3060
Brain consciousness affects HP lactate labeling from HP pyruvate1Laboratory of Functional and Metabolic Imaging, École polytechnique fédérale de Lausanne (EPFL), Lausanne, Switzerland, 2Department of Health Technology, Center for Hyperpolarization in Magnetic Resonance, Technical University of Denmark, Kgs Lyngby, Denmark
Synopsis
Keywords: Hyperpolarized MR (Non-Gas), Brain, Anesthesia, anaesthesia, cerebral, mouse, pyruvate, lactate, hyperpolarized, hyperpolarization, DNP, metabolism, metabolic
Motivation: Brain metabolism and activity are closely related. General anesthesia, commonly used in preclinical studies, alters functional connectivity, hemodynamics and metabolism. In preclinical MR, metabolic studies frequently employ isoflurane, while a medetomidine-isoflurane combination is preferred for fMRI. Detection of HP substrate conversions is the sole MR technology capable to capture real-time metabolism.
Goal(s): Towards rodent fMRSI studies, we aim to compare the cerebral metabolism of HP [1-13C] pyruvate between mice under isoflurane-only and combined medetomidine-isoflurane anesthesia.
Approach: Dynamic MRSI at high spatiotemporal resolution characterized HP pyruvate metabolism.
Results: Pyruvate-to-lactate turnover is lower and delayed under medetomidine-isoflurane compared to isoflurane-only anesthesia.
Impact: Anesthesia can modulate brain consciousness. Significantly higher hyperpolarized pyruvate-to-lactate turnover is observed in mice under isoflurane-only compared to medetomidine-isoflurane anesthesia. Beyond this finding’s relevance for preclinical studies, this opens opportunities for probing brain biochemistry in patients under general anesthesia.
Introduction
Brain consciousness and cerebral metabolism tightly relate to each other. Most preclinical studies are performed using general anesthetic agents, which are known to alter brain function, hemodynamics and metabolism. Isoflurane is among the most common anesthetic agents used in preclinical MRS studies, while combined medetomidine-isoflurane anesthesia, maintaining higher functional connectivity1, is preferred for fMRI measurements.The above anesthetics have been sparsely compared at the metabolic level. Recent work2 highlighted differences in endogenous lactate levels with 1H-MRS, as well as glucose metabolism via non-hyperpolarized 2H-MRS and hyperpolarized (HP) 13C-MRS in mice between both anesthetic conditions.
Pyruvate is the most available probe for interrogating metabolism via HP MR, can be produced via several approaches3, is at an important crossroad of metabolic pathways4, and is the first probe translated into clinical studies5. Anesthetic conditions are known to have a profound effect on HP pyruvate metabolism6–8.
In the perspective of fMRSI studies in small rodents, the present study aims at comparing the cerebral metabolism of HP [1-13C] pyruvate between isoflurane-only and combined medetomidine-isoflurane anesthetic conditions.
Methods
Measurements were performed on a 14.1T MRI scanner (Bruker) with a mouse head 1H/13C volume coil and a 2-loop 13C receive-only surface coil9, except for two mice using a 18mm 1H/13C volume coil.[1-13C]pyruvic acid with 15mM OX063 was hyperpolarized at 5T/1.2K, yielding 33.3±1.6% liquid-state polarization10.
HP pyruvate cerebral metabolism was assessed in two groups of C57BL6/J mice (26.8±2.5g body weight). Mice were anesthetized with 2% isoflurane in 60% oxygen during femoral vein surgery. Then, in the ISO group (n=4), mice remained under 1.5-2.5% isoflurane-only anesthesia. In the MED-ISO group (n=4), anesthesia was switched to a combination of medetomidine (0.3mg/kg bolus, 0.03mg/kg/h subcutaneous) and 0.25% isoflurane.
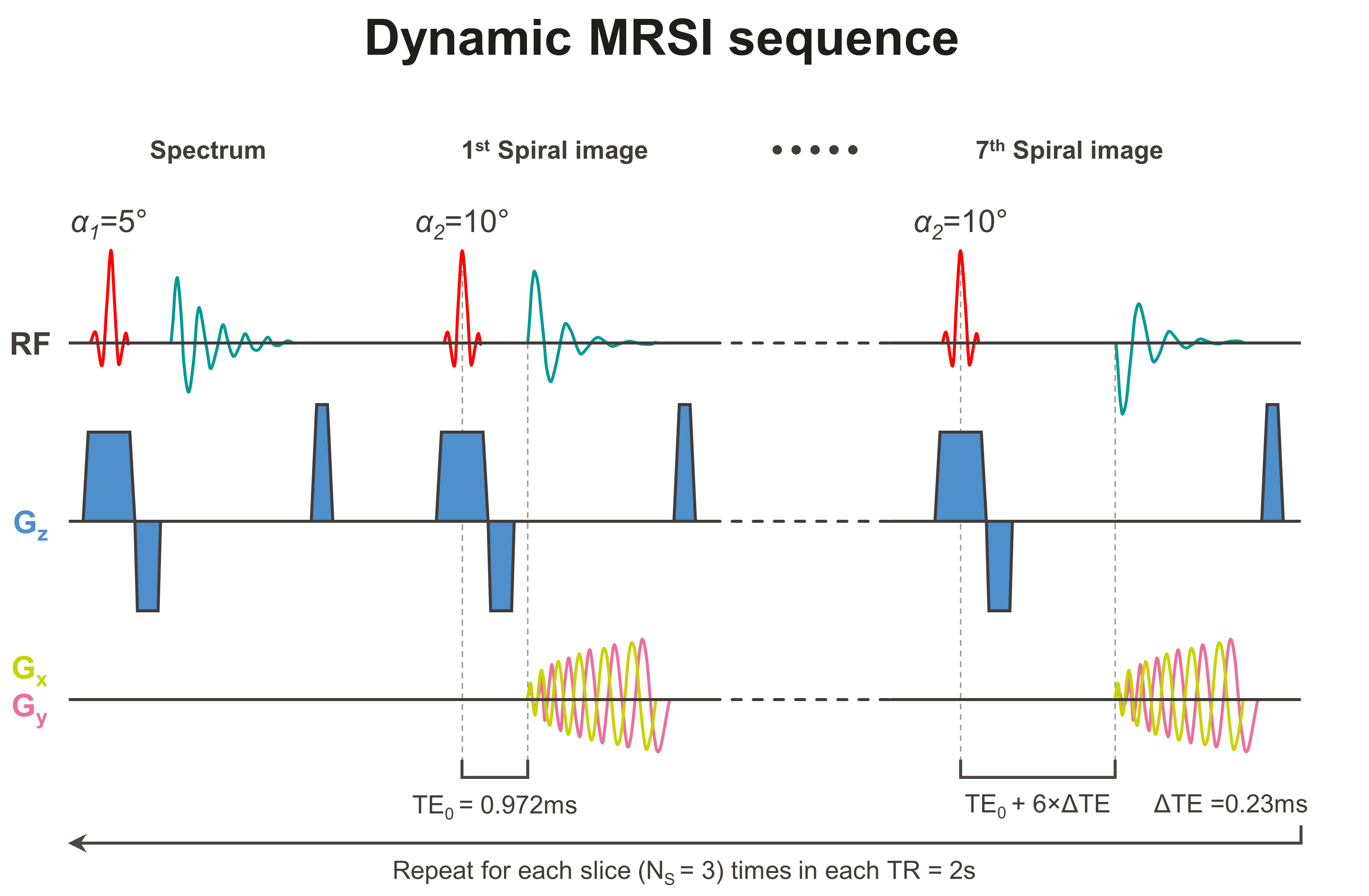
At 80min post-surgery, the sample was dissolved and automatically11 intravenously injected (325µl bolus, 38.2±3.4mM, 0.40±0.07µmol/g dose). Immediately, dynamic 13C MRSI was acquired (TR=2s, three 4mm axial slices, 1mm in-plane resolution) using an IDEAL Spiral CSI12 scheme9 (Fig.1).
Results
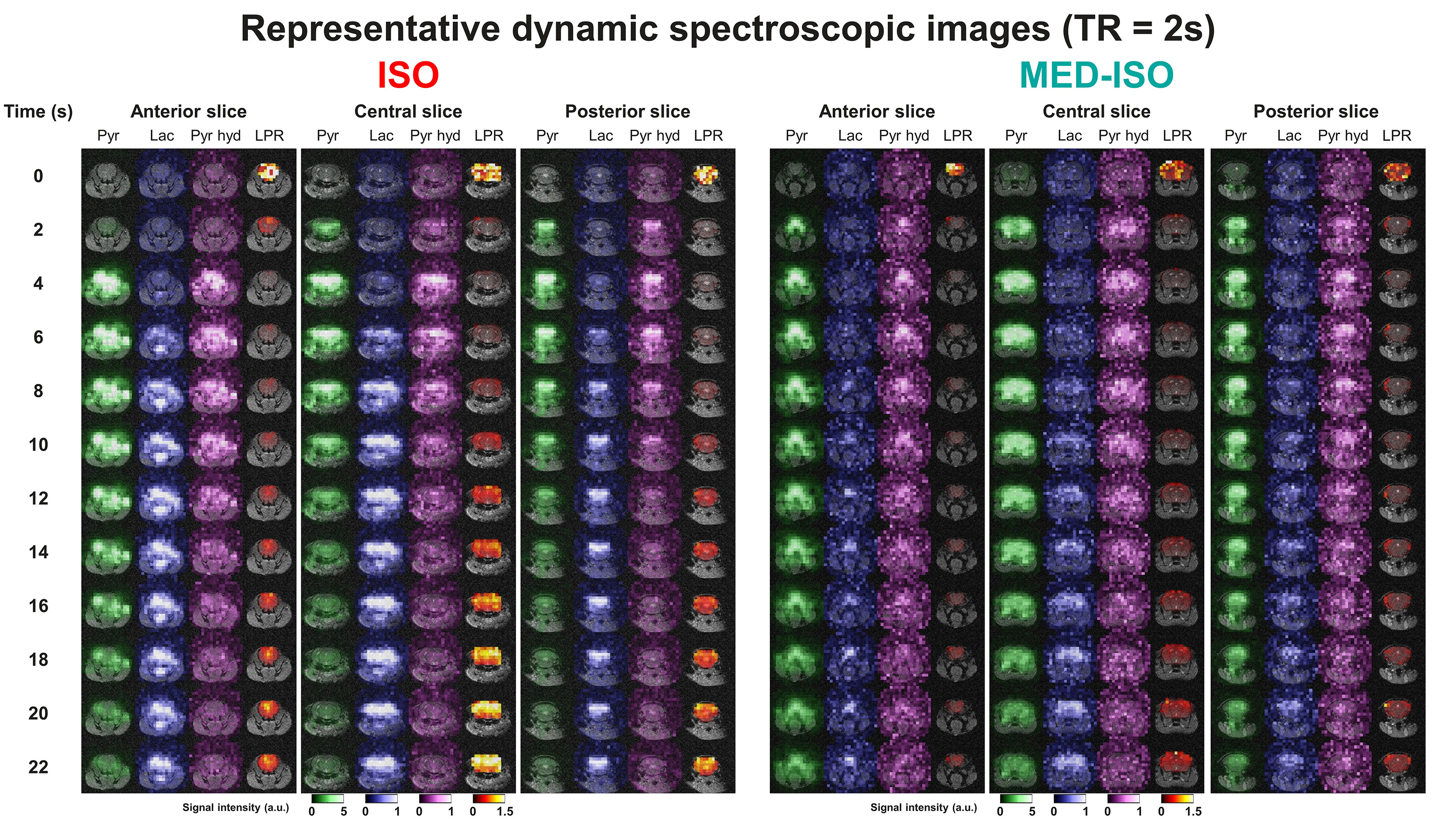
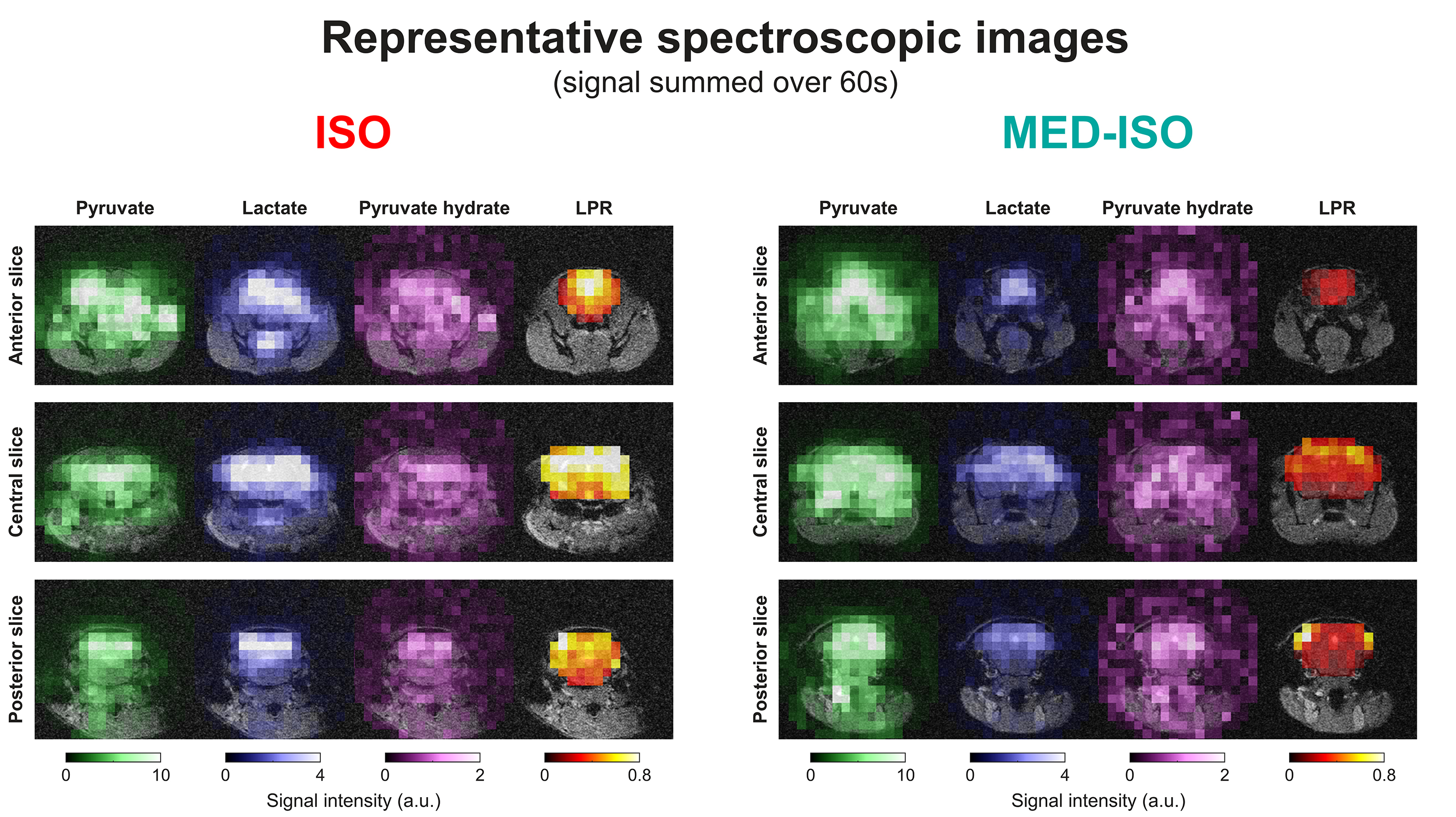
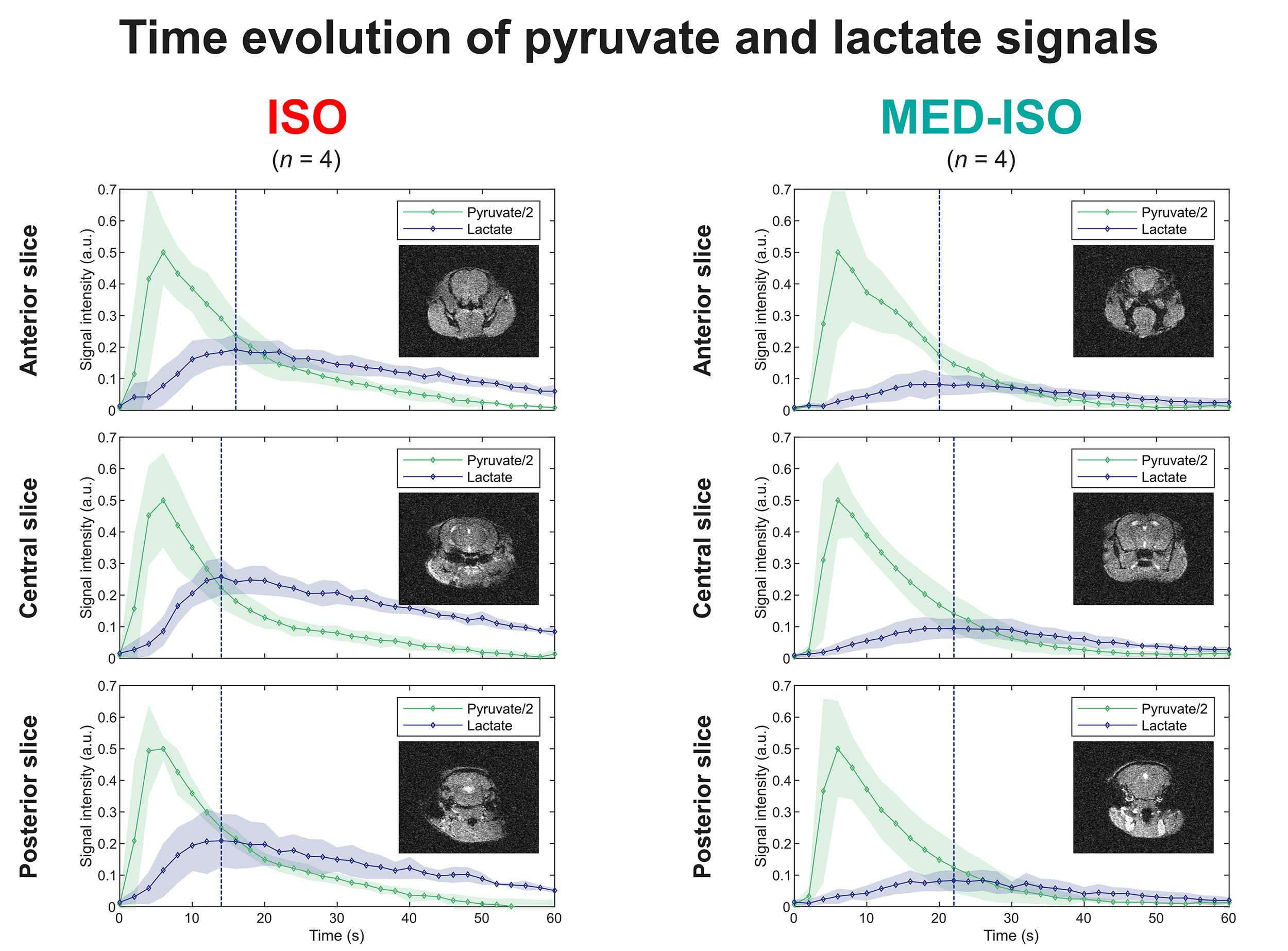
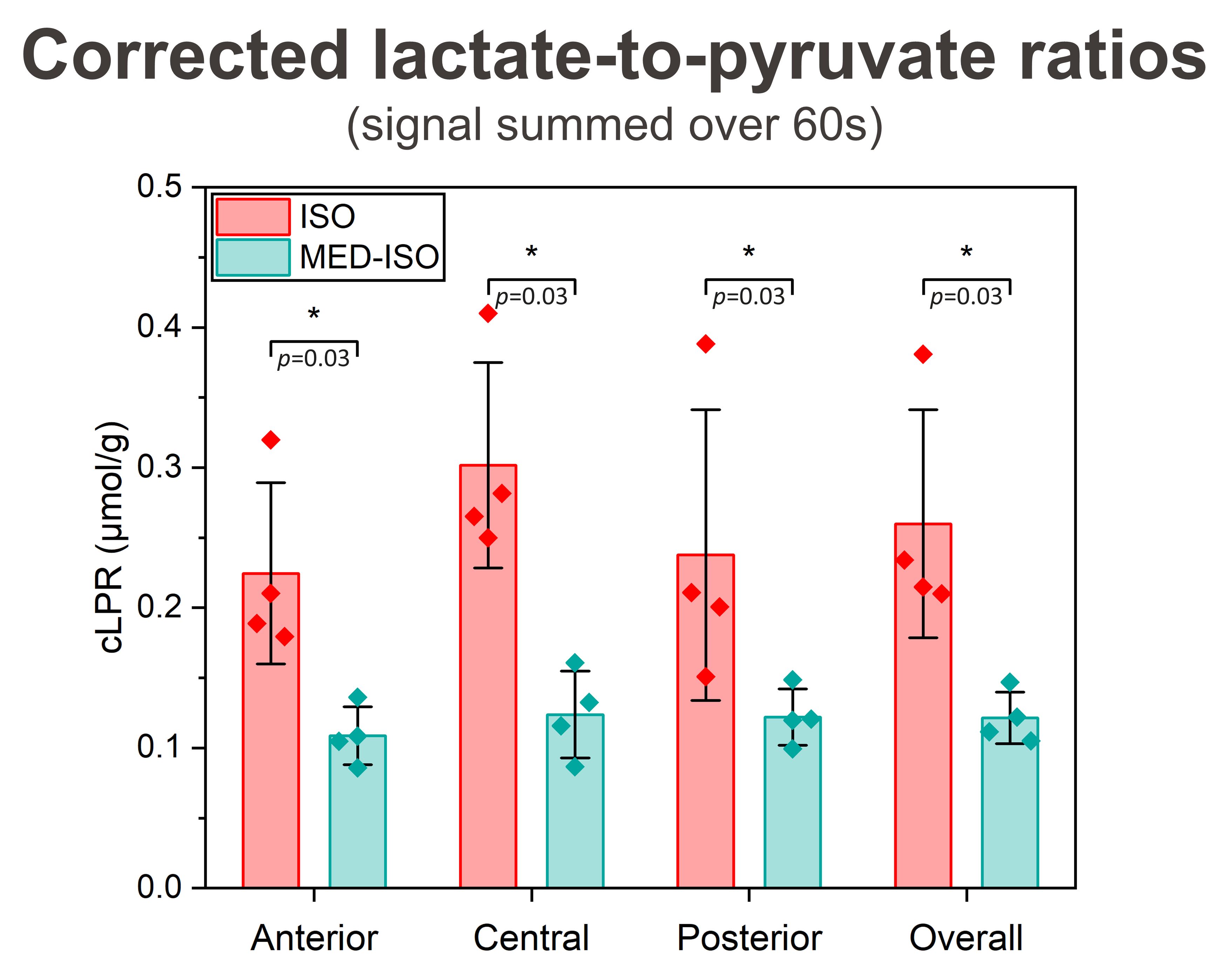
Dynamic MRSI in representative mice depict the influx of pyruvate (-hydrate) and lactate labeling in the brain and surrounding tissues (Fig.2). Across the brain, the lactate signal and lactate-to-pyruvate ratio (LPR) build up faster and higher under ISO than MED-ISO anesthesia (Figs.2-3).Pyruvate and lactate signal time courses within each brain slice were averaged across multiple experiments (Fig.4). The lactate signal is lower and builds up slower under MED-ISO than ISO anesthesia, with a 50% longer time-to-peak. Pyruvate signal dynamics are similar under both conditions.
The corrected lactate-to-pyruvate ratios (cLPR), measured within 60s post-infusion and normalized to the pyruvate dose to account for body weight and infusate concentration variations13, were significantly smaller by half under MED-ISO than ISO anesthesia.
Discussion
This study compared the HP lactate production from a HP pyruvate bolus in the mouse brain between ISO and MED-ISO anesthetic conditions. A delayed (50% longer time-to-peak) and significantly lower (-53%) lactate labeling was observed under MED-ISO compared to ISO anesthesia.This different metabolic outcome likely results from anesthesia-altered transport and/or enzymatic activity. Otherwise, if only physiology was being affected, one would expect higher LPR with MED-ISO. Indeed, the pyruvate signal predominantly originates from the blood volume14, since transport across the blood-brain-barrier15 is slower than lactate dehydrogenase (LDH) conversion, even with high enzymatic activity16. Isoflurane being a dose-dependent cerebral vasodilator17, the lower isoflurane under MED-ISO conditions would reduce pyruvate signal and increase LPR.
The dissimilar signal time evolution suggests that pyruvate uptake is substantially different between both groups. Further investigations are necessary to sustain this hypothesis and understand the distinct metabolic response.
The different lactate labeling observed here is coherent with previous studies2 reporting the absence of 2H-lactate produced from non-hyperpolarized 2H-glucose and the smaller endogenous lactate pool size observed in 1H MRS, under MED-ISO compared to ISO anesthesia.
Interestingly, an opposite trend was previously observed with HP 13C-glucose2, from which the lactate labeling is two-fold higher under MED-ISO than ISO anesthesia. This highlights that despite the identical metabolic outcome, anesthesia affects differently the steps involved in lactate production from pyruvate (2 steps: transport and LDH exchange) than glucose (12 steps: transport, 10 steps of glycolysis, and LDH exchange). Thus, these probes are complementary and can interrogate distinct aspects of tissue biochemistry.
Conclusion
Distinct brain consciousness and metabolic conditions can be modeled by anesthesia. A distinct conversion of HP pyruvate into lactate, both in terms of dynamics and turnover, was measured between mice under isoflurane and combined medetomidine-isoflurane anesthesia. This finding brings relevant information, not only regarding preclinical HP MRS and fMRSI, but also towards the measurement of neurochemistry in clinical cases with patients requiring general anesthesia.Acknowledgements
This work was generously supported by the Swiss National Science Foundation (193276 assigned to Andrea Capozzi, 214069 assigned to Mor Mishkovsky). The authors would like to thank Prof. Rolf Gruetter for fruitful discussions, as well as Estelle Gerossier and Dr. med. vet. Stefan Mitrea for their assistance in the animal preparation, as well as the CIBM Center for Biomedical Imaging, co-founded and supported by Lausanne University Hospital, University of Lausanne, École polytechnique fédérale de Lausanne, University of Geneva and Geneva University Hospitals.References
1. Hemmings HC, Riegelhaupt PM, Kelz MB, et al. Towards a Comprehensive Understanding of Anesthetic Mechanisms of Action: A Decade of Discovery. Trends Pharmacol Sci. 2019;40(7):464-481. doi:10.1016/j.tips.2019.05.001
2. Flatt E, Lanz B, Pilloud Y, et al. Measuring Glycolytic Activity with Hyperpolarized [13H7, U-13C6] D-Glucose in the Naive Mouse Brain under Different Anesthetic Conditions. Metabolites. 2021;11(7):413. doi:10.3390/metabo11070413
3. Nagel L, Gierse M, Gottwald W, et al. Parahydrogen-Polarized [1-13C]Pyruvate for Reliable and Fast Preclinical Metabolic Magnetic Resonance Imaging. Adv Sci. 2023:2303441. doi:10.1002/advs.202303441
4. Kurhanewicz J, Vigneron DB, Ardenkjaer-Larsen JH, et al. Hyperpolarized 13C MRI: Path to Clinical Translation in Oncology. Neoplasia. 2019;21(1):1-16. doi:10.1016/j.neo.2018.09.006
5. Nelson SJ, Kurhanewicz J, Vigneron DB, et al. Metabolic Imaging of Patients with Prostate Cancer Using Hyperpolarized [1-13C]Pyruvate. Sci Transl Med. 2013;5(198):198ra108-198ra108. doi:10.1126/scitranslmed.3006070
6. Josan S, Hurd R, Billingsley K, et al. Effects of isoflurane anesthesia on hyperpolarized 13C metabolic measurements in rat brain. Magn Reson Med. 2013;70(4):1117-1124. doi:10.1002/mrm.24532
7. Hyppönen V, Stenroos P, Nivajärvi R, et al. Metabolism of hyperpolarised [1–13C]pyruvate in awake and anaesthetised rat brains. NMR Biomed. 2022;35(2):e4635. doi:10.1002/nbm.4635
8. Marjańska M, Shestov AA, Deelchand DK, Kittelson E, Henry PG. Brain metabolism under different anesthetic conditions using hyperpolarized [1-13C]pyruvate and [2-13C]pyruvate. NMR Biomed. 2018;31(12):e4012. doi:10.1002/nbm.4012
9. Lê TP, Buscemi L, Lepore M, et al. Development and application of dynamic MRSI of an HP neuroprotective agent in an MCAO mouse model of ischemic stroke at 14.1T. In: Proc. ISMRM. ; 2023:3920. https://cds.ismrm.org/protected/23MPresentations/abstracts/3920.html
10. Lê TP, Hyacinthe JN, Capozzi A. How to improve the efficiency of a traditional dissolution dynamic nuclear polarization (dDNP) apparatus: Design and performance of a fluid path compatible dDNP/LOD-ESR probe. J Magn Reson. 2022;338:107197. doi:10.1016/j.jmr.2022.107197
11. Comment A, van den Brandt B, Uffmann K, et al. Design and performance of a DNP prepolarizer coupled to a rodent MRI scanner. Concepts Magn Reson Part B Magn Reson Eng. 2007;31B(4):255-269. doi:10.1002/cmr.b.20099
12. Wiesinger F, Weidl E, Menzel MI, et al. IDEAL spiral CSI for dynamic metabolic MR imaging of hyperpolarized [1-13C]pyruvate. Magn Reson Med. 2012;68(1):8-16. doi:10.1002/mrm.23212
13. Hyacinthe JN, Buscemi L, Lê TP, Lepore M, Hirt L, Mishkovsky M. Evaluating the potential of hyperpolarised [1-13C] L-lactate as a neuroprotectant metabolic biosensor for stroke. Sci Rep. 2020;10(1):5507. doi:10.1038/s41598-020-62319-x
14. Hurd RE, Yen YF, Tropp J, Pfefferbaum A, Spielman DM, Mayer D.
Cerebral Dynamics and Metabolism of Hyperpolarized [1-13C]pyruvate Using
Time-Resolved MR Spectroscopic Imaging. J Cereb Blood Flow Metab.
2010;30(10):1734-1741. doi:10.1038/jcbfm.2010.93
15. Miller JJ, Grist JT, Serres S, et al. 13C Pyruvate Transport Across the Blood-Brain Barrier in Preclinical Hyperpolarised MRI. Sci Rep. 2018;8(1):15082. doi:10.1038/s41598-018-33363-5
16. Rao Y, Gammon S, Zacharias NM, et al. Hyperpolarized [1-13C]pyruvate-to-[1-13C]lactate conversion is rate-limited by monocarboxylate transporter-1 in the plasma membrane. Proc Natl Acad Sci. 2020;117(36):22378-22389. doi:10.1073/pnas.2003537117
17. Todd MM, Weeks J. Comparative Effects of Propofol, Pentobarbital, and Isoflurane on Cerebral Blood Flow and Blood Volume. J Neurosurg Anesthesiol. 1996;8(4):296.
Figures