3169
Contribution of coupling task-functional-MRI and kinematic to the analysis of motor function in healthy subjects1Neuroradiology, Montpellier University Hospital, Montpellier, France, 2Siemens Healthineers, Courbevoie, France, 3Euromov Digital Health in Motion, Montpellier, France, 4Laboratoire Charles Coulomb, Montpellier, France
Synopsis
Keywords: fMRI Analysis, fMRI (task based), motor control
Motivation: There is a lack of understanding of the mechanisms of post-stroke motor recovery. To date, fMRI brings information which are not linked to the movement characteristics.
Goal(s): To investigate whether integration of kinematic in fMRI adds any value to the understanding of motor function.
Approach: A block designed motor-task-fMRI experiment coupled with real-time motion-tracking was performed on sixteen healthy subjects. Post-processing consisted of a group-level analysis comparing the regression of the BOLD signal with action-rest onsets, and with the flexion velocity vector.
Results: Using a wider cluster-size, kinematic approach allows retrieving regions found with conventional approach and additional regions involved in motor control.
Impact: Coupling of fMRI with kinematics provides additional information on motor function and motor control. Post-stroke motor recovery is subject to variability and is linked to motor control. Coupling both measurements could provide better understanding of motor recovery at the individual-level.
Introduction
After a stroke, functional MRI (fMRI) shows changes in brain activation patterns [Buma et al. 2010] and motion capture (Mocap) shows changes in movement ability [Kwakkel et al. 2019]. Yet, it is unclear whether combining fMRI and Mocap can help to better understand motor function. Our aim is to report whether integration of kinematics in fMRI adds any value to the understanding of motor function in healthy subjects.Materials and Methods
Sixteen healthy subjects (9 female, age 57.1±17.1 [29-79]) underwent a fMRI recording session while performing a continuous right elbow flexion motor task. Examinations were performed at 3T (MAGNETOM Prisma, Siemens Healthineers, Erlangen, Germany) using a 64-channel head coil. The functional acquisition consisted of a gradient echo planar imaging multiband sequence (TR/TE: 800/38 ms, resolution: 2*2*2 mm).The task stimuli were delivered visually, following a block design with action-rest (30s-30s) phases repeated three times. Motion was captured by an optical system (Oqus 500+, Qualisys, Göteborg, Sweden). Images were pre-processed and analyzed using SPM12 using :
a conventional approach consisting of regression of the BOLD signal with periods of action-rest and a kinematic approach consisting of using the flexion tangential velocity vector averaged (low-pass filter) as a regressor.
A first-level analysis with a p-value threshold of 0.001 and a cluster-size of 30 voxels was conducted for both approaches. The six head motion parameters were used as covariates accounting for head-movement-related artifacts. A second-level analysis was implemented for both approaches, with a threshold level of p<0.05, FWE corrected at the cluster level.
We observed similarities and differences between the conventional and the kinematic approach in the brain regions activated, and in the cluster sizes.
Results
In the first level analysis using the conventional approach, for 13/16 subjects, head motion correction tended to attenuate or even suppress the brain region activations. In these cases, the kinematic approach allowed to retrieve well known motor activations.The second-level analysis of the kinematic approach allowed to retrieved a right cerebellum and a left motor cortex activation which are also found with conventional approach, but also notably four additional regions : the bilateral supplementary motor area, the right Supra Marginal Gyrus (SMG) and the right Parietal Operculum (PO). (fig.1)
Discussion and Conclusion
The first-level analysis of the kinematic approach revealed activation of known primary motor regions, which were not identified using the conventional approach. This suggests a stronger correlation between the BOLD signal and the tangential flexion velocity during the elbow flexion task. It is consistent with studies highlighting a more specific correlation between brain activations and kinematics, compared to the use of motion periods alone [Brihmat 2020 et al.], [Buma et al. 2016].Moreover, group analysis using the kinematic approach allowed to identify regions not found using the conventional approach. In particular, the right and left supplementary motor areas, but also two unidentified regions in the primary motor network, the right SMG and the right PO.
It has been reported that the SMG plays a role in spatial processing and motor control [Ben-Shabat et al. 2015], and that lesions thereof were associated with proprioception deficits at six months after stroke. [Findlater 2018 et al.]
In severe stroke patients, it has also been reported that the PO ipsilateral to the paretic arm was involved in compensatory mechanisms; suggesting the PO was part of a phylogenetically old motor system control involved in motor recovery processes. [Hannanu 2017 et al.]
To date, few studies reported the combination of kinematic using motion capture and fMRI
experiments. The experimental difficulties lie in the low availability of MRI-compatible motion capture devices, and in the fact that patients must perform the movement while lying down in the MRI tunnel, which can be cumbersome considering the small ring diameter.
However, this work emphasizes the potential value of coupling fMRI with kinematics as integrating motion data into fMRI analysis allowed to better identify functional regions of the primary motor network, and to highlight new regions linked to motor control.
Acknowledgements
I would like to thank the healthy subjects for participating in this study.References
Ben-Shabat E, Matyas TA, Pell GS, Brodtmann A, Carey LM. The Right Supramarginal Gyrus Is Important for Proprioception in Healthy and Stroke-Affected Participants: A Functional MRI Study. Front Neurol. 2015 Dec 3;6:248. doi: 10.3389/fneur.2015.00248. PMID: 26696951; PMCID: PMC4668288.
Buma FE, Lindeman E, Ramsey NF, Kwakkel G. Functional neuroimaging studies of early upper limb recovery after stroke: a systematic review of the literature. Neurorehabil Neural Repair. 2010 Sep;24(7):589-608. doi: 10.1177/1545968310364058. Epub 2010 May 3. PMID: 20439501.
Buma FE, van Kordelaar J, Raemaekers M, van Wegen EEH, Ramsey NF, Kwakkel G. Brain activation is related to smoothness of upper limb movements after stroke. Exp Brain Res. 2016 Jul;234(7):2077-2089. doi: 10.1007/s00221-015-4538-8. Epub 2016 Mar 15. PMID: 26979435; PMCID: PMC4893073.
Brihmat N, Boulanouar K, Darmana R, Biganzoli A, Gasq D, Castel-Lacanal E, Marque P, Loubinoux I. Controlling for lesions, kinematics and physiological noise: impact on fMRI results of spastic post-stroke patients. MethodsX. 2020 Sep 9;7:101056. doi: 10.1016/j.mex.2020.101056. PMID: 32995309; PMCID: PMC7509233.
Findlater SE, Hawe RL, Semrau JA, Kenzie JM, Yu AY, Scott SH, Dukelow SP. Lesion locations associated with persistent proprioceptive impairment in the upper limbs after stroke. Neuroimage Clin. 2018;20:955-971. doi: 10.1016/j.nicl.2018.10.003. Epub 2018 Oct 4. PMID: 30312939; PMCID: PMC6180343.
Hannanu FF, Zeffiro TA, Lamalle L, Heck O, Renard F, Thuriot A, Krainik A, Hommel M, Detante O, Jaillard A; ISIS-HERMES Study Group. Parietal operculum and motor cortex activities predict motor recovery in moderate to severe stroke. Neuroimage Clin. 2017 Jan 26;14:518-529. doi: 10.1016/j.nicl.2017.01.023. PMID: 28317947; PMCID: PMC5342999.
Kwakkel G, Van Wegen E, Burridge JH, Winstein CJ, van Dokkum L, Alt Murphy M, Levin MF, Krakauer JW. Standardized measurement of quality of upper limb movement after stroke: Consensus-based core recommendations from the Second Stroke Recovery and Rehabilitation Roundtable. Int J Stroke. 2019 Oct;14(8):783-791. doi: 10.1177/1747493019873519. Epub 2019 Sep 11. PMID: 31510885.
Figures
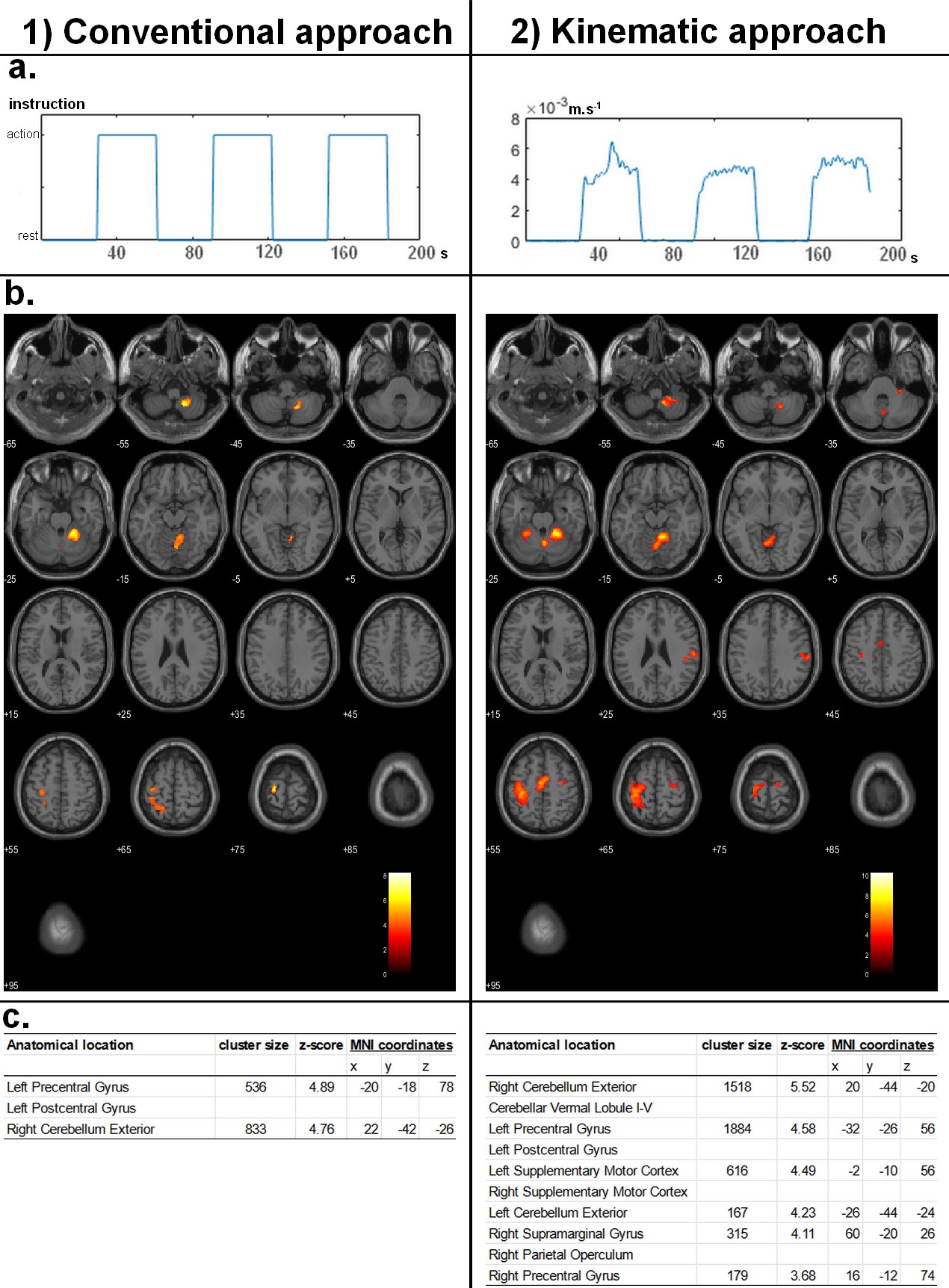
Elbow flexion fMRI results :
1) Conventional approach consisting of regression of BOLD signals with (1.a) periods of action-rest. 2) Kinematic approach consisting of using (2.a) the flexion tangential velocity vector averaged as a regressor. (1.a) represents the velocity averaged vector of the flexion for the first healthy subject as an example. (b) Brain activations overlaid to a T1 anatomical MNI template, obtained by a group-level analysis with a threshold level of p<0.05, FWE corrected at the cluster level, detailed in (c).