3062
A data-driven approach for improved quantification of in-vivo metabolic conversion rate of hyperpolarized [1-13C]pyruvate1Department of Radiology and Biomedical Imaging, University of California, San Francisco, CA, United States, 2Department of Neurological Surgery, University of California, San Francisco, CA, United States
Synopsis
Keywords: Data Processing, Hyperpolarized MR (Non-Gas)
Motivation: Accurate quantification of metabolism in hyperpolarized (HP) 13C MRI is essential for clinical application. However, kinetic model parameters such as flip angle are often uncertain, leading to model mismatch.
Goal(s): We aimed to develop a data-driven approach to quantify the HP pyruvate-to-lactate conversion rate (kPL) for with improved accuracy.
Approach: To validate our method, we conducted numerical simulations and animal studies with HP 13C-pyruvate and applied this method to human abdominal data.
Results: Our findings revealed that the data-driven kinetic fitting method can improve model-data fits by correcting flip angle and relaxation errors, resulting in more accurate kPL determination.
Impact: Using the new data-driven kinetic fitting method to quantify HP 13C-pyruvate metabolism, accurate kPL can be obtained even in the presence of B1 inhomogeneity. This improvement may prove to be clinically valuable in improving tumor staging or assessing treatment-response.
Introduction
Clinical translation of hyperpolarized (HP) [1-13C]pyruvate MRI has been applied to numerous applications in the brain, heart, prostate, and abdominal organs1. Using pharmacokinetic modeling, the conversion of pyruvate to lactate (kPL) can be quantified as a potential biomarker of abnormal metabolism. However, determining an accurate kPL is challenging due to B1 field inhomogeneities across the imaging volume, which results in inconsistencies between the data and kinetic model that can bias kPL2. To overcome this limitation, we explored a data-driven kPL fitting method that compensates for uncertainties in the measured flip angles. We tested this method in simulations, pre-clinical and human abdominal data to improve the accuracy of kPL determination.Methods
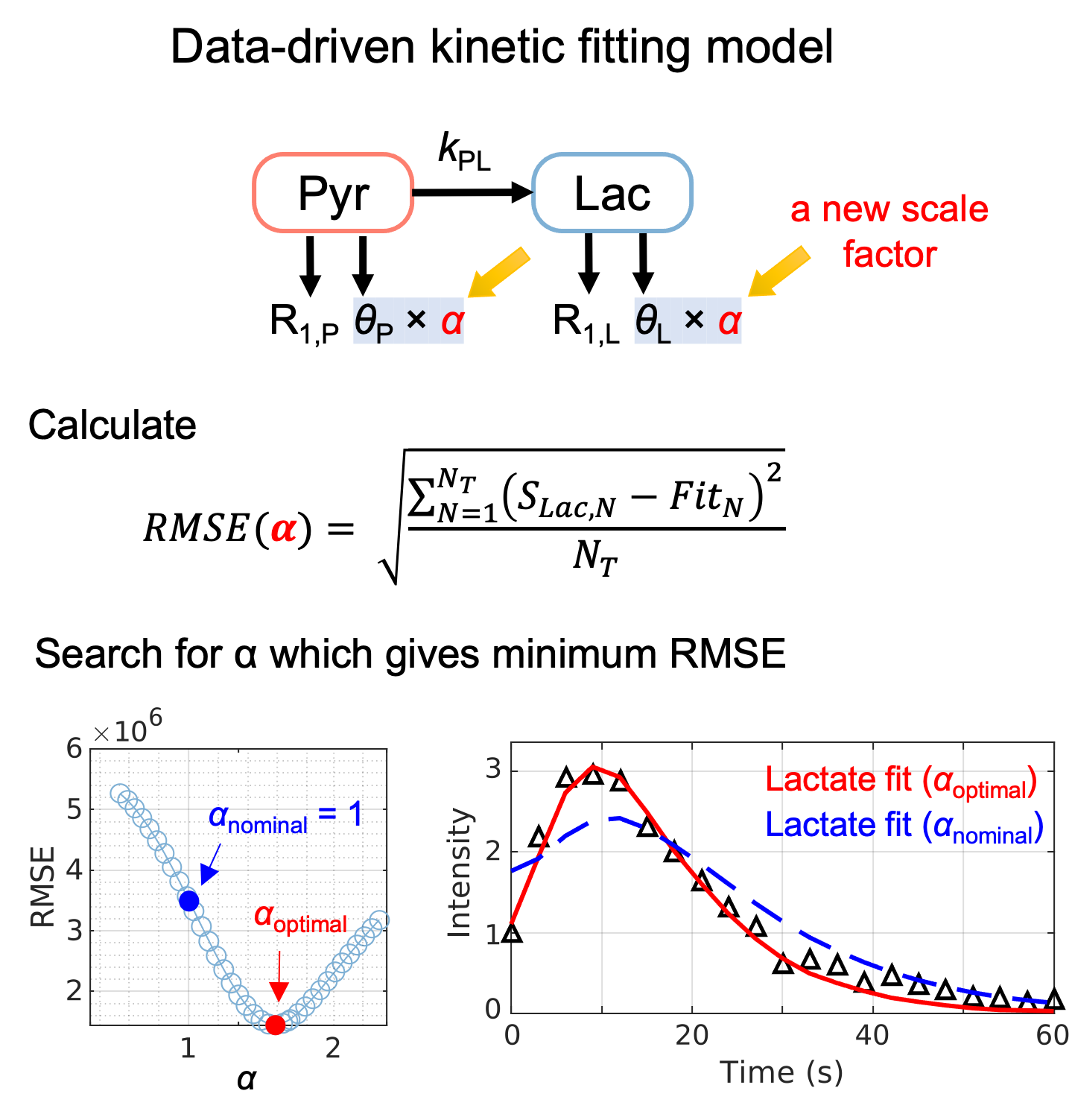
In the proposed method (Fig. 1), the inputless kPL fitting method3 is modified by applying a scale factor, α, to the RF flip angle (θ). Kinetic fitting is performed across a range of α, and the kPL is determined at α = αoptimal corresponding to the minimum root-mean-square error (RMSE) of lactate fit.Numerical simulations were conducted using pyruvate and lactate data simulated with added noise and R1P = 1/30 s-1, R1L = 1/25 s-1, kPL= (0.005, 0.02, and 0.04) s-1, and ground truth pyruvate and lactate flip angles (θP, θL) = (10°, 30°). To model B1 field inhomogeneity and uncertainty in R1L, (θP, θL) and R1L were varied ± 60%. 250 datasets with 20 timepoints with TR = 3 s were generated at each parameter set. In one simulation, additional scaling parameter β was introduced to R1L to evaluate the impact of uncertainties in R1L. kPL was computed for a range of α and β, along with the RMSE of the lactate fit.
HP [1-13C]pyruvate data were acquired from 3 healthy Sprague-Dawley rats using metabolite-specific spiral-GRE (RTHawk, HeartVista)4 and a 1H/13C transceiver birdcage coil on a clinical 3T scanner. HP [1-13C]pyruvate was prepared in a 5T GE SPINlab at 0.8 K. Each rat was imaged twice with 3 HP [1-13C]pyruvate injections. In one session, three different flip angles were used for each acquisition (θP, θL) = (10°, 30°), (15°, 45°), and (20, 60°). In the other, each flip angle scheme was repeated to assess the impact of multiple pyruvate injections on measured kPL.
HP [1-13C]pyruvate data of the human abdomen was also acquired from a patient with nonalcoholic steatohepatitis (NASH) following a similar method described previously5 to assess the feasibility of applying the proposed kinetic fitting method to human data.
Results
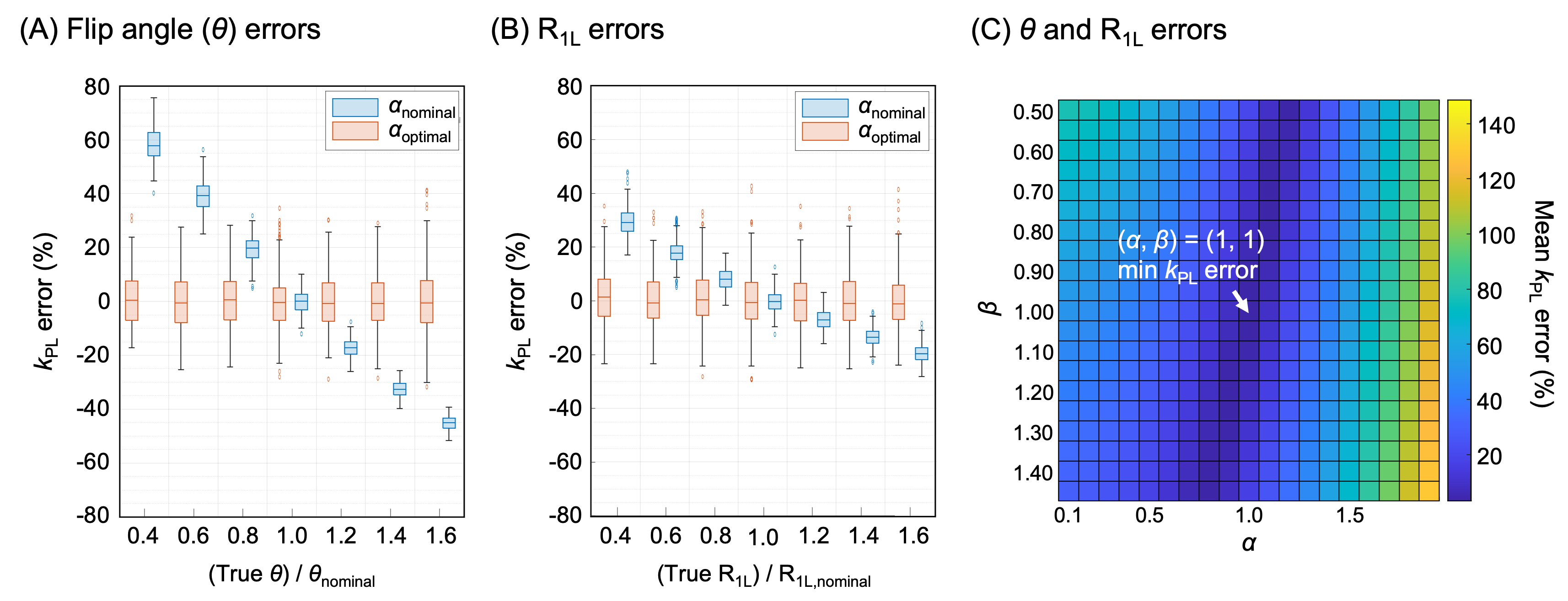
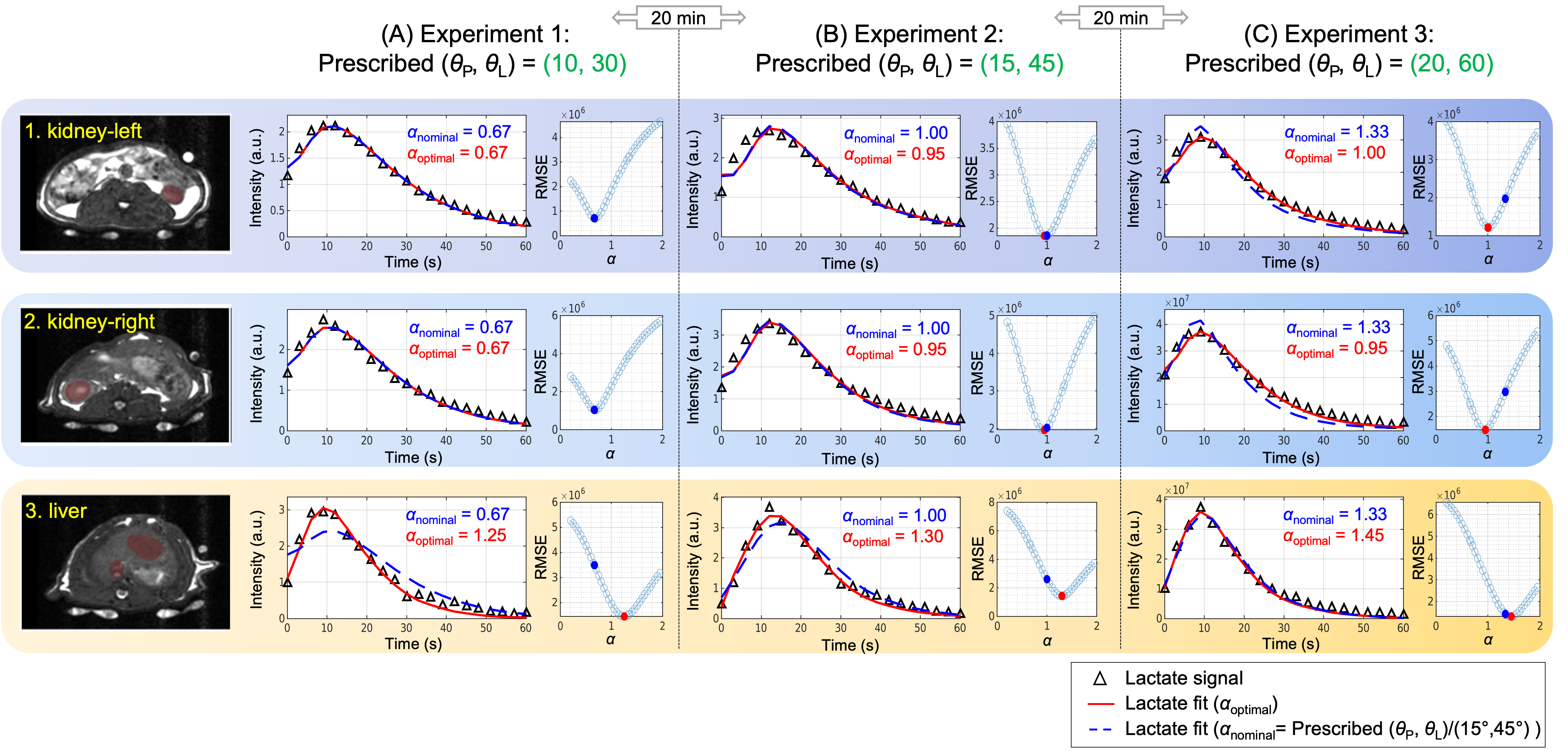
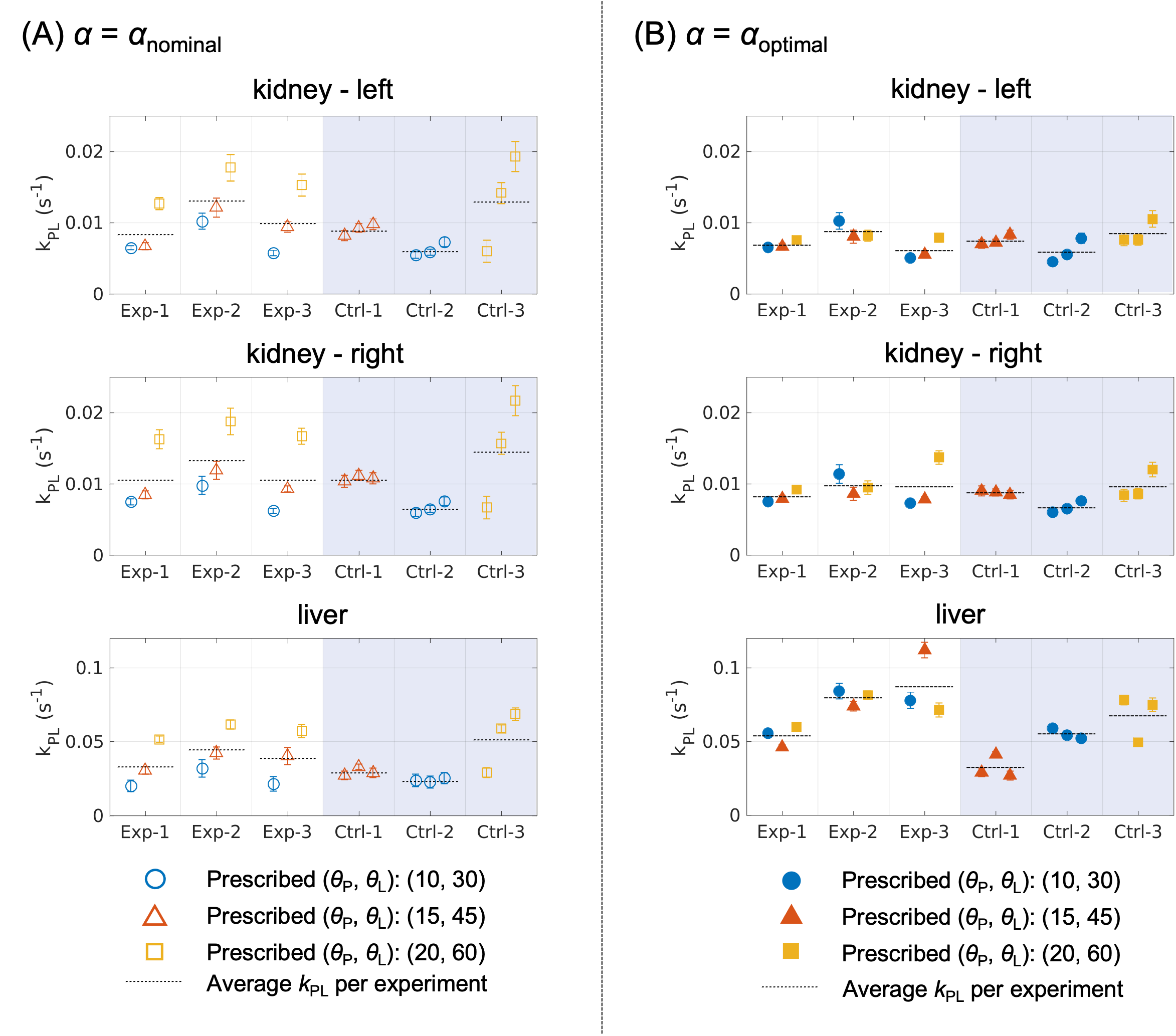
In simulations, the data-driven approach was effective in correcting for flip angle errors and improved the accuracy of kPL determination at the cost of increased variance (Fig. 2A). When the assumed value of R1L was incorrect, αoptimal was affected but the kPL accuracy was maintained (Fig. 2B). When both flip angle and R1L were varied using scale factors (α, β), a 2D map of mean kPL errors showed vertically aligned local minima with α, indicating that the RMSE is more sensitive to the variation in flip angle than R1L (Fig. 2C).The kinetic fitting model was verified in animals using HP 13C acquisitions with different flip angles. Figure 3 represents the kPL results in kidney and liver ROIs from one set of experiments. The lactate fits are improved using αoptimal as supported by lower RMSE compared to using nominal flip angles (αnominal). Interestingly, αoptimal was not necessarily the same as αnominal despite using a volume coil with a homogeneous B1 field. Comparing kPL data between αnominal and αoptimal obtained from 3 experiments and 3 controls (Figure 4A-B), tighter kPL distributions can be observed with αoptimal. Additionally, the repeated pyruvate injections had a minimal effect on the pyruvate metabolism (Fig. 4). The average relative standard deviation of kPL from using αnominal and αoptimal was 43.3 ± 10.9 and 27.3 ± 6.63 %, respectively.
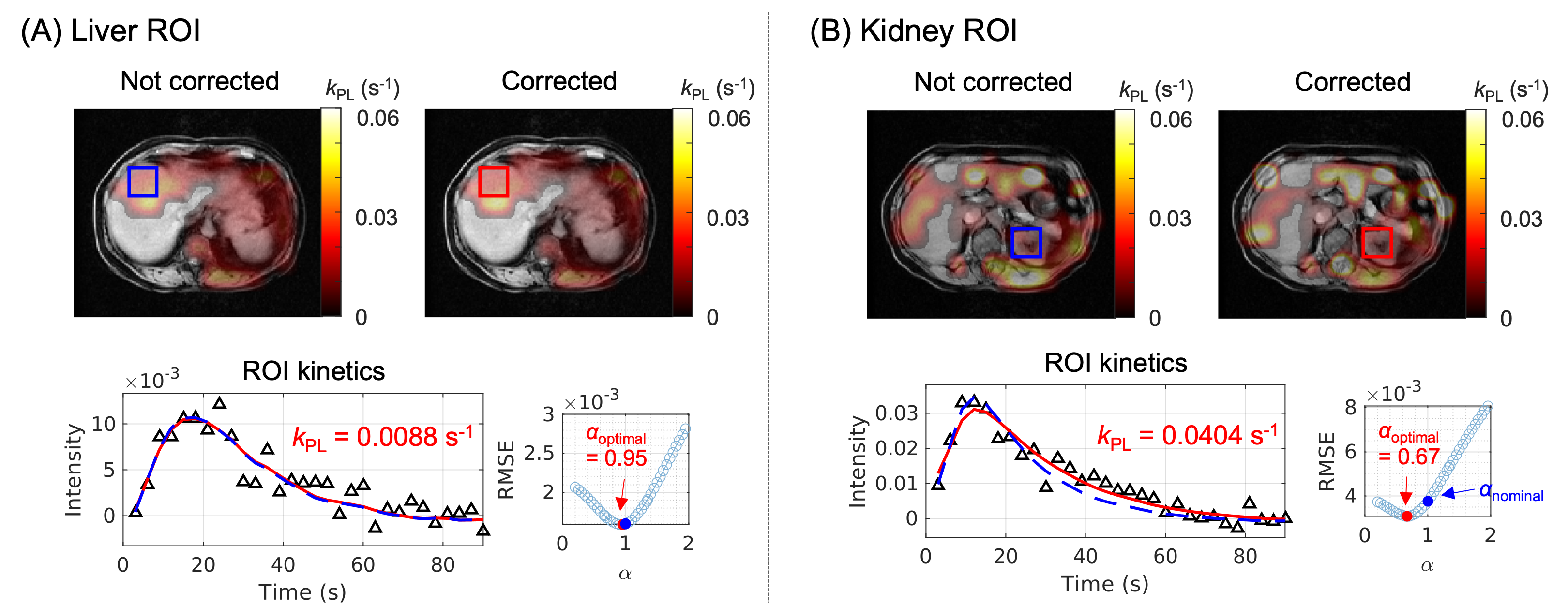
This method was applied to HP-13C pyruvate data from a NASH patient acquired with a flexible vest coil known to have B1 inhomogeneity. Figure 5 displays the kPL maps obtained before and after α correction and the lactate fits from liver and kidney ROIs.
Discussion and Conclusion
This study proposed a data-driven kinetic fitting method for HP 13C-pyruvate MRI and demonstrated improved kinetic modeling accuracy. Via numerical simulations and animal experiments, we showed that this approach could handle errors due to variation in B1 and R1L. The discrepancy in our animal experiments between αoptimal and αnominal, along with the reduced kPL variation when using αoptimal, further implies that this approach can potentially correct for other sources of model mismatch such as variations in bolus characteristics and relaxation rates.Acknowledgements
This work was supported by NIH grants R01CA183071, U01EB026412, R01DK115987, and P41EB013598.References
1. Kurhanewicz J, Vigneron DB, Ardenkjaer-Larsen JH, et al. Hyperpolarized 13C MRI: Path to Clinical Translation in Oncology. Neoplasia. 2019;21(1):1-16. doi:10.1016/j.neo.2018.09.0062.
2. Lee PM, Chen H, Gordon JW, et al. Specialized computational methods for denoising, B1 correction, and kinetic modeling in hyperpolarized 13C MR EPSI studies of liver tumors. Magnetic Resonance in Med. 2021;86(5):2402-2411. doi:10.1002/mrm.289013.
3. Larson PEZ, Chen HY, Gordon JW, et al. Investigation of analysis methods for hyperpolarized 13C-pyruvate metabolic MRI in prostate cancer patients: Hyperpolarized Pyruvate Prostate Cancer Analysis Methods. NMR in Biomedicine. 2018;31(11):e3997. doi:10.1002/nbm.39975.
4. Liu X, Tang S, Mu C, et al. Development of specialized magnetic resonance acquisition techniques for human hyperpolarized [13C, 15N2]urea + [1‐13C]pyruvate simultaneous perfusion and metabolic imaging. Magnetic Resonance in Med. 2022;88(3):1039-1054. doi:10.1002/mrm.29266
5. Lee PM, Chen H, Gordon JW, et al. Whole‐Abdomen Metabolic Imaging of Healthy Volunteers Using Hyperpolarized [1‐13C]pyruvate MRI. Magnetic Resonance Imaging. April 2022:jmri.28196. doi:10.1002/jmri.281964.
Figures