3100
Novel radiomic models based on DCE MRI for predicting axillary pathologic response in node-positive breast cancer after neoadjuvant therapy1Tianjin Medical University Cancer Institute and Hospital, Tianjin, China, 2Tianjin Medical University General Hospital, Tianjin, China, 3GE Healthcare, Beijing, China, Beijing, China
Synopsis
Keywords: Radiomics, Breast
Motivation: It's essential for breast and axillary conservation surgery decisions by accurately predicting axillary lymph node (ALN) status after neoadjuvant chemotherapy (NAC) in node-positive breast cancer.
Goal(s): We aimed to evaluate the performance of intratumor and peritumor radiomics signature from pretreatment DCE-MRI for predicting ALN pathologic complete response (pCR) after NAC in breast cancer patients.
Approach: We retrospectively collected 175 patients and integrated the clinicopathological features and DCE-MRI radiomics signature for prediction.
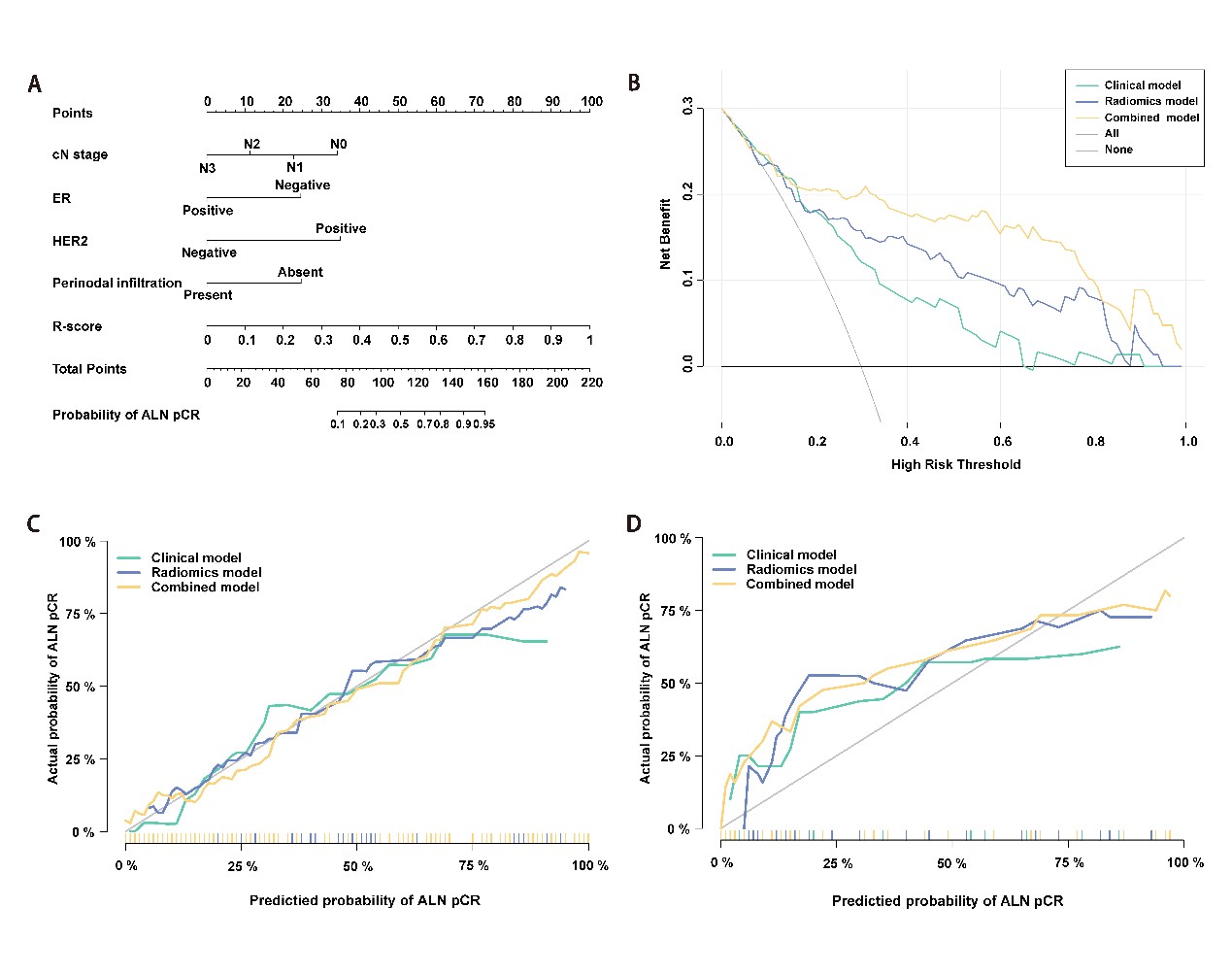
Results: The radiomics score was identified as one of independent predictor for ALN pCR. The factors in the optimal model include initial clinical N stage, ER status, HER2 status, and radiomics score.
Impact: The independent risk factors can provide valuable insights into the patients’ conditions before NAC. The nomogram model may help to identify the candidates who do not necessarily require ALN dissection, thereby facilitating personalized treatment strategies for node-positive breast cancer.
Introduction
Neoadjuvant chemotherapy (NAC) is increasingly employed in breast cancer treatment, aiming to downstage disease and enhance the possibility of breast and axillary conservation surgery1. Most patients with initial axillary lymph node positive (ALN+) breast cancer undergo ALN dissection (ALND) after NAC to evaluate the axillary status, which may cause complications such as lymphedema or arm paresthesia. Sentinel lymph node biopsy (SLNB) has been considered an alternative strategy for patients achieving axillary pathologic complete response (pCR) after NAC (ALN-pCR). And the proportion of patients with ALN-pCR is approximately 40%-60%. However, the feasibility of SLNB post-NAC in initial ALN+ patients remain a concern due to higher false-negative rates (FNRs) of 13%-14%2. Currently, there is no consensus on selecting suitable candidates for SLNB. It has been reported that characteristics of the primary tumor on pretreatment DCE-MRI can be used to predict both the tumor and ALN response after NAC in triple-negative breast cancer3. A previous study indicated that pre-NAC tumor radiomics features may not be informative in predicting the ALN response4. However, these features were only quantified from the first phase of pretreatment DCE-MRI, potentially overlooking spatiotemporal heterogeneity throughout the entire enhancement process. Therefore, we hypothesized that novel radiomic features of the tumor and peritumoral regions, integrating change of spatiotemporal heterogeneity extracted from pretreatment DCE-MRI, could predict the ALN response to NAC.Methods
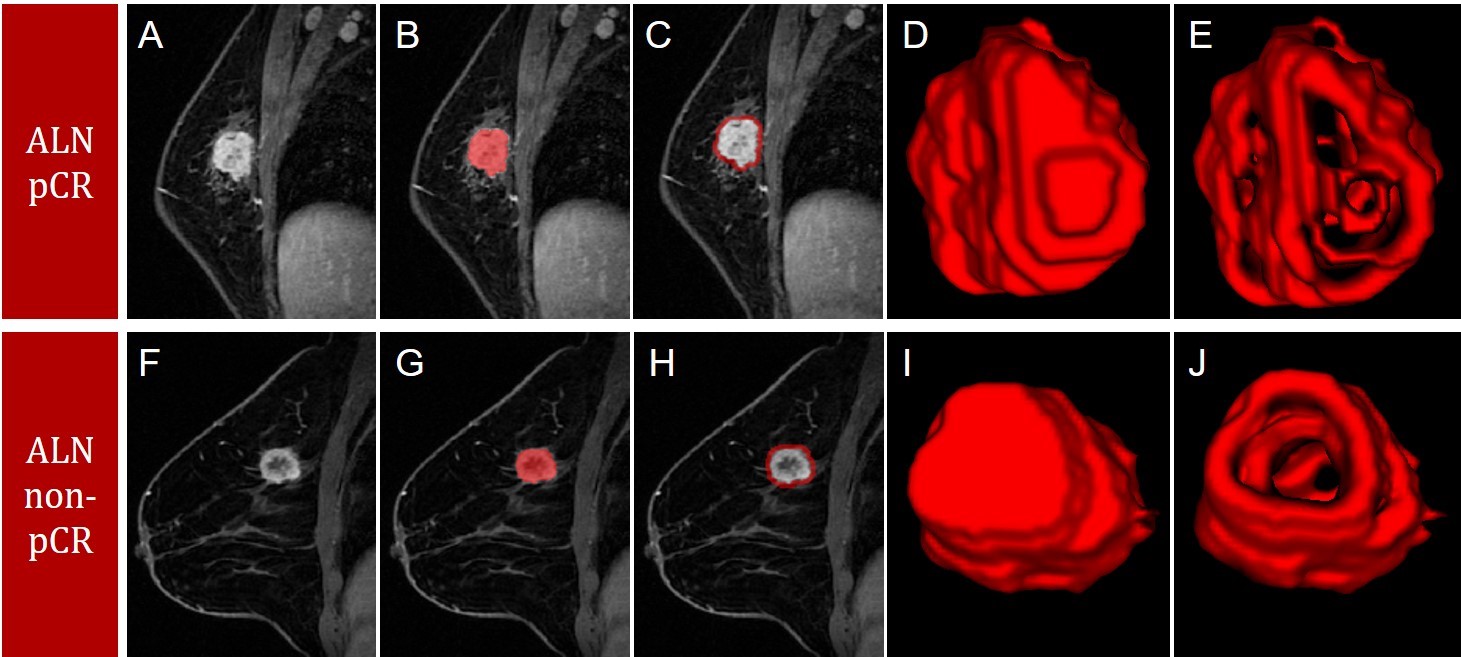
Patients diagnosed with initial ALN-positive breast cancer between January 2017 and December 2019 were retrospectively included if they met the following criteria: (1) they had undergone DCE-MRI (6 phases, 60 seconds per phase) before NAC, and (2) they underwent NAC. The subjects were randomly divided into training and validation cohorts at an 8:2 ratio. Radiomics features were extracted from each phase of DCE-MRI and then the variances of each feature over six phases were calculated as the novel radiomics features. Univariate and multivariate logistic regression analyses were employed to assess the predictors of ALN pathologic complete response (pCR). Three models were developed using clinical and radiomics features from training cohort. The validation cohort was used to validate the models.Results
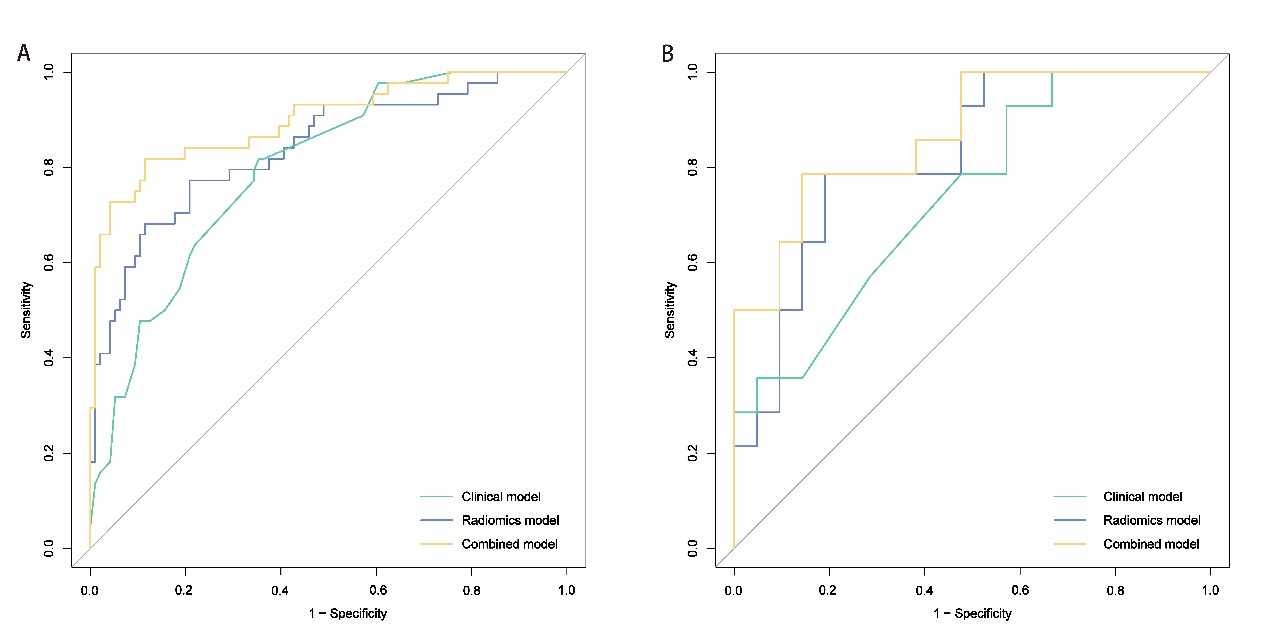
A total of 175 women were included (47.83 ± 10.39 years old). The clinical N stage, ER status, HER2 status, and radiomics score were identified as independent predictors for ALN pCR. Three predictive models were developed, incorporating clinical, radiomics, and combined features. The model with combined features demonstrated the optimal performance, with AUCs of 0.90 (95% CI: 0.84–0.96) and 0.87 (95% CI: 0.75–0.99) in the primary and validation cohorts, respectively.Discussion
In this study, we developed and validated novel radiomics based models that integrated the spatiotemporal information of pretreatment DCE-MRI to predict ALN pCR after neoadjuvant therapy. These models were expected to identify the suitable candidates for sentinel lymph node biopsy. The combined model demonstrated well predictive performance in both the training and validation cohorts. Notably, the top 10 discriminating features from the radiomics features included seven from the peritumoral area, emphasizing the changes in peritumoral intensity and texture heterogeneity during NAC. Hence, it’s crucial to consider both peritumoral and intratumoral radiomics features. Additionally, our study revealed that breast cancers with ER negativity, HER2 positivity, and a lower initial cN stage exhibited higher ALN pCR rates, consistent with previous studies5.Conclusion
The nomogram, integrating novel radiomics and clinical features, exhibited the best performance in predicting axillary response. It has the potential to tailor treatment regimens for patients with initial axillary lymph node-positive breast cancers.Acknowledgements
No acknowledgement found.References
1. Korde LA, Somerfield MR, Carey LA, et al. Neoadjuvant Chemotherapy, Endocrine Therapy, and Targeted Therapy for Breast Cancer: ASCO Guideline. J Clin Oncol. 2021; 39(13):1485-505.
2. Boughey JC, Suman VJ, Mittendorf EA, et al. Sentinel lymph node surgery after neoadjuvant chemotherapy in patients with node-positive breast cancer: the ACOSOG Z1071 (Alliance) clinical trial. JAMA. 2013; 310(14):1455-61.
3. Li Y, Chen Y, Zhao R, et al. Development and validation of a nomogram based on pretreatment dynamic contrast-enhanced MRI for the prediction of pathologic response after neoadjuvant chemotherapy for triple-negative breast cancer. Eur Radiol. 2022; 32(3):1676-87.
4. Drukker K, Edwards A, Doyle C, Papaioannou J, Kulkarni K, Giger ML. Breast MRI radiomics for the pretreatment prediction of response to neoadjuvant chemotherapy in node-positive breast cancer patients. J Med Imaging (Bellingham). 2019; 6(3):034502.
5. Kim R, Chang JM, Lee HB, et al. Predicting Axillary Response to Neoadjuvant Chemotherapy: Breast MRI and US in Patients with Node-Positive Breast Cancer. Radiology. 2019; 293(1):49-57.
Figures