3086
Brain atrophy in epilepsy, a function of etiology? A preliminary analysis1Department for Neurosurgery, Medical University of Vienna, Vienna, Austria, 2Department of Biomedical Imaging and Image-guided Therapy, Medical University of Vienna, Vienna, Austria, 3Division of Neuroradiology and Musculoskeletal Radiology, Medical University of Vienna, Vienna, Austria, 4Department for Neurology, Medical Hospital Hietzing, Vienna, Austria, 5Christian Doppler Laboratory for Clinical Molecular MR Imaging, Medical University of Vienna, Vienna, Austria, 6Center of rare and complex epilepsies, member of ERN EpiCARE, Department of Paediatrics, Medical University Vienna, Vienna, Austria, 7Department for Neurology, Medical University of Vienna, Vienna, Austria, 8NMR Research Unit, Queen Square Multiple Sclerosis Centre, Queen Square Institute of Neurology, University College London, London, United Kingdom
Synopsis
Keywords: Epilepsy, Gray Matter
Motivation: The relationship of grey-matter atrophy in structural epilepsy across various etiologies remains poorly understood.
Goal(s): To perform volumetric brain MRI analysis in the presence of structural epileptogenic brain lesions.
Approach: 68 subjects with structural epilepsy were longitudinally imaged, grey-matter volume estimates were derived from SynthSeg segmentations and corrected for structural lesions with manual segmentation. Grey-matter volume change was assessed over five structural etiological groups and related to the Seizure Frequency Score.
Results: Our data show significant correlation between grey-matter volume loss and the Seizure Frequency Score. We could find no clear trend across etiological groups in our primary analysis.
Impact: Our analysis of grey-matter volume loss in structural epilepsy shows a correlation with the Seizure Frequency Score, supporting the concept of epilepsy-associated neurodegeneration and highlighting the importance of early diagnosis and treatment.
Introduction
Epilepsy is a disabling condition characterized by a wide variety of underlying pathologies, all resulting in the common symptom of seizures. Even though numerous pharmaceutical treatment options are available, one-third of patients still experience pharmaco-resistant epilepsy(1). Surgical intervention may lead to seizure freedom, though often a significant amount of time passes prior to resection. In this period, persistent seizures can lead to cumulative brain damage, either as a direct result of the underlying pathology or due to over-excitation, resulting in glutamate excitotoxicity(2). As recently reviewed, this cumulative damage is associated with progressive brain atrophy in temporal lobe epilepsy(3). However, deciphering the cause of atrophy more closely, namely to which extent it is influenced by the underlying pathology or whether it is predominantly a function of cumulative seizure burden remains unclear. The purpose of this longitudinal study is to offer a comparison of rates of gray-matter volume (GMV) loss in various etiological groups and relate these findings to age, seizure frequency, seizure type and epilepsy duration.Methods
Sixty-eight patients (24±14, 38f,30m, Table 1) with intractable epilepsy were enrolled, who had undergone standardized clinical MRI on at least two time points, a minimum of four months apart (median=17, range= 4-152 months) at our tertiary hospital’s clinic. SynthSeg (4) (Freesurfer v7.4.1) was used to obtain individual patient grey matter volume (GMV) from T1w pre-operative isotropic brain MRI scans. The rate of grey matter volume loss was estimated as the volume difference between the two time points, divided by time (i.e. GMV at follow-up minus GMV at baseline, divided by months). Structural brain lesions were manually segmented on T1 weighted images by neuroradiologically trained readers in consensus and subtracted from the automated brain segmentations to derive comparable GMV between both time points. Prospective clinical data collection and retrospective review was used to obtain patient’s clinical data including seizure types (focal, generalized or both), epilepsy duration (from time point of diagnosis to both brain MRI time points) and seizure frequency, according to the Seizure Frequency Score (SFS) (5) at the time of both MRI sessions and etiology. The etiological groups were based on clinical assessment (consisting of presentation, MRI findings, histopathology or genetic testing) and subdivided into five groups, namely 1. Cortical Disorders (subsuming FCD, MOGHE, mMCD, etc.), 2. Long-Term Epilepsy Associated Tumours (LEATS), 3. Vascular Genesis (AVM, Cavernomas), 4. Hippocampal Sclerosis or TLE and lastly, 5. an MR-negative group with unknown cause of focal epilepsy. Patients with concomitant neurological diagnoses or a history of chemotherapy were excluded. The statistical analysis was conducted R, using parametric and non-parametric methods for group comparisons and correlation analysis as applicable.Results
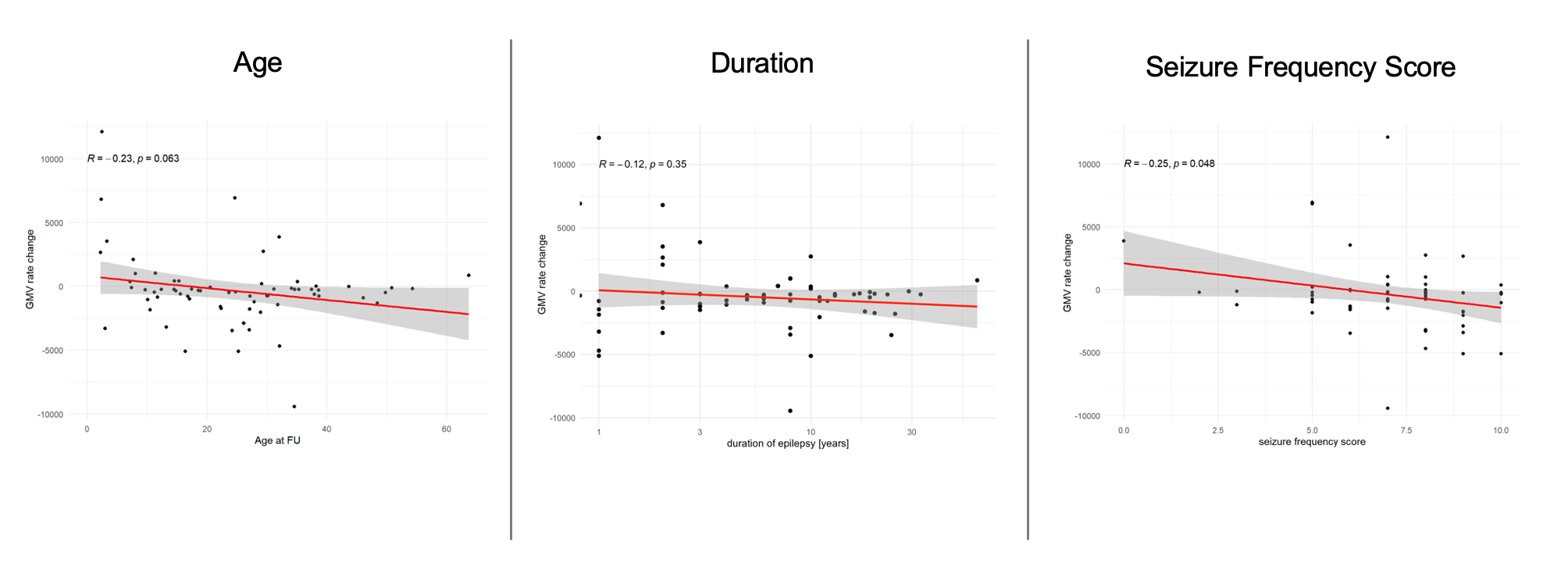
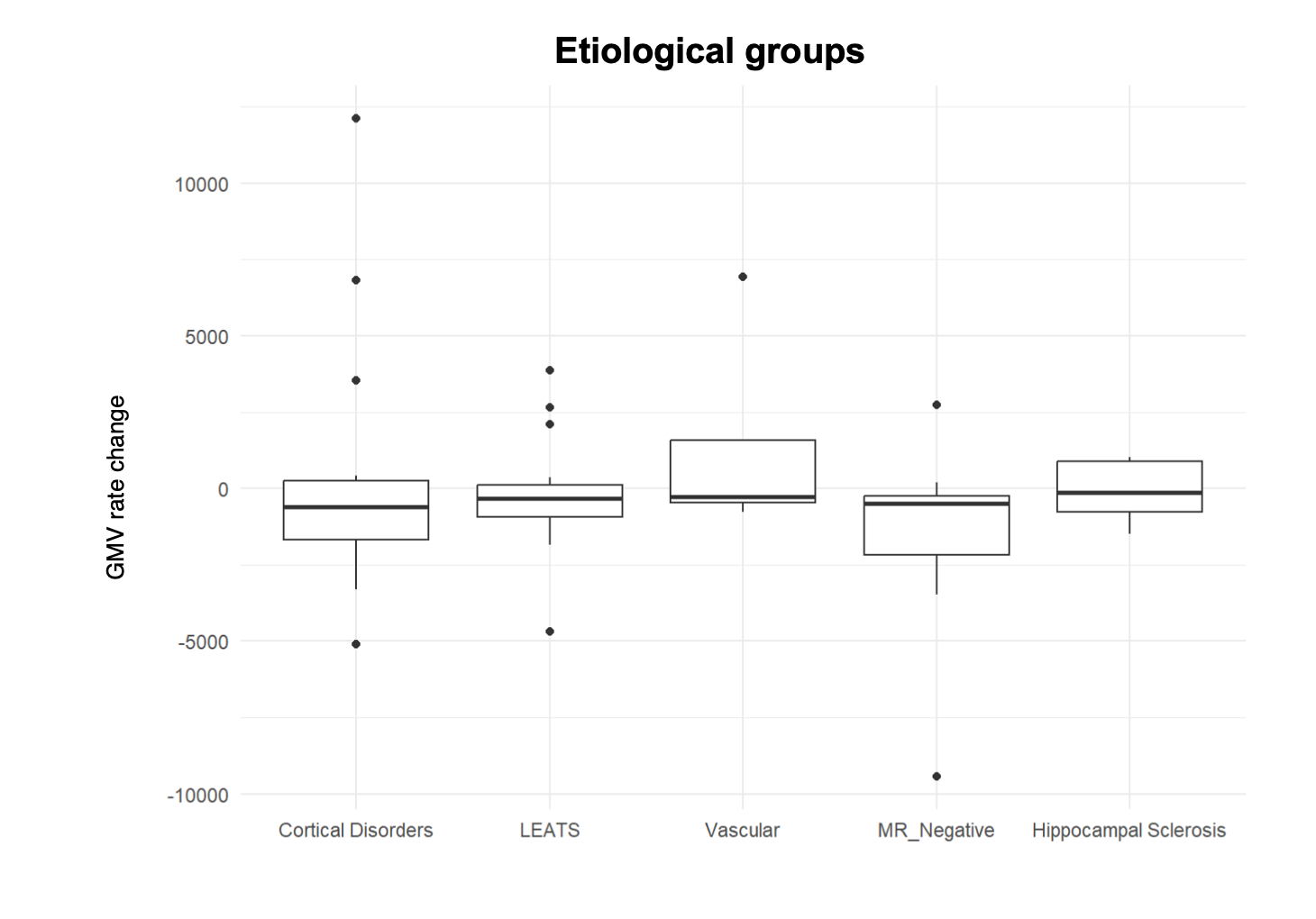
The strongest correlate of GMV loss was the SFS, with higher seizure frequency scores corresponding to increased grey matter volume (GMV) loss (R= -0.25, p= 0.048). A similar trend for GMV was observed in correlation to age (R= -0.23, p= 0.063). Interestingly, despite the age-dependent relationship of brain atrophy, the duration of epilepsy was not associated with GMV loss (R= -0.12, P= 0.35). With respect to the influence of etiology on grey-matter atrophy, we could find no significant differences across the five groups.Discussion
Our preliminary analysis indicates that the rate of grey-matter atrophy in individuals with structural epilepsy is primarily related to seizure burden and age, with etiological factors only playing a minor role. Due to the lack of a control group and limited cohort size, this preliminary analysis only serves as an orientational inter-group comparison within our cohort. Furthermore, seizure amnesia has not yet been taken into account in the course of this analysis, thereby potentially underestimating SFS in some patients. However, this work provides biological evidence for the hypothesis that structural brain changes in the course of epilepsy are driven by seizure frequency rather than the underlying pathologies, supporting the concept of epilepsy-related brain damage and highlighting the relevance for early pharmacological and surgical treatment.Acknowledgements
This study was supported by the Austrian Science Fund (FWF) project KLI 1121. The financial support by the Austrian Federal Ministry for Digital and Economic Affairs, the National Foundation for Research, Technology and Development and the Christian Doppler Research Association is gratefully acknowledged.References
1. Fattorusso, A. et al. The Pharmacoresistant Epilepsy: An Overview on Existant and New Emerging Therapies. Front. Neurol. 12, 674483 (2021).
2. Matute, C., Domercq, M. & Sánchez‐Gómez, M. Glutamate‐mediated glial injury: Mechanisms and clinical importance. Glia 53, 212–224 (2006).
3. Caciagli, L. et al. A meta-analysis on progressive atrophy in intractable temporal lobe epilepsy: Time is brain? Neurology 89, 506–516 (2017).
4. Billot, B. et al. SynthSeg: Segmentation of brain MRI scans of any contrast and resolution without retraining. Med. Image Anal. 86, 102789 (2023).
5. Schäuble, B. et al. Seizure outcomes after stereotactic radiosurgery for cerebral arteriovenous malformations. Neurology 63, 683–687 (2004).
Figures