3147
Shared and Unique Alterations of Large-Scale Network Connectivity in drug-naïve Adolescent-onset and Adult-onset Major Depressive Disorder1Beijing Anding Hospital,Capital Medical University, Beijing, China, 2Beijing Anding Hospital, Capital Medical University, Beijing, China
Synopsis
Keywords: Functional Connectivity, fMRI (resting state)
Motivation: The motivation is to explore the influence of onset age on large-scale brain networks in MDD patients.
Goal(s): The purpose of this study is to explore the shared and unique alterations of large-scale network connectivity between adolescent-onset and adult-onset MDD.
Approach: This was a single-center cross-sectional study. Volunteers underwent R-fMRI scans. The 2×2 ANOVA was used to analyze the main effects of diagnosis, age and their interaction effect on FCs.
Results: Adolescent-onset and adult-onset MDD have shared and unique large-scale network alterations. The shared altered FCs included VN, LN, VN-DAN VN-LN and LN-DMN. The unique altered FCs included DAN and LN.
Impact: Our findings provide the physiological mechanisms of adolescent-onset and adult-onset MDD for improving clinical subtyping and treatment strategies. The results also suggested that when we explore biomarkers of MDD, we should include onset age as a consideration.
Compared with adult-onset(≥18) Major Depressive Disorder(MDD), adolescent-onset(< 18) MDD is more likely to have a higher risk of mania, more serious symptoms and suicide than adult-onset depression [1,2]. Previous studies suggested that adolescent-onset MDD and adult-onset MDD may differ in clinical symptoms and biological bases, which indicated that age of onset(AOO) may influence clinical subtyping and treatment strategies of MDD[3-5]. However, current studies are lack of direct comparisons between two different AOO groups.
The purpose of this study is to explore whether there are shared and unique alterations of large-scale network connectivity between the two different AOO levels of MDD.
Methods
In this study, a total of 156 volunteers(46 adolescents with MDD, 35 adults with MDD, 19 healthy adolescents and 56 healthy adults) underwent resting-state functional MRI(R-fMRI) scans. All participants were scanned on a 3T MRI scanner(German Siemens Prisma ) with a 64-channel phased-array head coil. Scan parameters are as follows: (1)T1-MPRAGE sequence: repetition time(TR) = 2530ms,echo time(TE) = 1.85ms,flip angle(FA) = 15°, matrix = 256×256,slice thickness = 1 mm,number of slices = 192,FOV = 256 mm×256 mm; (2)EPI sequence: repetition time(TR) = 2000ms, echo time(TE) = 30ms, flip angle(FA) = 90°, matrix = 64×64,slice thickness = 3.5 mm, number of slices = 33, FOV = 200 mm × 200 mm. Subjects were asked to close their eyes during the rs-fMRI scan. The scanning took approximately 20 minutes.
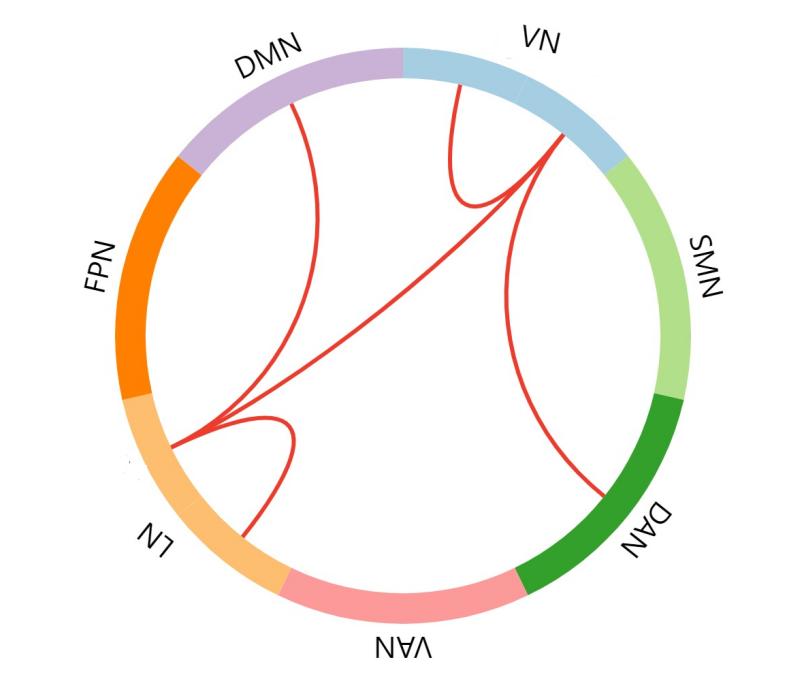
DPABISurf_V1.2 was applied for image preprocessing. Schaefer's functional Atlas defined 400 ROI across the brain[6]. Subsequently, seven cortical networks were generated by matching with Yeo’s seven networks parcellation[7]. The intra-network and inter-network functional connectivity (FC) of 7 major brain networks were calculated, including visual network (VN), sensorimotor network (SMN), dorsal attention network (DAN), ventral attention network (VAN), limbic network (LN), frontoparietal network (FPN) and default mode network (DMN). Then a 2×2 ANOVA was used to analyze the main effects of diagnosis, age and their interaction effect on FCs. NBS was also used to further explore the interaction effect between diagnosis and age on the FC of large-scale brain networks. In addition, correlations were examined between abnormal FCs and HAMD sub-scores.
Results
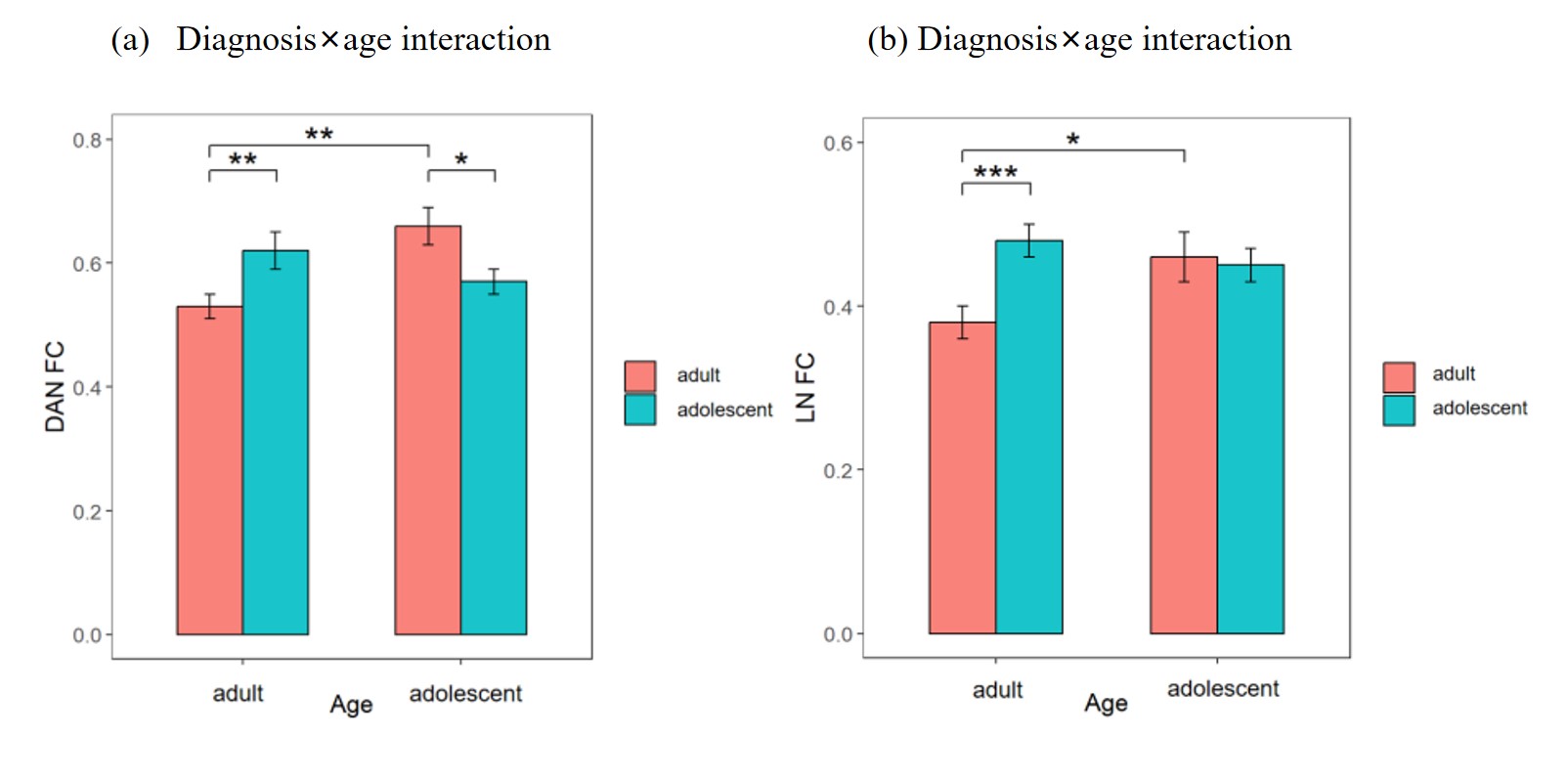
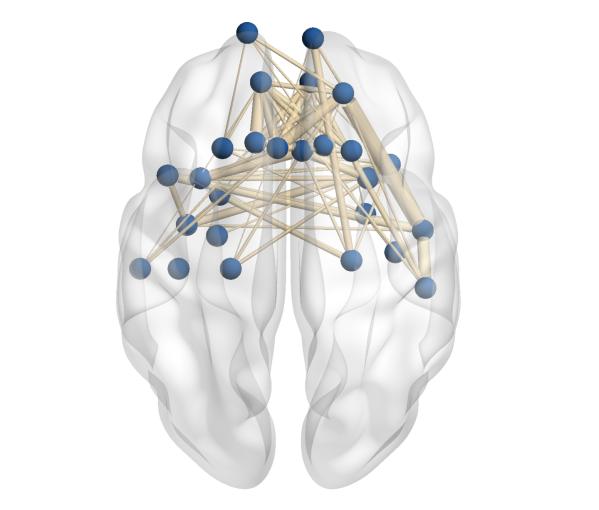
We found the diagnosis main effect on the intra-network FCs of the VN and the LN and the inter-network FCs between the VN and the DAN and between the VN and the LN (F = 6.260,pFDR = 0.046; F = 12.272, pFDR = 0.004 ;Figure 1), indicating that these FC abnormalities were independent of age. Post hoc analysis suggest that all of these FCs were increased in the MDD group. We also found an interaction effect between diagnosis and age on the intra-network FC within the DAN and the LN (F = 10.116, pFDR = 0.013; F = 6.550, pFDR = 0.040; Figure 2). Post hoc analysis showed that both of these intra-network connectivity in adolescent-onset MDD patients were significantly lower than that in the adolescent HCs (p=0.032), whereas this connectivity in adult-onset MDD patients was significantly higher than that in the adult HCs (p = 0.008). The NBS identified that there was an interaction effect of diagnosis and age on FC between components of LN(p=0.0478, corrected; Figure3). The NBS also identified that there was an interaction effect of diagnosis and age on FC between components of LN(p=0.0478, corrected; Figure3). Regression analysis showed that these identified FCs of DAN, VN and VN-DAN were associated with the anxiety somatization scores of HAMD, and the association was more significant in adult-onset MDD.
Discussion
In this study, we explored the large-scale network connectivity abnormalities in drug-naïve MDD patients between adult-onset and adolescent-onset. Our findings indicated that both adolescent-onset and adult-onset MDD have shared and unique Large-Scale network alterations. The shared alterations suggesting that these effects may be explained by depression, and independent of AOO. The unique alterations suggesting that these effects may be specific explained by onset age. Our findings substantiated adolescence as a critical stage of brain development for MDD and might provide neuroimaging support for improving clinical subtyping and treatment strategies. These results can help us gain a deeper understanding of the age-onset-related heterogeneity of MDD from the perspective of brain dysfunction.
Conclusion
Our findings indicated that the adolescent-onset and adult-onset MDD patients have shared and unique large-scale network alterations. These findings are helpful to understand the physiological mechanisms of adolescent-onset and adult-onset MDD for improving clinical subtyping and treatment strategies. The results also suggested that when we explore biomarkers of MDD, we should include AOO as a consideration.
Acknowledgements
No acknowledgement found.References
1. Hu, C., et al., Demographic and clinical differences between early- and late-onset major depressions in thirteen psychiatric institutions in China. J Affect Disord, 2015. 170: p. 266-9.
2. Zisook, S., et al., Factors that differentiate early vs. later onset of major depression disorder. Psychiatry Res, 2004. 129(2): p. 127-40.
3. Kaufman, J., et al., Are child-, adolescent-, and adult-onset depression one and the same disorder? Biol Psychiatry, 2001. 49(12): p. 980-1001.
4. Wang, L., et al., Disturbance of neurotransmitter metabolism in drug-naïve, first-episode major depressive disorder: a comparative study on adult and adolescent cohorts. Eur Arch Psychiatry Clin Neurosci, 2022. 272(7): p. 1283-1296.
5. Zwolińska, W., M. Dmitrzak-Węglarz, and A. Słopień, Biomarkers in Child and Adolescent Depression. Child Psychiatry Hum Dev, 2023. 54(1): p. 266-281.
6. Schaefer, A., et al., Local-Global Parcellation of the Human Cerebral Cortex from Intrinsic Functional Connectivity MRI. Cerebral Cortex, 2018. 28(9): p. 3095-3114.
7. Yeo, B.T., et al., The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J Neurophysiol, 2011. 106(3): p. 1125-65.
Figures