 yields high-resolution T2* and R2’ maps (Fig.2) as well as regionally precise parameter estimates, especially around tissue borders due to reduced PVE. The improved spatial resolution reveals structural details like vessels, which could be segmented and disregarded for oxygenation-parameter calculation (inset in Fig.2B vs. C/I). This may improve the accuracy of the mqBOLD-method, as the model is based on the assumption of a blood vessel network composed of randomly distributed and oriented cylinders, which only holds true for voxels with a small partial volume of blood.12 Our results confirm that high-resolution 3D-GRE is indeed intrinsically less prone to mBFG-related T2* reduction (Fig.3A) compared to low-resolution 2D-GRE, as reported previously.8,9 Additionally, 3D-GRE yields significantly increased T2* values, which generally appear more realistic and indicate reduced mBFG-bias. Moreover, GM was better contrasted from WM compared to the standard 2D-method (Tab.1). Finally, all analyses (Fig.2/Tab.1/Fig.3B) consistently demonstrate that CS with a DL-based reconstruction reliably accelerates 3D-GRE with acceleration factors of up to R=8, which more than bisects measurement time compared to 2D-GRE, without major compromises in image quality or quantification accuracy, fitting previous observations.10Conclusion
In conclusion, we demonstrated that high-resolution 3D-GRE enables more accurate T2* mapping compared to standard 2D-GRE, improving the estimation of oxygenation-sensitive parameters like R2’ and ultimately rOEF and CMRO2 in mqBOLD MRI. Applying CS-based acceleration with DL-based reconstruction allows to reduce the acquisition time by a factor of 2 compared to the reference method without distorting the quantitative results, and thus, ensuring clinically applicable scan durations. Further methodological improvements could be realized by implementing an mBFG-correction method for 3D-GRE.Acknowledgements
We acknowledge support by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) – project number 395030489.References
1. Hirsch NM, Toth V, Förschler A, et al. Technical considerations on the validity of blood oxygenation level-dependent-based MR assessment of vascular deoxygenation. NMR Biomed, 2014; 27(7):853-862.
2. Kaczmarz S, Hyder F, Preibisch C. Oxygen extraction fraction mapping with multi-parametric quantitative BOLD MRI: Reduced transverse relaxation bias using 3D-GraSE imaging. Neuroimage, 2020; 220:117095.
3. Göttler J, Kaczmarz S, Kallmayer M, et al. Flow-metabolism uncoupling in patients with asymptomatic unilateral carotid artery stenosis assessed by multi-modal magnetic resonance imaging. J Cereb Blood Flow Metab, 2019; 39(11):2132-2143.
4. Gersing AS, Ankenbrank M, Schwaiger BJ, et al. Mapping of cerebral metabolic rate of oxygen using dynamic susceptibility contrast and blood oxygen level dependent MR imaging in acute ischemic stroke. Neuroradiology, 2015; 57(12):1253-1261.
5. Baudrexel S, Volz S, Preibisch C, et al. Rapid single-scan T2*-mapping using exponential excitation pulses and image-based correction for linear background gradients. Magn Reason Med, 2009; 62(1):263-268.
6. Hirsch NM, Preibisch C. T2* mapping with background gradient correction using different excitation pulse shapes. AJNR Am J Neuroradiol, 2013; 34(6):E65-68.
7. Nöth U, Volz S, Hattingen E, et al. An improved method for retrospective motion correction in quantitative T2* mapping. Neuroimage, 2014; 92:106-119.
8. Haacke EM, Tkach JA, Parrish TB. Reduction of T2* dephasing in gradient field-echo imaging. Radiology, 1989; 170(2):457-462.
9. Young IR, Cox IJ, Bryant DJ, et al. The benefits of increasing spatial resolution as a means of reducing artifacts due to field inhomogeneities. Magn Reason Imaging, 1988; 6(5):585-590.
10. Pezzotti N, Yousefi S, Elmahdy MS, et al. An Adaptive Intelligence Algorithm for Undersampled Knee MRI Reconstruction. IEEE Access, 2020; 8:204825-204838.
11. Wellcome Centre for Human Neuroimaging. Statistical Parametric Mapping Software (SPM 12).
12. Yablonskiy DA, Haacke EM. Theory of NMR signal behavior in magnetically inhomogeneous tissues: the static dephasing regime. Magn Reson Med, 1994; 32(6):749-763.
Figures