3157
Changes in Brain Network Connectivity in Obese Patients Following Weight Loss Surgery Based on Independent Component Analysis1Departments of Radiology, The Third Xiangya Hospital of Central South University, Changsha, China, 2Philips Healthcare, Shanghai, China
Synopsis
Keywords: Functional Connectivity, fMRI (resting state), Obesity, Bariatric surgery
Motivation: Bariatric surgery can rapidly alter obese status, but its effects on resting state functional connectivity (rsFC) in obesity remain unclear.
Goal(s): We examined the effects of bariatric surgery on rsFC between brain networks in obese patients using independent component analysis.
Approach: Thirty obese patients underwent resting state fMRI scans before and after bariatric surgery. We used independent component analysis to analyze surgery-related rsFC changes.
Results: Bariatric surgery improved rsFC of hVN-lFPN, hVN-SMN, AUN-pDMN, AUN-DAN, pVN-aDMN, pVN-SMN, pDMN-SN, aDMN-DAN, and SMN-DAN in obese patients. These results indicate that bariatric surgery induces functional reorganization of brain networks in obesity.
Impact: Bariatric surgery can rapidly alter obese status. Our study investigates the rsFC before and after bariatric surgery, results show that bariatric surgery induces functional reorganization of brain networks in obesity.
Introduction
Obesity involves aberrant multiple brain networks. Bariatric surgery effectively intervenes, directly and sustainably improving somatic function in obesity. However, its contribution to reorganizing obesity-associated resting-state network connectivity remains elusive.Methods
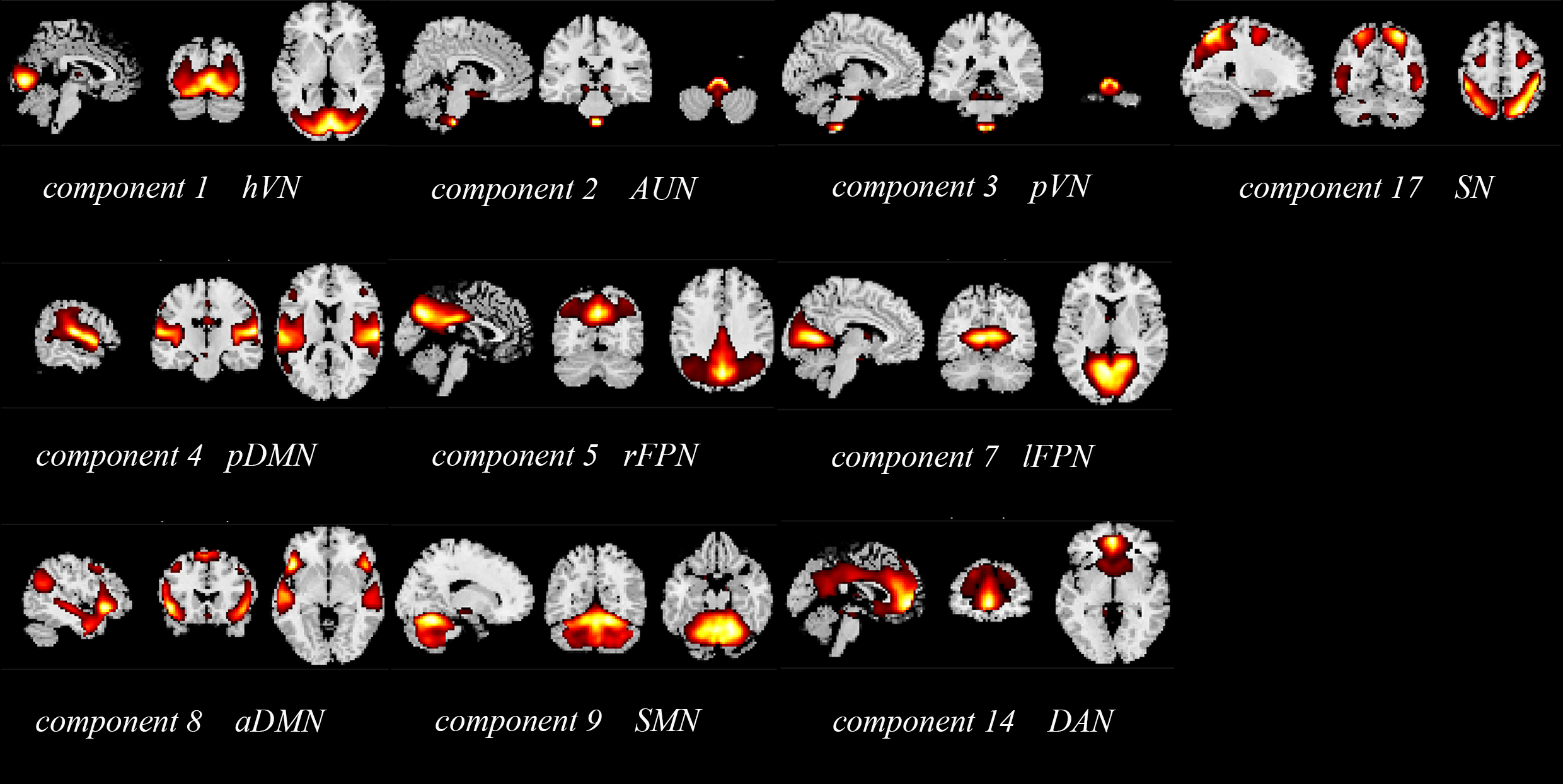
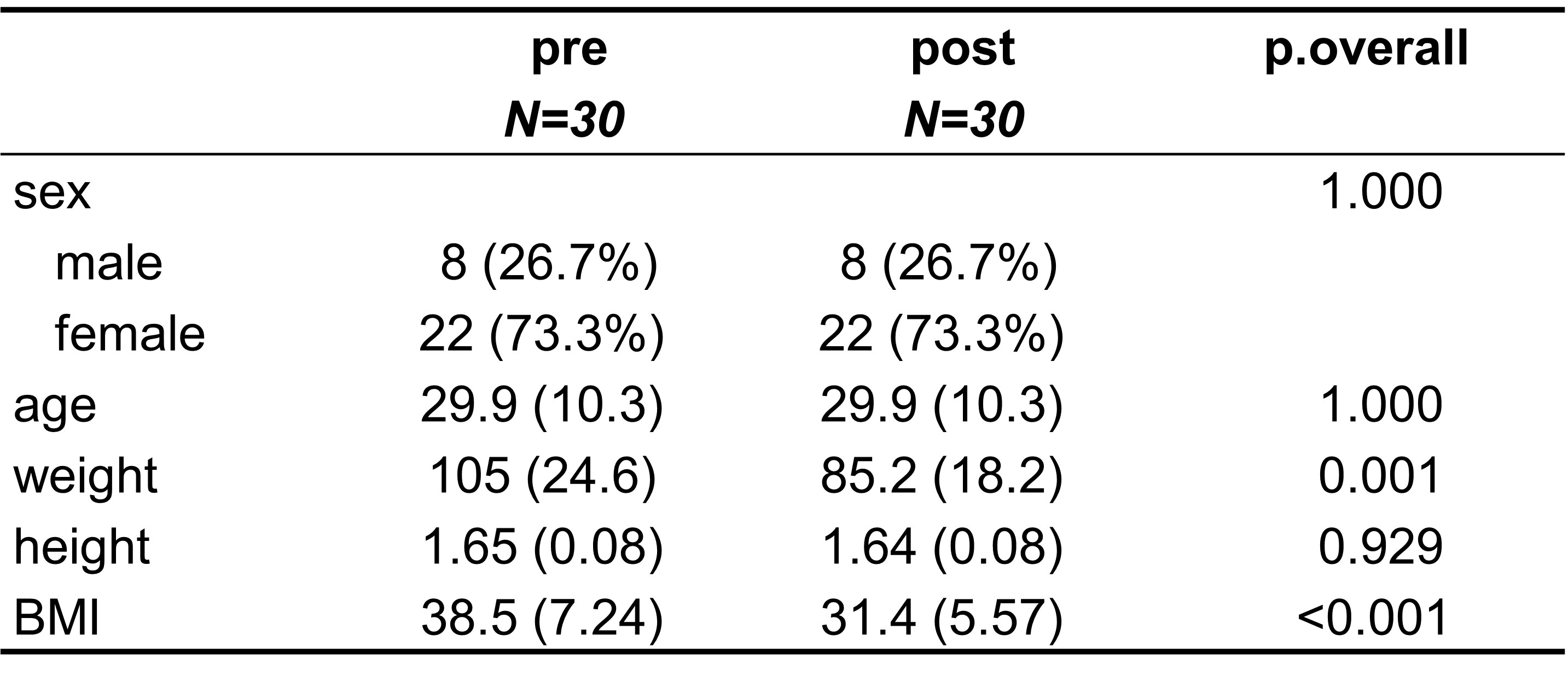
Thirty obese patients undergoing laparoscopic sleeve gastrectomy were recruited at Xiangya Hospital, Central South University, China. Patients with psychiatric/neurological disorders or prior abdominal surgery were excluded. Identical pre- and post-surgery MRI scans were completed 3 months after sleeve gastrectomy. The study was approved by Xiangya Hospital's Ethics Committee and registered at the Chinese Clinical Trial Registry. It adhered to the principles of the Helsinki Declaration. All participants were informed of the study's nature and provided written informed consent. After 12-hour overnight fasting, all participants underwent MRI scans between 6-8 am. Identical measurements were taken at baseline before surgery and 3 months after surgery, with all surgeries performed by the same surgeon (GJ) (Table 1). Images were preprocessed using SPM. Independent component analysis using GIFT software was applied to the images. 10 functional networks were obtained: anterior and posterior default mode networks (aDMN and pDMN), left and right fronto-parietal networks (lFPN and rFPN), salience network (SN), dorsal attention network (DAN), sensory motor network (SMN), auditory network (AUN), primary and higher visual networks (pVN and hVN). Shown in Figure 1.Results
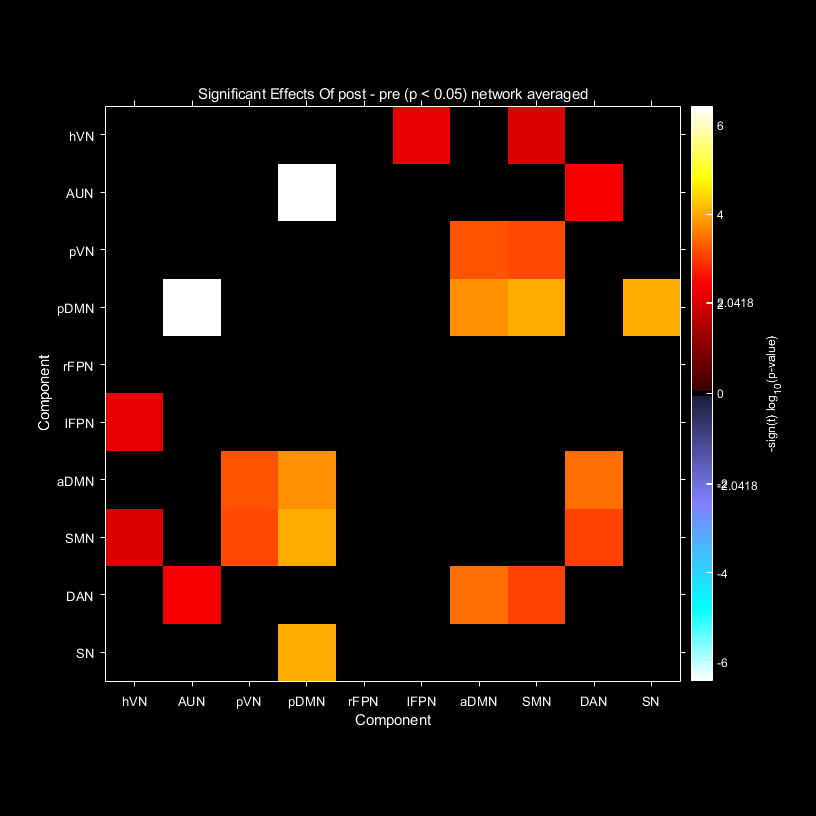
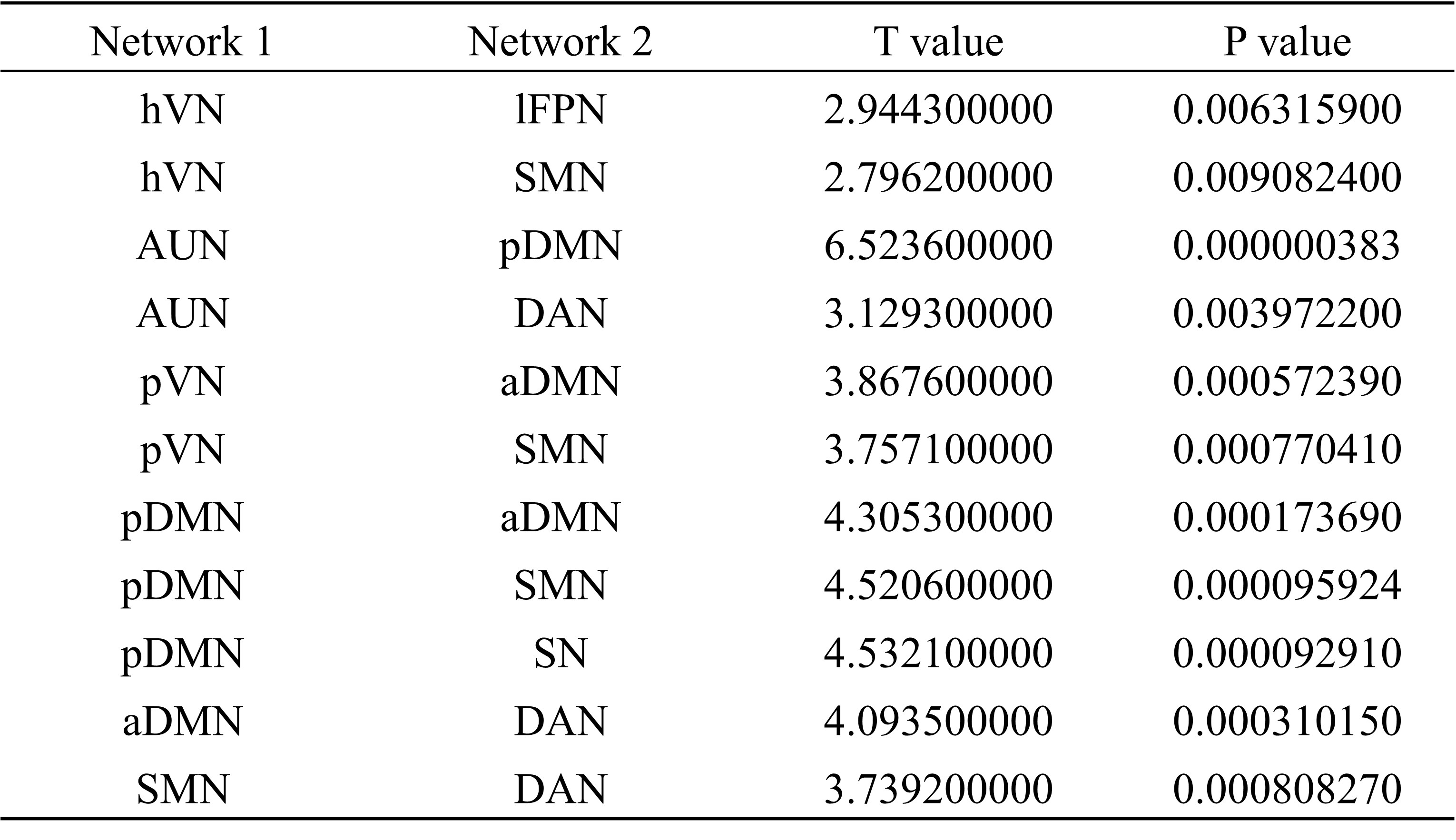
hVN-lFPN, hVN-SMN, AUN-pDMN, AUN-DAN, pVN-aDMN, pVN-SMN, pDMN-SN, aDMN-DAN, and SMN-DAN connectivity showed statistically significant differences, with greater connectivity post-surgery compared to pre-surgery. Shown in Figure 2 and Table 2.Discussion
Bariatric surgery can improve resting-state brain functional network connectivity.We found improved connectivity of hVN-lFPN, hVN-SMN, pVN-aDMN, and pVN-SMN after bariatric surgery. The visual system processes visual information, including primary (V1) and higher-order areas involved in object recognition and motion perception. It functions in food cue processing. Geha et al1. found increased visual cortex whole-brain connectivity in obese vs normal-weight individuals at rest and when drinking milkshakes. Frank et al2 found that after RYGB surgery, lower liking/wanting and eating behavior scores correlated with higher activation in visual, prefrontal, interoceptive, motor, memory, and gustatory regions. Ten Kulve et al3 found decreased reward region activity after RYGB when viewing/tasting food with GLP-1R blockade, increasing activity to food cues. The left fronto-parietal network (L-FPN) exerts broad control over brain information flow, underlying executive functions like goal-directed cognition, working memory, inhibition, and task-switching. The fronto-parietal network is highly associated with eating behavior4,5 and strongly correlates with BMI6. The sensorimotor network underlies motor control and links to reward systems. Disruption can reduce motivation for energy expenditure. Obese individuals may have motor difficulties and altered body image, influencing food and activity behaviors. Decreased connectivity within the SMN has been found in obese patients7.
Connectivity of pDMN-SN and aDMN-DAN was enhanced after compared to before surgery. The DMN includes the medial prefrontal, posterior cingulate, medial temporal, and angular gyri. Studies show increased bilateral wedge frontal lobe and decreased right posterior cingulate cortex functional connectivity within default and temporal networks in obesity8. The salience network includes the dorsal anterior cingulate, insular, and orbital frontal cortices, involved in emotional arousal, reward sensitivity, and decision making9. In the SN, obese participants showed increased functional connectivity strength of the nucleus accumbens at resting state fMRI, and may lead to binge eating through an imbalance between autonomic processing and reward processing of food cues10. The dorsal attention network (DAN) consisting of the frontal eye fields (FEF) and intraparietal sulcus (IPS) showed decreased interoceptive/attentional network and increased visual/salience network functional connectivity in overweight compared to normal weight individuals11.
We found that the connectivity between the auditory network (AUN) and posterior default mode network (pDMN), and between AUN and dorsal attention network (DAN) was enhanced after bariatric surgery. The postprandial increase in GLP-1 (pre- to post-surgery) was associated with reduced RYGB surgery brain activation in the temporal and parietal lobes, and enhanced stimulation of the right ventromedial prefrontal cortex/cingulate, suggesting these attentional and inhibitory regions contributed to augmented satiety signaling after surgery12.
Discussion
In summary, we found that bariatric surgery induced significant rsFC changes across multiple networks in obese patients. Our findings indicate that functional connectivity changes after bariatric surgery in obese patients go beyond interoceptive, default mode, salience, and attentional networks, extending to visual and auditory networks. We speculate these changes may represent adaptive modulatory mechanisms in visual, auditory, interoceptive, motor, attentional, salience, and default mode networks during weight loss. These network connectivity changes elucidate the role of functional homeostasis rebalancing triggered by bariatric surgery, and may help clarify the underlying brain mechanisms during weight reduction.Acknowledgements
No acknowledgement found.References
Figures