3104
MRI-Based Radiomics Analysis to Assess Treatment Response after Neoadjuvant Therapy in Nasopharyngeal Carcinoma1The Second Clinical College, Lanzhou University, Lan Zhou, China, 2Department of Magnetic Resonance, The Second Hospital of Lanzhou University, Lan Zhou, China
Synopsis
Keywords: Radiomics, Tumor, nasopharyngeal carcinoma neoadjuvant chemotherapy
Motivation: Radiomics, as a non-invasive way for analysis of tumor heterogeneity, has been applied to the detection of therapeutic sensibility with satisfactory outcomes.
Goal(s): This study aimed to explore the predictive value of nomogram combing MRI-based radiomics and clinical factors in detecting tumor response to neoadjuvant therapy in nasopharyngeal carcinoma patients.
Approach: LASSO-logistic regression analysis was applied to select radiomics features. The “rms” package was used to construct nomogram and calibration curves. The ROC curves, calibration, and decision curves were performed to assess the performance of the models.
Results: The nomograms integrated radiomics scores with clinical factors outperformed the clinical-only or radiomics-only models.
Impact: The nomogram developed from MRI-based radiomics combined with clinical factors could serve as a reliable tool for non-invasively discriminating neoadjuvant chemotherapy responders from non-responders and provide a basis for personalized therapeutic regimens for LA-NPC patients.
Summary of Main Findings
Our results suggest that the brain glymphatic system is impaired in multiple sclerosis. Impaired glymphatic function was associated with multiple sclerosis-related fatigue. Those findings confirmed that glymphatic system may be involved in the pathogenesis of fatigue in multiple sclerosis patients.Introduction
Nasopharyngeal carcinoma (NPC) is a malignant tumor originating from the nasopharyngeal mucosal epithelium [1]. For locoregionally advanced NPC (LA-NPC), the addition of neoadjuvant chemotherapy (NAC) to concurrent chemoradiotherapy (CCRT) has been shown to decrease the distant metastasis rate and provide survival benefits for NPC patients [2, 3]. Nevertheless, not all patients respond favorably to NAC, Liao et al. reported that 23.1% of the NPC patients were resistant to NAC [4]. Therefore, identifying NAC responders from non-responders for personalized therapeutic options is clinically needed. Radiomics, as an emerging method to analyze tumor heterogeneity, has been applied to the diagnosis, detection of therapeutic sensibility, and gene mutation status of malignant tumors, with satisfactory outcomes [5, 6].Material and Methods
168 patients with pathologically confirmed NPC were retrospectively enrolled and randomly stratified into the training (n = 114) and validation (n = 54) cohorts, at a 7:3 ratio. All patients underwent imaging on a 1.5-T MR scanner (Signa HDx, GE Healthcare, USA), with head and neck coils. More details about scanning parameters were listed in Table 1.We used 3D-Slicer (www.slicer.org, version 4.13.0) to segment the ROIs of NPC lesions manually slice-by-slice on the axial CE_T1WI, and superimposed this onto T1WI and T2WI_FS images. We used “Pyradiomics” package to extract radiomics features and LASSO regression to select features for Rad-Score calculation. Multivariate analysis was performed to select independent clinical predictors. The “rms” package was used to construct the nomogram and calibration curves. ROCs were plotted and AUCs with 95% confidence interval (CI) was calculated to evaluate the performance of different models. Decision curve analysis was used to estimate if the nomogram was sufficiently reliable for clinical use. P < 0.05 indicates a significant difference.Results
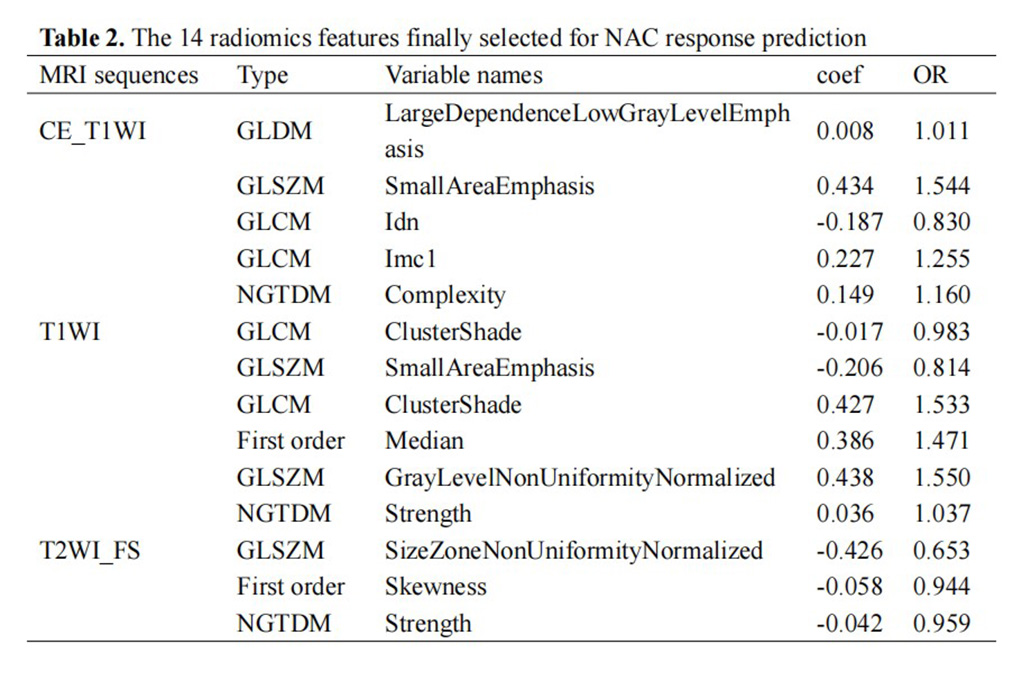
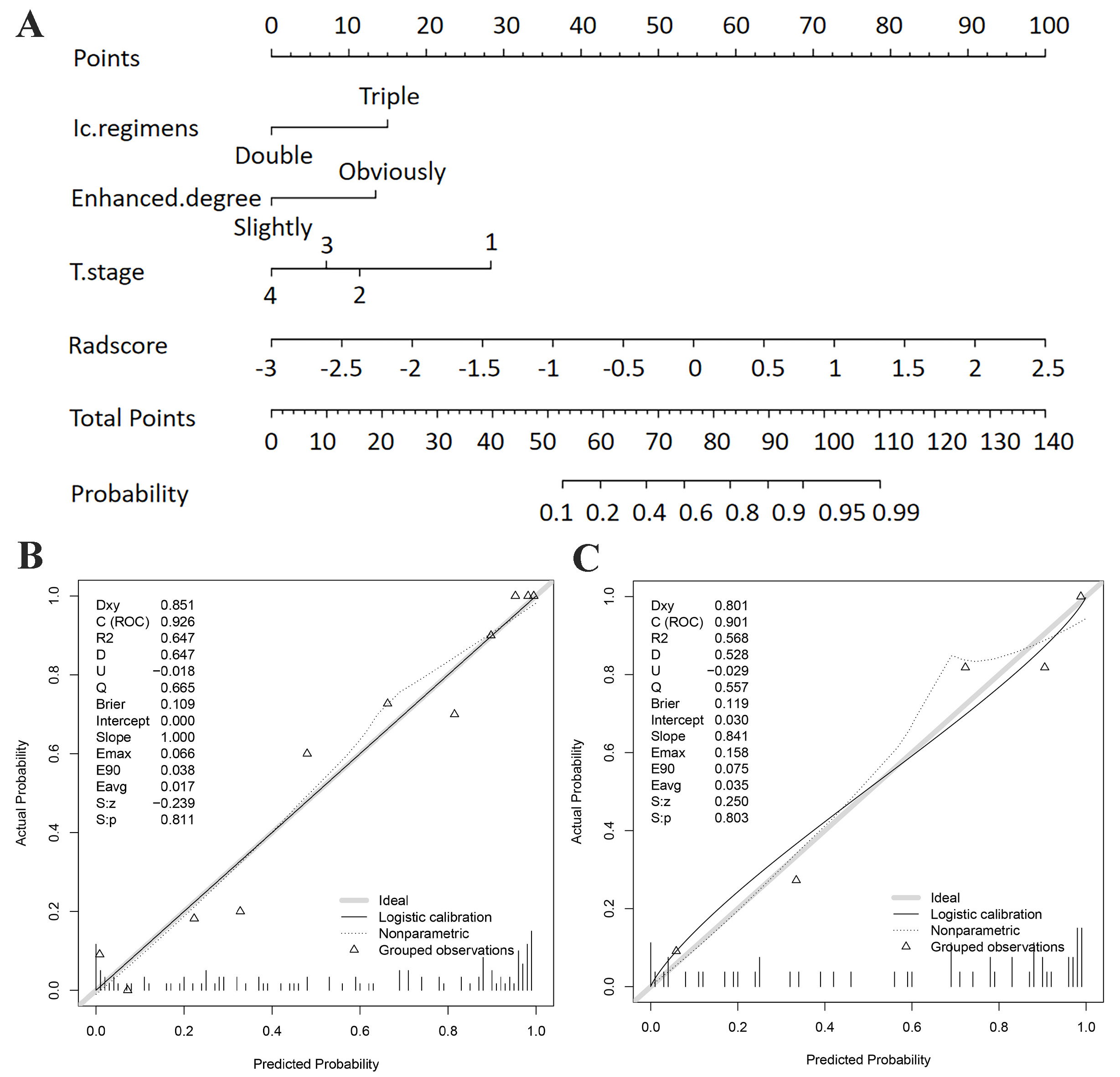
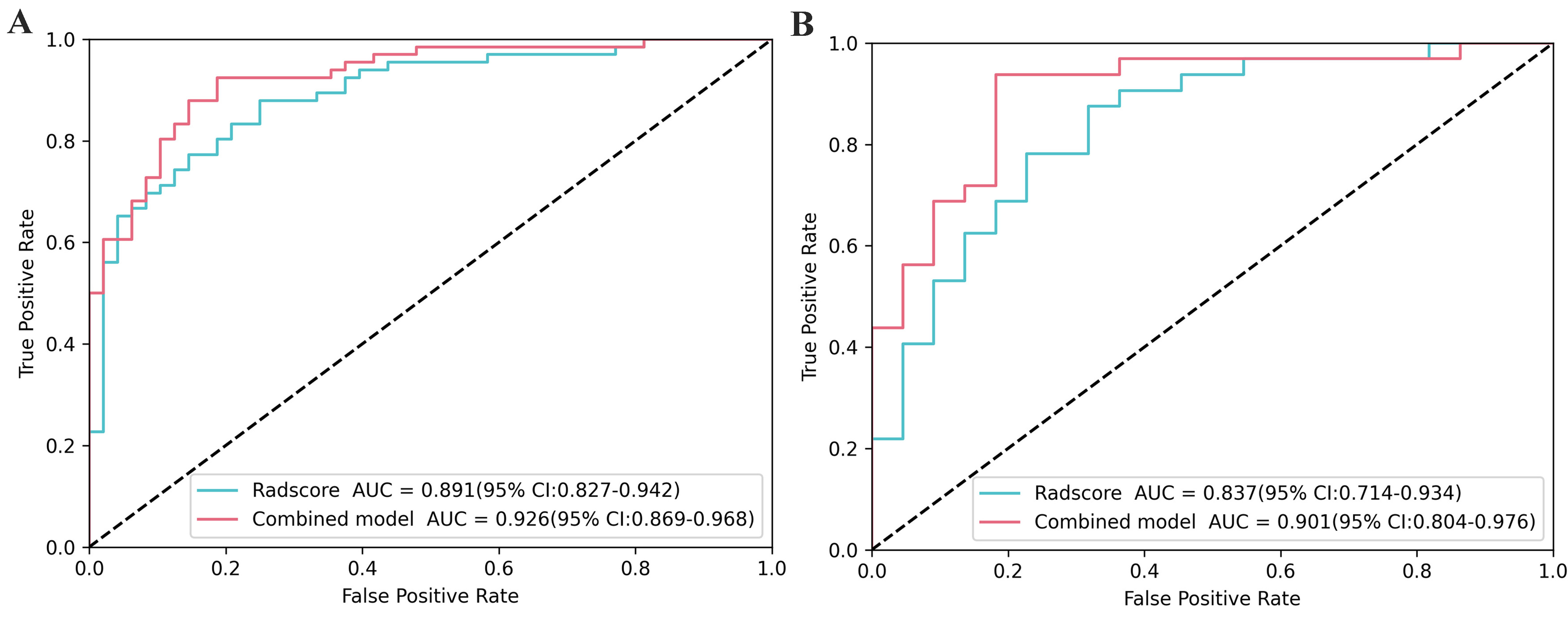
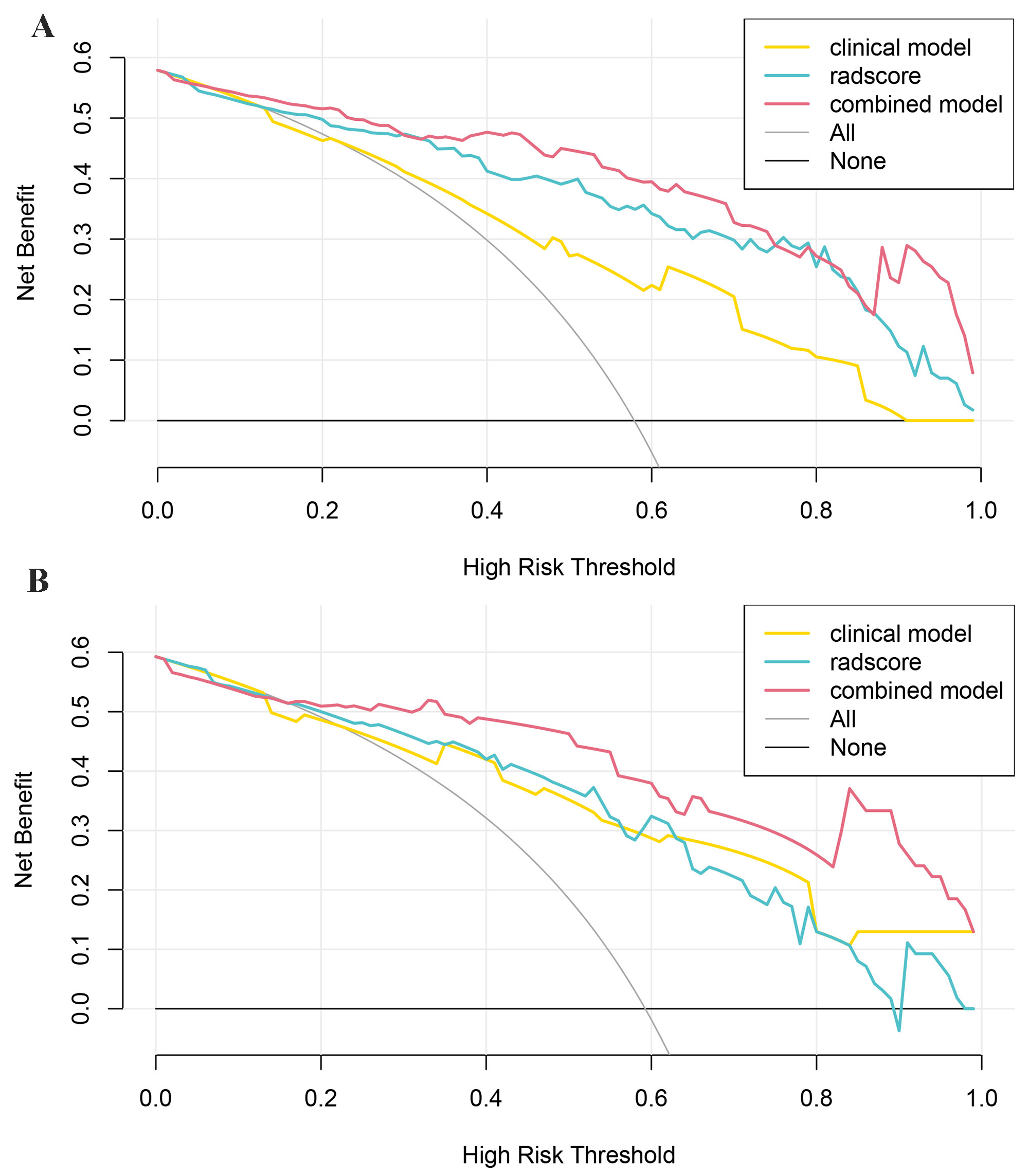
ICT regimens (P = 0.005), T stage (P = 0.004), and enhanced degree (P < 0.001) were identified as the clinical predictors for identifying NAC responders from non-responders. 14 most predictive radiomics features were obtained by LASSO-logistic regression for Rad-Score calculation. As is shown in Figure 1a, a nomogram was developed by integrating the Rad-Score, T stage, ICT regimens, and enhanced degree. The calibration curves demonstrated good agreements between the estimated and observed results in two cohorts (Figure 1b, c). As is shown in Figure 2a, b, the nomogram achieved the best performance as compared to the clinical or radiomics-based model (AUC for training set: 0.926 vs. 0.775, 0.891; for validation set: 0.901 vs. 0.757, 0.837). DCA displayed that applying the nomogram yielded the best clinical benefit compared to using the clinical-only or radiomics-only models at nearly any given probability threshold (Figure 3).Discussion and Conclusion
This study explored the potential value of using nomogram based on multiparametric MRI radiomics combined with clinical features for evaluating the early NAC response status to guide individualized treatment and avoid unnecessary NAC-related side effects. The proposed nomogram model demonstrated better predictive accuracy than models based solely on clinical factors or radiomics. Essentially, it was able to differentiate patients with NPC between favorable and unfavorable responders based on tumor response to NAC. Thus, for subgroups with high sensitivity to NAC, intensive chemotherapy may be an effective strategy and provide survival benefits. Furthermore, other intensive strategies, such as a high dose of radiotherapy [7], immunotherapy [8], or the adoption of EGFR inhibitors [9] may be necessary. On the other hand, for subgroups with low NAC sensitivity, reducing treatment intensity may help avoid unnecessary chemotherapy-induced toxicities, costs, and prolonged wait times for radical radiotherapy. However, notably, further validations with larger sample sizes are required to provide treatment recommendations with more certainty.we extracted radiomics features from multiparametric MR images rather than from single sequence. Therefore, the spatial heterogeneity of the tumor, which is closely correlated with NAC sensitivity, could be fully mined. What’s more, the addition of clinical factors to radiomics greatly improved the predictive performance of the nomogram, which was consistent with the results reported by Hu et al [10]. In conclusion, the nomogram developed from multiparametric MRI-based radiomics and clinical features could serve as a reliable tool for non-invasively evaluating early response to NAC and guide individualized therapeutic regimens for NPC patients.Acknowledgements
Z.W. thanks J.Z. for guidance and advice during the writing process of the article. The authors are grateful to K.A. of Philips Healthcare China for their help with the MRI technique used in this article.References
[1] de Martel C, Georges D, Bray F, et al. Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis. Lancet Glob Health. 2020 Feb;8(2): e180-e190.
[2] Liu W, Yu B, Luo Y, et al. Survival benefit of induction chemotherapy for locally advanced nasopharyngeal carcinoma: prognosis based on a new risk estimation model. BMC Cancer. 2021;21(1):639.
[3] Chen YP, Tang LL, Yang Q, et al. Induction Chemotherapy plus Concurrent Chemoradiotherapy in Endemic Nasopharyngeal Carcinoma: Individual Patient Data Pooled Analysis of Four Randomized Trials. n Clin Cancer Res. 2018;24(8):1824-1833.
[4] Liu SL, Sun XS, Yan JJ, et al. Optimal cumulative cisplatin dose in nasopharyngeal carcinoma patients based on induction chemotherapy response. Radiother Oncol. 2019; 137:83-94.
[5] Liu W, Yu B, Luo Y, et al. Survival benefit of induction chemotherapy for locally advanced nasopharyngeal carcinoma: prognosis based on a new risk estimation model. BMC Cancer. 2021 May 29;21(1):639.
[6] Zhao L, Gong J, Xi Y, et al. MRI-based radiomics nomogram may predict the response to induction chemotherapy and survival in locally advanced nasopharyngeal carcinoma. Eur Radiol. 2020 Jan;30(1):537-546.
[7] Lee AW, Lin JC, Ng WT. Current management of nasopharyngeal cancer.Semin Radiat Oncol. 2012;22(3):233-244.
[8] Yeo ELL, Li YQ, Soo KC, Wee JTS, Chua MLK. Combinatorial strategies of radiotherapy and immunotherapy in nasopharyngeal carcinoma.Chin Clin Oncol. 2018;7(2):15.
[9] Lee NY, Zhang Q, Pfister DG, et al. Addition of bevacizumab to standard chemoradiation for locoregionally advanced nasopharyngeal carcinoma (RTOG 0615): a phase 2 multi-institutional trial. Lancet Oncol. 2012;13(2):172-180.
[10] Hu C, Zheng D, Cao X, et al. Application Value of Magnetic Resonance Radiomics and Clinical Nomograms in Evaluating the Sensitivity of Neoadjuvant Chemotherapy for Nasopharyngeal Carcinoma. Front Oncol. 2021 Nov 1; 11:740776.
Figures
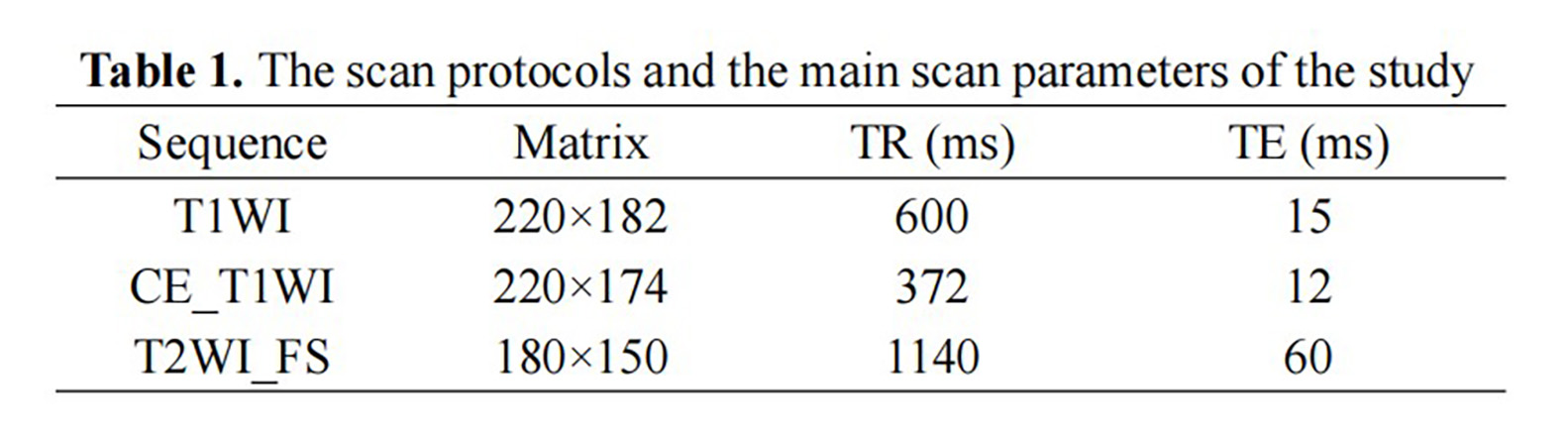
* Abbreviation: CE_T1WI: contrast-enhanced T1-weighted imaging, T1WI, T1-weightedImaging, T2WI_FS, T2-weighted fast suppressed.
** Field of view (FOV): 220 × 220 mm2, slice thickness: 5 mm, slice gap: 1 mm; all images were collected in transverse view.