3079
Parallel transmit (pTx) 7T MRI for drug-resistant focal epilepsy1University of Cambridge, Cambridge, United Kingdom, 2Cambridge University Hospitals NHS Foundation Trust, Cambridge, United Kingdom, 3MRC Cognition and Brain Sciences Unit, Cambridge, United Kingdom, 4Joint Senior Authors, ., United Kingdom
Synopsis
Keywords: Epilepsy, Epilepsy, ptx, UHF
Motivation: In one third of patients diagnosed with drug-resistant focal epilepsy 3T MRI cannot identify the causative lesion. Single transmit (1Tx) 7T MRI is more sensitive, but signal dropouts obscure temporal lobes where lesions often occur.
Goal(s): Show feasibility of parallel transmit (pTx) 7T MRI to identify epileptogenic lesions and compare with circularly polarized (CP) 7T MRI.
Approach: 10 patients with drug-resistant focal epilepsy and normal 3T were scanned with pTx and CP 7T MRI.
Results: : pTx images were more uniform than CP. In three cases epileptogenic lesions (focal cortical dysplasia and encephalocele) that had not been visible at 3T were revealed.
Impact: Parallel transmit (pTx) 7T MRI improves lesion detection in drug-resistant focal epilepsy patients. With further validation, this could contribute to surgical decision making, potentially without requiring invasive depth electrodes tests. This would widen access to curative epilepsy surgery.
Introduction
About 360.000 people in the UK suffer from focal epilepsy [1]. In one third of them anti-seizure medications are ineffective [2]. In that case patients can be freed from seizures by surgery, but one third of MRI scans acquired in conventional field strengths (3T) do not demonstrate the causative lesion [3]. 7T MRI having better SNR, CNR and higher spatial resolution can reveal lesions in patients with negative MRIs acquired at lower fields [3]. However, B1 inhomogeneity in UHF leads to signal dropouts in deeper brain structures, which are frequent locations of brain malformation in epilepsy [4]. Parallel transmit (pTx) can deliver more uniform tissue excitation and thus reduce signal dropouts in temporal lobes. In this study we aim to show feasibility of pTx 7T MRI to find epileptogenic lesions in patients with drug-resistant epilepsy and negative prior 3T MRI.Methods
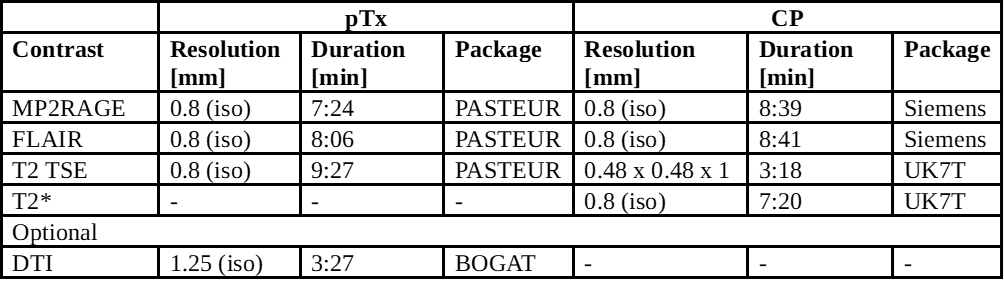
We recruited 11 adult patients with drug-resistant epilepsy on the Cambridge epilepsy surgery pathway into a research study approved by the West Midlands Research Ethics Committee (23/WM/0008). One patient was unable to fit inside the scanner bore because of body habitus, and one interrupted the imaging halfway through the protocol due to claustrophobia, resulting in nine complete and one incomplete dataset. The average age of the scanned patients was 35.2 years (ranging from 19 to 56), 6 females and 4 males. All patients gave written consent to take part in the study.The MRI protocol consisted of both pTx and circularly polarized (CP) – equivalent to 1Tx [5] – sequences (Table 1) including MP2RAGE (resulting in 3D-EDGE and T1-UNI images [6]), FLAIR, volumetric T2 TSE, high-resolution in-plane T2 TSE, T2* and optionally DTI which was acquired last if the patient felt comfortable enough and time permitted (which was the case for 5 out of 10 scanned patients).
The structural pTx sequences used Universal Pulses in the PASTEUR package [7, 8], CP scans used UK7T [9] or Siemens product sequences. For DMRI pTx we used per-subject BOGAT Bayesian pulse optimisation [10].
The acquired images were reported by neuroradiologists and discussed by the multi-disciplinary team (MDT) which integrated the 7T MRI images with 3T MRI, FDG-PET and video-EEG.
Results
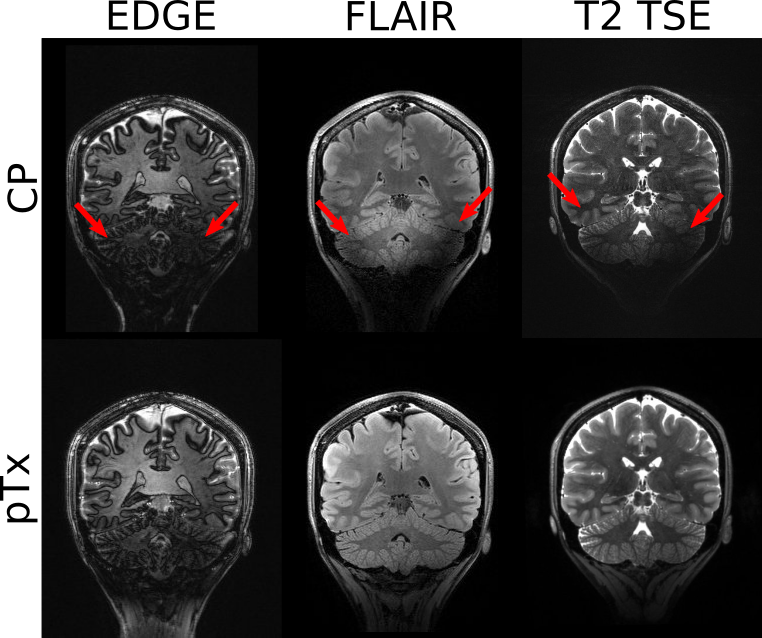
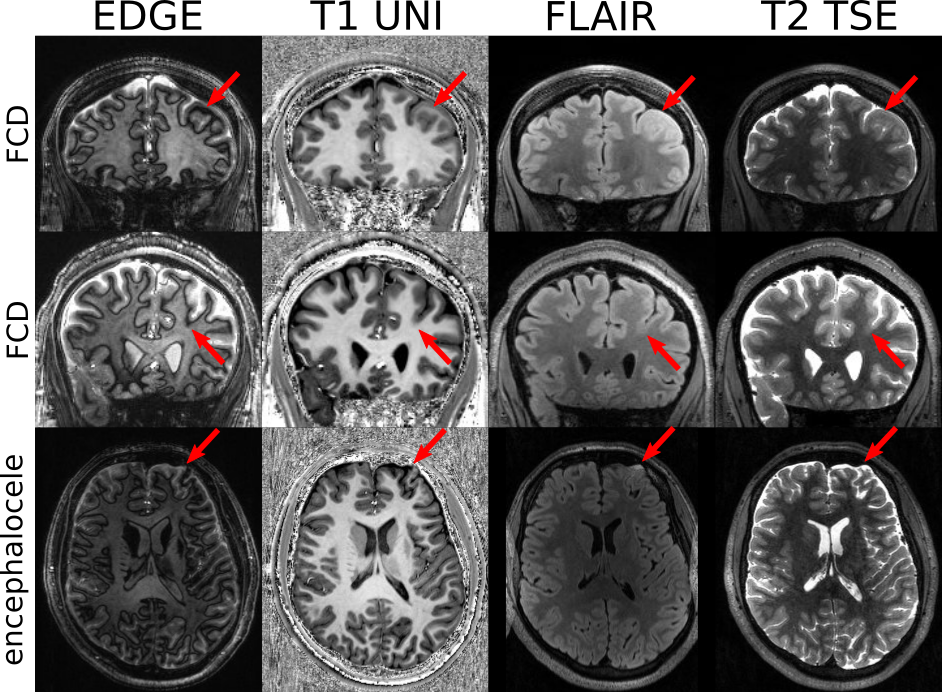
pTx images were more uniform with fewer signal dropouts in the temporal lobes and cerebellum compared to CP images. The biggest differences were visible in EDGE (MP2RAGE first inversion image), FLAIR and T2 TSE images (Figure 1), which are the sequences of highest clinical utility [3].In three out of ten scanned patients we found brain tissue abnormalities that were determined by the MDT to be the cause of their epileptic seizures: Focal Cortical Dysplasia (FCD) in two patients and encephalocele in one patient (Figure 2). In one of the patients with FCD, a previous 3T MRI scan suggested presence of hippocampal dysplasia, which was disproved by the 7T scan. In all cases, the novel imaging findings significantly changed clinical management.
Diffusion scans completed successfully in 5 patients. To minimise scan time we acquired a slab covering only the lower part of the brain. One patient with FCD also had diffusion MRI, but unfortunately the lesion was located beyond the diffusion FOV.
Discussion and Conclusion
In this study we showed that UP pTx sequences visibly improve uniformity of the images in temporal lobes and cerebellum. We also demonstrated a 30% increased yield of UHF MRI over 3T MRI for epileptogenic lesions, in line with theoretical expectations [3]. However, these three abnormalities were all in frontal rather than temporal lobe, and their detection was aided by hypometabolism on FDG-PET. Improved analysis and reporting mechanisms will be an important next step in maximising the utility of the large amount of data generated by UHF imaging.pTx 7T MRI is feasible in patients with drug-resistant focal epilepsy. It visibly improves image uniformity in temporal lobes and cerebellum compared to CP 7T MRI. This is important because epilepsy lesions often occur in the temporal lobes. We have just received funding to scan a further 25 patients for a statistically powered comparison.
Conflict of interest
CTR discloses research grant support from Siemens, for a different project.Acknowledgements
This study was funded by the MRC (MR/X502844/1), with additional support from the Addenbrooke’s Charitable Trust and the NIHR Cambridge Biomedical Research Centre (NIHR203312 and BRC-1215-20014).
M.Z. is supported by the Medical Research Council (MRC N013433-1) and the Cambridge Trust.
The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. For the purpose of open access, the authors have applied a CC-BY public copyright licence to any Author Accepted Manuscript version arising from this submission.
We thank the WBIC radiographers for scanning the patients. We thank Neurospin Paris for sharing their PASTEUR pTx pulse sequence package. We thank Iulius Dragonu and Belinda Ding for IDEA programming assistance.
References
1. NICE, Epilepsies: diagnosis and management. Clinical guideline (NG217). 2022.
2. Mesraoua, B., et al., Drug-resistant epilepsy: Definition, pathophysiology, and management. Journal of the Neurological Sciences, 2023. 452: p. 120766.
3. Opheim, G., et al., 7T Epilepsy Task Force Consensus Recommendations on the Use of 7T MRI in Clinical Practice. Neurology, 2021. 96(7): p. 327-341.
4. Chambers Stefanie, et al. Quantification of Lesion Volume Differences in Structural Epilepsy in 7T and 3T. in ISMRM Annual Meeting 2023. 2023. Toronto, Canada.
5. Ding, B., et al., Parallel transmit (pTx) with online pulse design for task-based fMRI at 7 T. Magn Reson Imaging, 2022. 93: p. 163-174.
6.
Middlebrooks, E.H., et al., Improved
detection of focal cortical dysplasia using a novel 3D imaging sequence:
Edge-Enhancing Gradient Echo (3D-EDGE) MRI. Neuroimage Clin, 2020. 28: p. 102449.
7. Le Ster, C., et al., Standardized universal pulse: A fast RF calibration approach to improve flip angle accuracy in parallel transmission. Magnetic Resonance in Medicine, 2022. 87(6): p. 2839-2850.
8. Massire, A., et al., PASTEUR: Package of Anatomical Sequences Using Parallel Transmission Universal Pulses Now Available for MAGNETOM Terra. MAGNETOM Flash, 2022. 1(80).
9.
Clarke, W.T., et al., Multi-site
harmonization of 7 tesla MRI neuroimaging protocols. Neuroimage, 2020. 206: p. 116335.
10. Zhang, M. and C.T. Rodgers, Online gradient optimisation for spokes parallel transmit – the BOGAT method, in ISMRM 2023. 2023.
11. Yushkevich, P. Greedy. [cited 2023 05.07.2023]; Available from: https://github.com/pyushkevich/greedy.
Figures