3113
High-resolution Organ-axial T2-weighted Improves the Accuracy and Reliability of FIGO Classification of Fibroids1Department of Radiology, Peking University People’s Hospital, Beijing, China, 2Department of Obstetrics and Gynecology, Peking University People’s Hospital, Beijing, China, 3Philips Healthcare, Beijing, China
Synopsis
Keywords: Data Processing, Uterus
Motivation: Limitations of the FIGO classification of fibroid by MRI include interobserver variability, especially for large lesion, leading to distortion of the uterine landmarks.
Goal(s): We aim to evaluate the accuracy and reliability of FIGO type using organ-axial T2WI .
Approach: Organ- and body-axial T2WI were used to identify FIGO classification of fibroids. FIGO types assigned by each radiologist and operation outcome were compared. The association and correlation between FIGO types and cavity compression parameters were analysis.
Results: Organ-axial images showed excellent consistency (kappa=0.877, P=0.04) and accuracy (kappa=0.932, P=0.037) . Compression angle exhibited linear correlation with FIGO types with r of 0.68 (P<0.001) .
Impact: High resolution organ-axial T2 weighted MR could provide exceptional reliability and accuracy in identifying the FIGO classification for uterine fibroid and can be applied to assist in treatment planning and assessing response assessment.
Introduction
Uterine fibroids, represent the most prevalent gynecologic and uterine neoplasm, affecting up to 80% of women by the age of 50 [1]. Implementing the Federation of Gynecology and Obstetrics (FIGO) classification system has facilitated the use of more detailed descriptors to enhance treatment planning and assess response assessment [2]. MRI surpasses the primary examination method, ultrasound, in cases of significant uterine enlargement and in identifying submucosal and subserosal fibroids. However, interobserver variability is constrained by the FIGO classification system identified by MRI, especially in the staging of a large fibroid, which could result in distortion of the landmarks in the uterus [3]. In the evaluation of endometrial cancer assessment, the assessment of myometrial extension is most accurately performed by using high-resolution T2-weighted MRI (T2-WI) acquired along the short axis of the uterus. This approach is recommended by the European Society of Urogenital Radiology (ESUR) [4]. Therefore, the aim of this study is to determine the reliability and accuracy of FIGO for classifying the uterine fibroid by using organ-axial T2-WI imaging.Methods
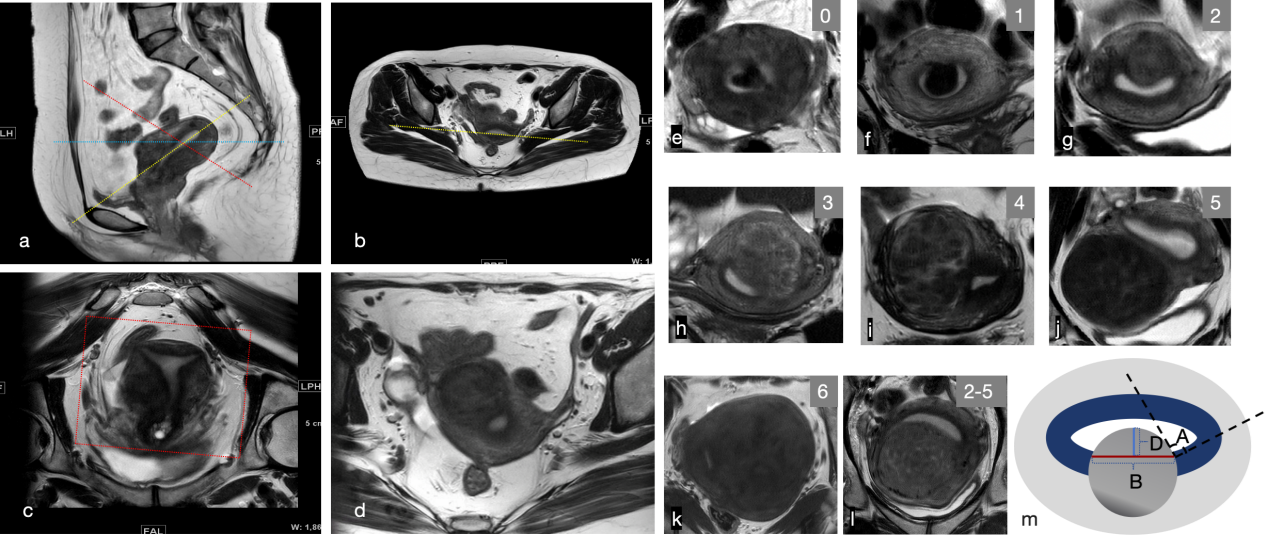
The prospective cohort study involved patients who needed the treatment of symptomatic uterine fibroids from March 2023 to October 2023. All patients underwent laparoscopic or hysteroscopic myomectomy. The FIGO classification of each resected fibroid was identified intraoperatively by a gynecologist. Preoperative magnetic resonance imaging scanning was performed on 3.0 T MRI system (Ingenia, Philips Healthcare, the Netherlands) with a 32-channel body coil. MRI sequences included body-axial T2WI images (sagittal and axial) and organ-axial T2WI images (high resolution with oblique coronal and double oblique axial ) were performed for FIGO classification (Figure1, Table1). The body- and organ-axial images were independently reviewed by two academic radiologists. The third expert radiologist made the final decision if different classification was made. FIGO classifications assigned by each radiologist and operation identification were compared. The association and correlation between FIGO types and uterine cavity deformation parameters were analyzed (Figure 1).Results
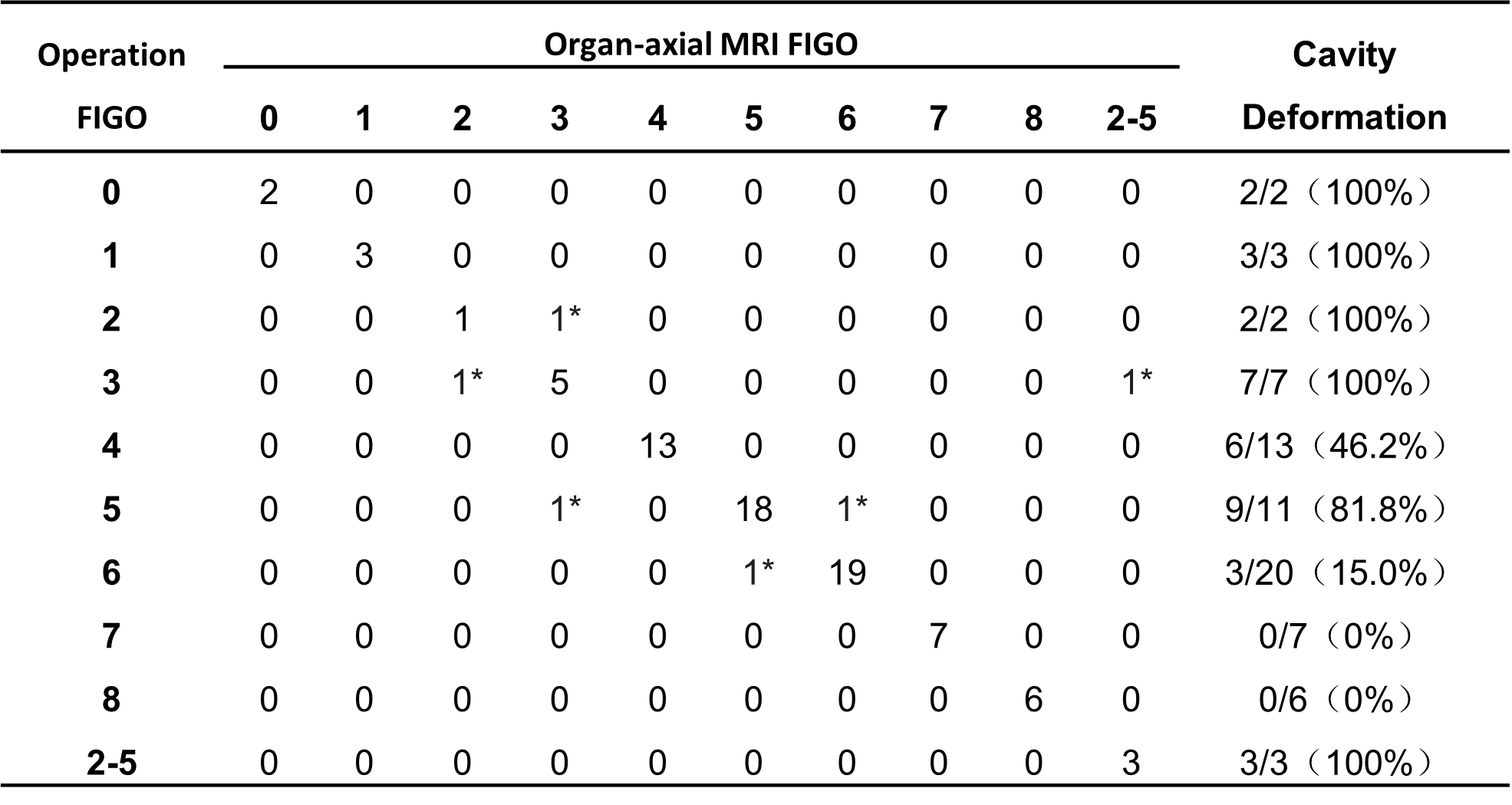
84 fibroids from 73 patients were resected by laparoscopy or hysteroscopy. Organ-axial images showed better consistency and higher match rates with operational descriptions accurately, and the Kappa values were 0.877 (P=0.04) and 0.932 (P=0.037) (Table 2). Only 6 cases were in discrepancy between organ-axial MRI and operation identification (Table 3).32 (38.1%) fibroids showed cavity deformation according to organ-axial MR images, including fibroids with FIGO type 0~7 and 2-5, respectively(Table 3). The imagining characteristics related to cavity deformation are shown in Table 4. Among them, compression angle exhibited a linear correlation with FIGO types, with a correlation coefficient of 0.68 (P<0.001) (Table 4).
Discussion
The consistency between readers regarding the FIGO classification of fibroids based on body-axial MRI was low and had poorer conformity with operation identification. This result was similar to previous literature[3]. In addition, dual-oblique organ-axial MR achieved a high degree of inter-reader agreement and matched with operative assessments. Myometrial extension is most accurately assessed using organ-axial T2WI, which has been recommended by ESUR[4]. While there are no literature reports on the application of organ-axial images in terms of fibroids, our study confirmed that it enhanced the reliability and accuracy of FIGO classification which is similar to endometrial cancer. Furthermore, our results showed the accuracy rate of type 0, 1, 4, 7, and 8 were 100%, respectively. Considering that this classification is meant to assist in the evaluation of abnormal uterine bleeding, which could differentiate submucosal leiomyomas (FIGO 0–2) from other fibroid that do not involve the endometrium (FIGO 3–8) [5]. The challenge lies in distinguishing between types 2, 3, and 2-5.According to previous literature, distortion of the uterine cavity is typically attributed to submucosal fibroids with FIGO type 0,1 and 2 and intramural fibroids with FIGO type 2-5. Conversely, fibroid types that do not distort the uterine cavity, intramural fibroids with FIGO type 3,4,5 and subserosal fibroids with FIGO type 6,7 [2]. Nonetheless, our research found that FIGO types 3-6 have different proportions of signs of uterine cavity compression. In cases of types 0~6 and 2-5 that caused uterine cavity deformation, the compression angle has a linear correlation with the FIGO classification. This indicates the deformation of the uterine cavity gradually transitions from tongue-like protruding to pushing from type 0 to type 6 and 2-5. Furthermore, fibroid-caused physical compression and deformation of the uterine cavity are important mechanisms related to infertility [6]. Our findings imply that an increased number of fibroids may pose a potential risk for sub-fertility, requiring intervention to restore uterine cavity shape.
Conclusion
Given the excellent reliability and accuracy of preoperative FIGO classification, organ-axial T2WI could contribute to treatment planning.Acknowledgements
No acknowledgement found.References
1. Donna Day Baird, David B Dunson, Michael C Hill, et.al. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol. 2003 Jan;188(1):100-7.
2. Malcolm G Munro, Hilary O D Critchley, Ian S Fraser, et.al. The two FIGO systems for normal and abnormal uterine bleeding symptoms and classification of causes of abnormal uterine bleeding in the reproductive years: 2018 revisions. Int J Gynaecol Obstet. 2018 Dec;143(3):393-408.
3. Shannon K Laughlin-Tommaso, Gina K Hesley, Matthew R Hopkins, et.al. Clinical limitations of the International Federation of Gynecology and Obstetrics (FIGO) classification of uterine fibroids. Int J Gynaecol Obstet. 2017 Nov;139(2):143-148.
4. Stephanie Nougaret, Mariana Horta, Evis Sala, et.al. Endometrial Cancer MRI staging: Updated Guidelines of the European Society of Urogenital Radiology. Eur Radiol. 2019 Feb;29(2):792-805.
5. Wendy Tu, Motoyo Yano, Nicola Schieda, et.al. Smooth Muscle Tumors of the Uterus at MRI: Focus on Leiomyomas and FIGO Classification. Radiographics. 2023 Jun; 43(6): e220161.
6. Emma E Don, Velja Mijatovic, Judith A F Huirne. Infertility in patients with uterine fibroids: a debate about the hypothetical mechanisms. Hum Reprod. 2023 Sep 28: dead194.
Figures

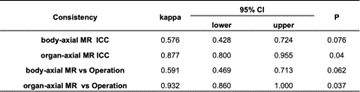
Table 2. Reliability and accuracy of body- and organ-axial MR identified FIGO classification
ICC:intraclass correlation coefficient