3145
Aberrant functional connectivity of multiple networks in first-episode adolescence-onset major depressive disorder1Department of Radiology, The Second People’s Hospital of Yibin, Yibin, China, 2West China Hospital, Sichuan University, Chengdu, China
Synopsis
Keywords: Functional Connectivity, Psychiatric Disorders, depression,adolescent,network
Motivation: The underlying mechanisms in adolescent-onset major depression disorder (AO-MDD) remains unclear with only few studies in small sample size.
Goal(s): To investigate the alteration of functional connectivity (FC) in multiple networks in AO-MDD patients.
Approach: Seed-based analysis was conducted to detect the FC between AO-MDD group and healthy controls (HCs) at the regional and subregional level.
Results: Hypoconnectivity in AO-MDD was discovered in seeds including insula, amygdala, hippocampus, and their subregions which belong to salience network and affective network. The FC of the right insula and the left hippocampus correlated with the age of onset.
Impact: Our findings provided a comprehensive description of the altered connectivity in multiple networks at regional and subregional levels in AO-MDD pathogenesis. We demonstrated how age of onset contributes to AO-MDD symptomatology.
Introduction
Major depressive disorder (MDD) is predicted to rise to become the world's first burden of disease by 2030 1. The first episode of MDD usually occurs in adolescence. Adolescent-onset major depression disorder(AO-MDD) is defined as the age of onset between 11 and 21years old2,3. The prevalence rate of MDD among adolescents has risen sharply in the past decade4. Which is characterized by chronic and recurrent disease. Seed based functional connectivity(SBFC) is one of the most commonly methods in rest-state functional magnetic resonance imaging(rs-fMRI)analysis to reveal brain connectivity changes. In current study, we selected multiple seeds to explore networks changes at the regional and subregional levels in AO-MDD.Methods
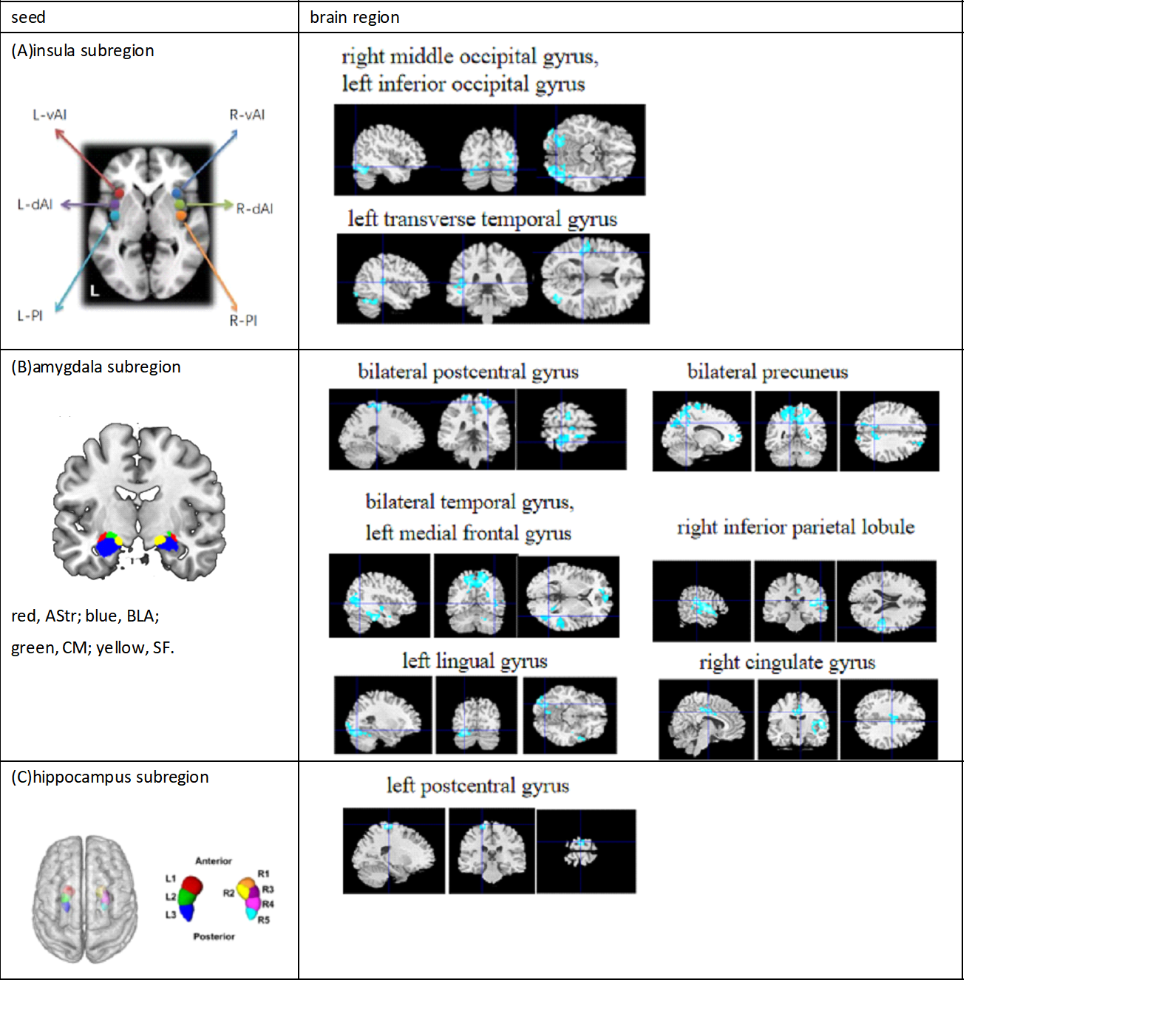
Fifty-two patients with first-episode AO-MDD and fifty-eight HCs were recruited in our study. Each participant was scanned by a 3.0-T Siemens MRI system with a 8-channel phased-array head coil to obtain high-resolution T1-weighted and rs-fMRI images. Neuroimaging data were preprocessed using the DPABI5, including slice-timing, motion correction, co-registeration, regressing out nuisance signals, spatial normalization, smoothing, detrending, and filtering (0.01–0.08Hz). Multiple networks such as default mode network (DMN) including prefrontal cortex (MPFC), bilateral posterior cingulate cortex (PCC), frontoparietal network (FPN) containng bilateral dorsolateral prefrontal cortex (DLPFC), bilateral posterior parietal cortex (PPC) and salience network (SN) including bilateral anterior cingulate cortex(ACC), bilateral insula as seeds to construct functional connectivity. All seeds were defined from the automated anatomical labeling (AAL) atlas or spheres with radius equal to 6 mm based on Montreal Neurological Institute (MNI) spactial coordinates. And subcortical nuclei networks incoporate bilateral amygdala, hippocampus, thalamus, accumbens, caudate, pallidum, putamen also used as seeds. The general linear modal was fulfilled to distinguish group comparisons in rsFC maps of networks in SPM12, with age, sex and head motion as covariates. The significance threshold was set as Puncorrected<0.005 at voxel level and PFWE-corrected<0.05 at cluster level.For the seeds that had between-group differences in seed-based rsFC maps, we further explore the rsFC alterations of these seeds at the subregional level. The insula was divided into ventral anterior insula (vAI), dorsal anterior insula (dAI), posterior insula (PI)6. The amygdala was consisted of amygdalostriatal transition area (AStr), basolateral amygdala (BLA), centromedial amygdala (CM), superficial amygdala (SF)7. The hippocampal subregions were identified as three subregions (L1, L2, L3) and five subregions (R1, R2, R3, R4, R5) in the left and right hemisphere along the anterior–posterior axis8. Analysis of between-group differences in rsFC at subregional level was the same as mentioned above. Partial correlation were used to explore the association between rsFC abnormality and age of onset in AO-MDD subjects in SPSS21. A PFWE corrected<0.05 was considered statistically remarkable.Results
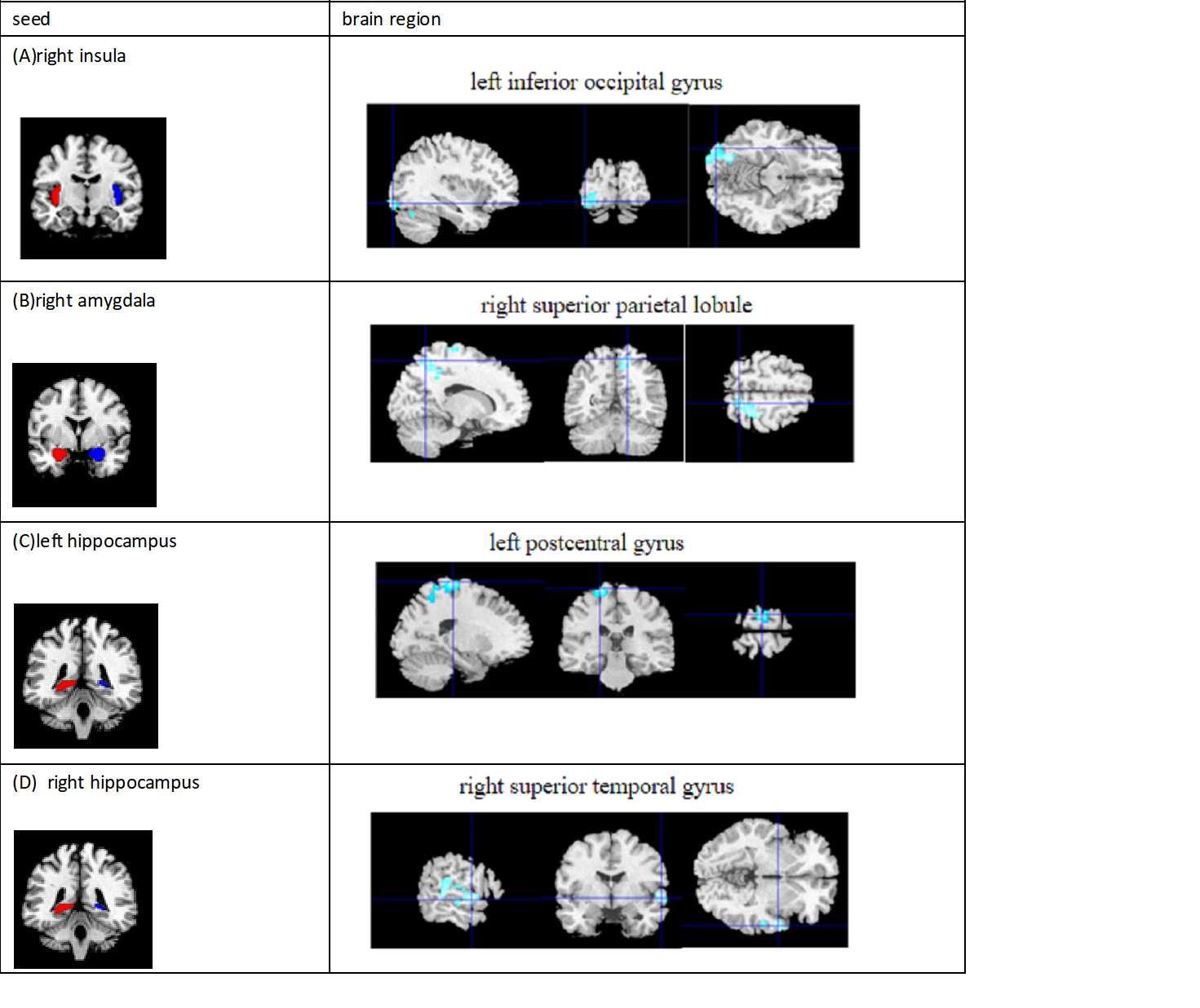
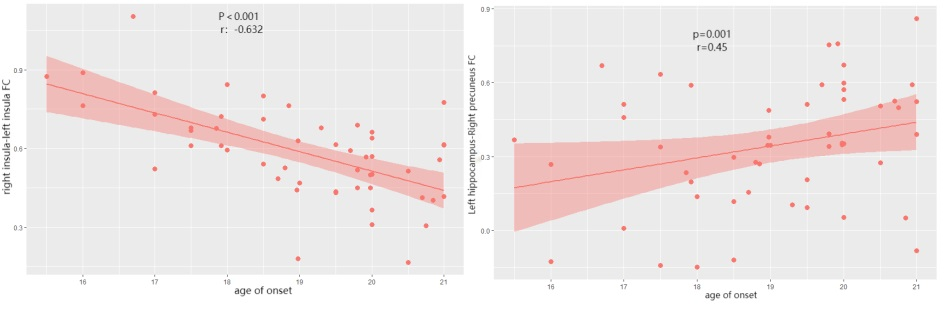
The demographic and clinical characteristics of all participants are presented in Table 1. Table 2 lists all the seeds selected for this study. Significant between-group differences was observed only in rsFC based on the right insula, right amygdala, and bilateral hippocampus (Figure 1). The AO-MDD patients showed significantly lower rsFC between right insula and left inferior occipital gyrus, between left hippocampus and left postcentral gyrus, between right hippocampus and right superior temporal gyrus (STG), and between right amygdala and right superior parietal lobule (SPL). More interestingly, in the AO-MDD group, the rsFC of left hippocampus and right precuneus were positively correlated with age of onset (p=0.001, r=0.45), and the rsFC of bilateral insula were negatively correlated with age of onset(p<0.001, r=-0.632) (Figure 3). As for further analysis at subregional level, there were significant between-group differences in rsFC of the right insula, right amygdala and bilateral hippocampal subregions (Figure 2). Specifically, the hypoconnectivity between right PI with right middle occipital gyrus, left inferior occipital gyrus, and left transverse temporal gyrus, between left AStr-left postcentral gyrus, right AStr-bilateral postcentral gyrus, left CM-left precuneus, left medial frontal gyrus, right middle temporal gyrus, right superior temporal gyrus, right CM- right precuneus, right LB with right inferior parietal lobule, left lingual gyrus, right cingulate gyrus, and between L3 with left postcentral gyrus.Discussion and conclusion
In our study, multiple seeds in networks were selected to investigate the group differences at the regional and subregional levels, and to explore the correlation between age of onset and abnormal FC in AO-MDD group. For all the seeds selected, we only found group difference in salience network(insular as seed) and limbic network(hippocampus and amygdala as seeds). Our findings provided a comprehensive description of the characteristic in connectivity alterations in AO-MDD patients. We also demonstrated how age of onset contributes to AO-MDD symptomatology. Our study may propose potential destinations for diagnosis and individualized intervention strategies of AO-MDD.Acknowledgements
This study is supported by the Natural Science Foundation of Sichuan Province (2022NSFSC0052), National Key R&D Program of China (Grant No.2022YFF1202400), National Natural Science Foundation of China (82372080).References
1. Malhi GS, Mann JJ. Depression. Lancet. 2018;392(10161):2299-2312. 2. Marchitelli R, Paillère-Martinot ML, Bourvis N, et al. Dynamic Functional Connectivity in Adolescence-Onset Major Depression: Relationships With Severity and Symptom Dimensions. Biol Psychiatry Cogn Neurosci Neuroimaging. 2022;7(4):385-396. 3. Ho TC, Gutman B, Pozzi E, et al. Subcortical shape alterations in major depressive disorder: Findings from the ENIGMA major depressive disorder working group. Hum Brain Mapp. 2022;43(1):341-351.4. Thapar A, Eyre O, et al. Depression in young people. Lancet.2022; 400:617-631.5. Yan CG, Wang XD, Zuo XN, Zang YF. DPABI: Data Processing & Analysis for (Resting-State) Brain Imaging. Neuroinformatics. 2016;14(3):339-51. 6. Peng X, Lin P, et al. Insular subdivisions functional connectivity dysfunction within major depressive disorder. J Affect Disord. 2018;227:280-288. 7. Zilles K, Amunts K. Centenary of Brodmann's map--conception and fate. Nat Rev Neurosci. 2010 ;11(2):139-45. 8. Robinson JL, Barron DS, et al. Neurofunctional topography of the human hippocampus. Hum Brain Mapp. 2015;36(12):5018-37.Figures
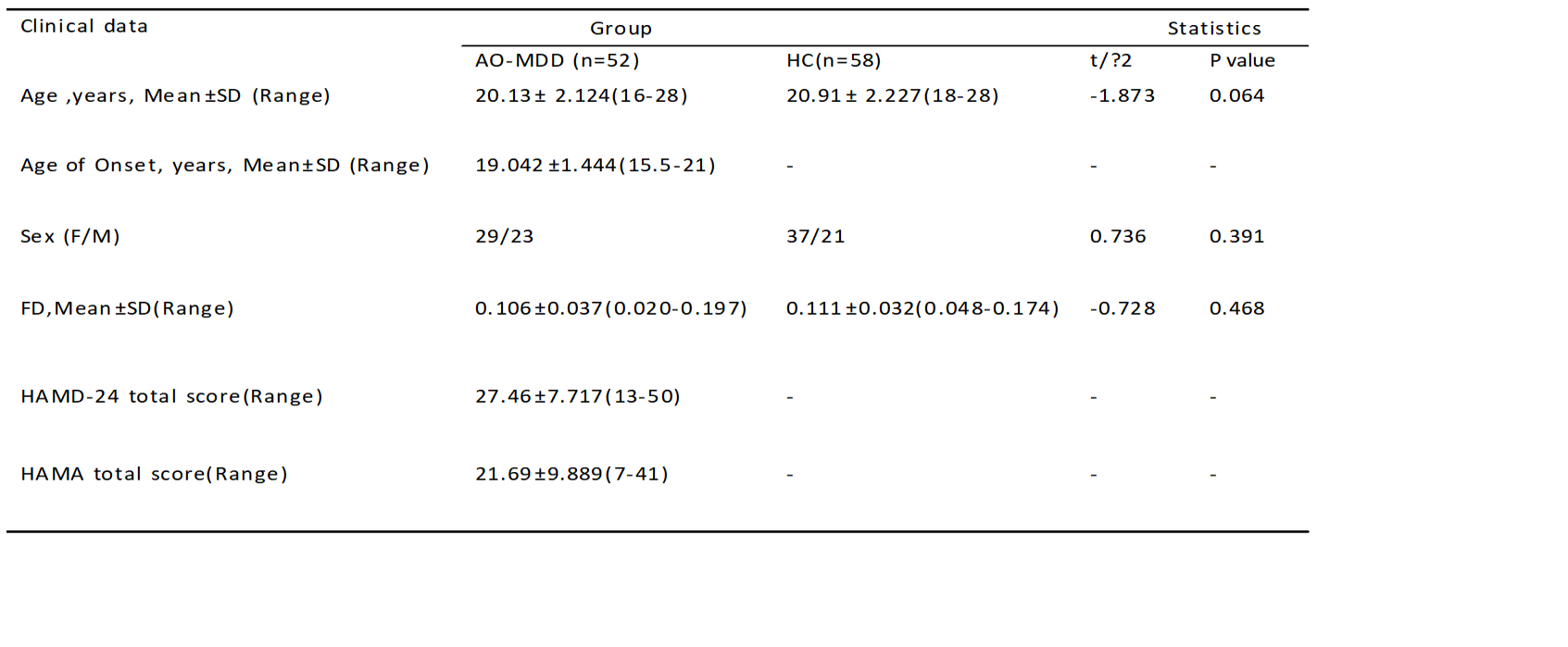
Table 1 demographic,psychometric and rs-fMRI characteristics in AO-MDD and HC group.
Abbreviations:AO-MDD, adolescence-onset major depressive disorder; HC, healthy controls;SD, standard deviation;FD, framewise displacement;HAMD, Hamilton Depression Rating Scale; HAMA, Hamilton Anxiety Rating Scale.
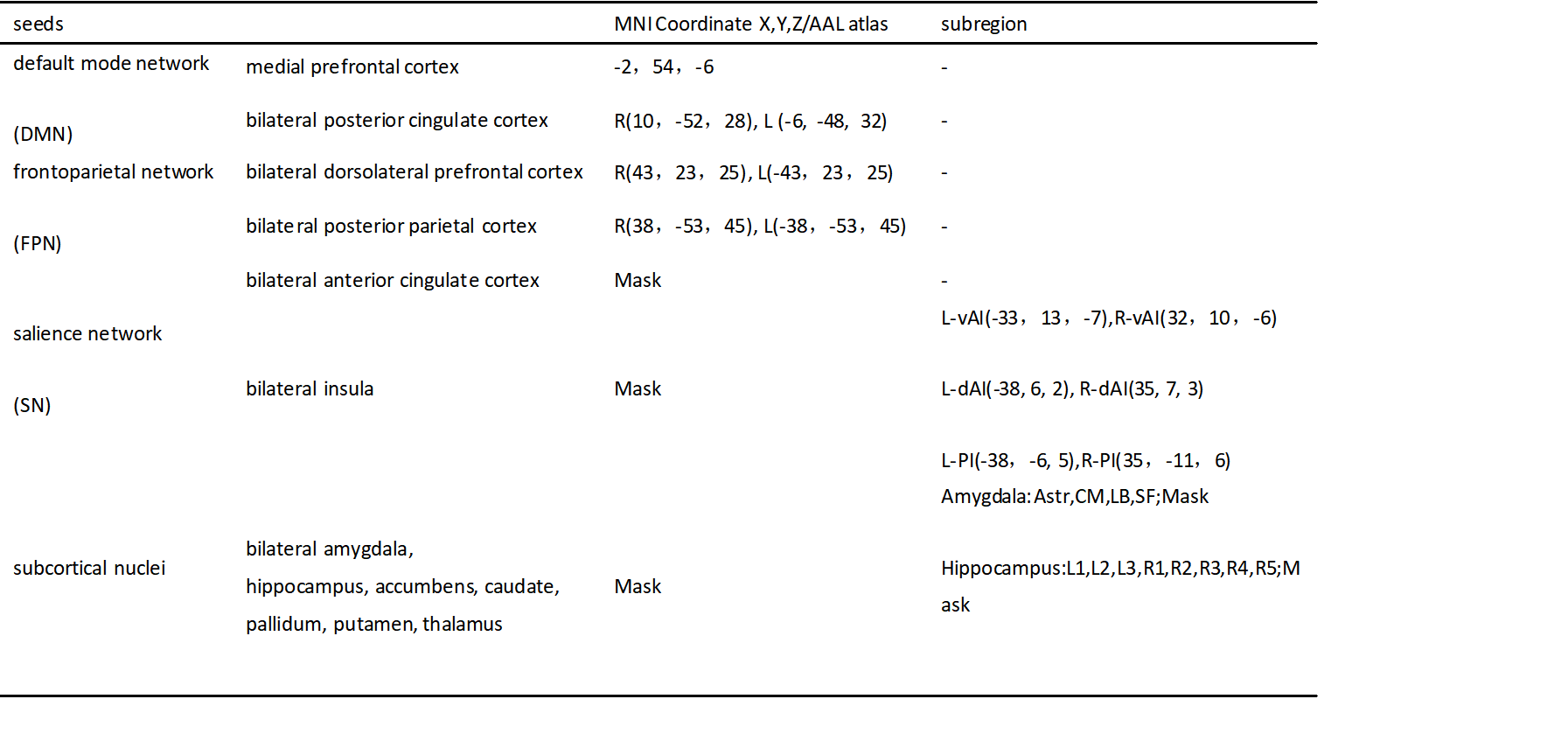
Table 2 The seeds selected in functional connectivity at the regional or subregional levels.
There were group comparison in insula, amygdala, hippocampus,we further investigated FC at subregional level.Abbreviations: MNI, Montreal Neurological Institute; AAL, automated anatomical labeling; L, left; R, right; vAI, ventral anterior insula; dAI, dorsal anterior insula; dPI, dorsal posterior insula; Astr, amygdalostriatal transition area; BLA,basolateral amygdala; CM, centromedial amygdala; SF, superficial amygdala.