3042
Development and optimization of deuterium metabolic imaging in the human abdomen at 3T1Radiology, University of Cambridge, Cambridge, United Kingdom, 2Urology, Cambridge University Hospitals NHS Trust, Cambridge, United Kingdom, 3Surgery, University of Cambridge, Cambridge, United Kingdom
Synopsis
Keywords: Deuterium, Deuterium
Motivation: Abdominal imaging of orally-administered deuterium-labelled tracers can be hindered by artifacts arising from excessive stomach signal.
Goal(s): To establish and optimize methods for acquisition of abdominal deuterium metabolic imaging in conjunction with orally-administered tracers.
Approach: A flexible transmit-receive surface coil was used to image naturally abundant deuterium in healthy volunteers and orally-administered D2O in a patient with renal cancer.
Results: Water and lipid peaks were repeatably fit with high confidence both in unlocalised spectra and voxels extracted from MRSI in the liver, kidney, and spleen. Artifacts were minimal even 12 minutes after tracer ingestion.
Impact: Feasibility of abdominal deuterium imaging at 3T was demonstrated using a flexible surface coil. We obtained consistent water measurements in healthy volunteers and good images in a patient with a left-sided renal tumour even just 12 min after drinking D2O.
Introduction
Few deuterium imaging studies have been undertaken in the human abdomen1-3, and none at clinical field strength. We have recently demonstrated deuterium imaging at 3T in the brain4. When volume transmit coils are used, oral tracer studies can be overwhelmed by the signal arising from the stomach, especially at early time points2. Here we report the use of a surface transmit-receive coil to minimize stomach signal, while enabling coverage of other abdominal organs at 3T. Posterior and lateral coil positions are compared, and we demonstrate the proof of principle in a patient with a renal tumour following oral administration of D2O.Methods
Ten subjects (9 young healthy volunteers; 1 patient with a left-sided 5.2cm renal oncocytoma) were recruited to ethically approved clinical studies (REC: 23/YH/0127; NCT06016075). They were positioned supine in a 3T Premier MRI scanner (GE Waukesha WI, USA). A flexible 20x30cm surface coil for deuterium (RAPID, Rimpar, Germany) was either placed underneath the subjects to target both kidneys (n=5 healthy volunteers and 1 patient) or wrapped around the right side of the abdomen, secured with velcro straps, to target the liver and right kidney (n=4). An axial T1W dual gradient-echo fat/water (LAVA-flex) series was acquired in a single breath-hold using the body coil (flip 12°, TE = 1.1/2.2ms, TR=4.0ms, FOV 48cm, matrix 300x200, 64 x 5mm thick slices, 1 NEX, BW 167 kHz). Unlocalized spectra were collected from the whole sensitive volume of the coil (TE=0.7ms, TR=600ms, flip=90°, 64 averages), followed by Hamming-filtered density-weighted MRSI (10x10x10 resolution, 1678 transients, FOV 40cm, flip 60°, TE 0.7ms, TR 250ms). A matching MRSI with flip 30° was acquired in 4 subjects for generation of a double-angle method B1 map5. Unlocalized spectra were repeated within-session in 2 subjects, and between-sessions about 10 days apart in 2 subjects. The patient drank the D2O solution (190g of water for injection + 11.1g of D2O) immediately before the scan, with the last meal 2h prior.MRSI data were zero-filled once in each spatial domain prior to automated peak fitting of water and lipids using AMARES in a locally customised version of OXSA6. Amplitude ratios of water/(water+lipids) were compared in unlocalized spectra and between voxels selected from liver, kidneys, spleen, and (in the patient) tumour and stomach. Overlays on anatomic images were created using ITK-SNAP 3.8.
Results
Reasonable fits to unlocalized spectra were obtained in all cases (Fig. 1; Cramer-Rao Bounds (CRB) for water ranged from 0.9 – 3.2%, mean 1.7%). The CRB for lipids was always higher than water, especially when the coil was placed laterally rather than posterior (mean CRB 19% lateral vs 5% posterior, p<0.02). The water fraction tended to be higher in the lateral position, but not significantly (0.86 ± 0.13 vs 0.75 ± 0.07). The standard deviation of repeated measures of water fraction within the same session was small (0.008), but variation between sessions was higher (0.03 - 0.06), which may be secondary to inconsistencies in coil placement. Coil penetration can be measured from the B1 maps to be around 12cm, while nulls were often seen in the subcutaneous fat close to the coil surface.Acceptable fits were also obtained to spectra extracted from MRSI voxels in the liver, kidneys, and spleen when those were within the sensitive volume of the coil. Ratios of water/(water+lipid) were consistent within and between organs and volunteers (Fig. 2).
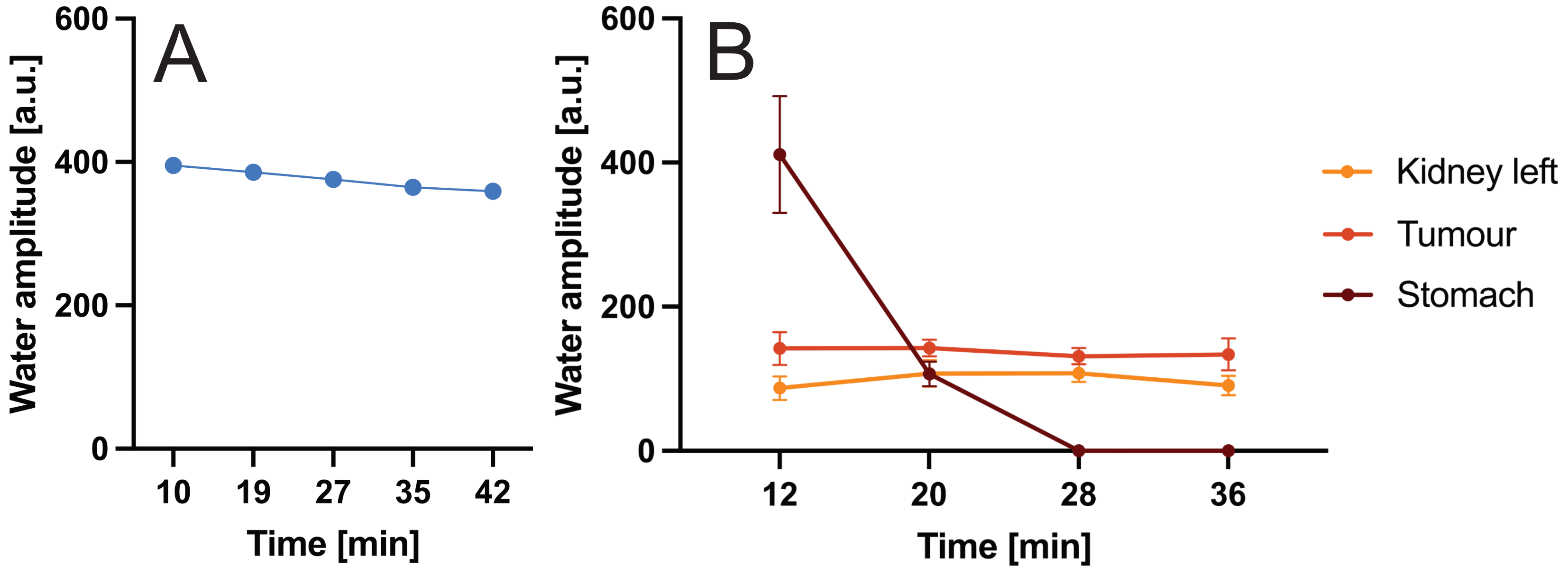
After ingestion of D2O, strong water signal was detected from the stomach despite the depth (13-25 cm) exceeding the expected coil penetration (Fig. 3). However, although this was stronger than signal in other organs at the initial time points, the distance from the coil limited the dynamic range difference and thus prevented severe point spread function artifacts, and it disappeared within 30 minutes. Water signal in the tumour and contralateral kidney remained stable over the timecourse, while overall unlocalized water signal declined slowly over 40 min (Fig. 4).
Discussion
Imaging of naturally abundant deuterium has been demonstrated in the human abdomen at 3T. Water and lipid peaks were repeatably fit with high confidence both from the unlocalised spectra and voxels extracted from MRSI in the liver, kidney and spleen. Small variation in the water/(water+lipid) ratio was observed within and between organs and volunteers. The coil used was shown to avoid excessive artifact from stomach signals even within 12 minutes of oral administration of a high dose of D2O. D2O itself may be of interest in cancer monitoring7, but also the current work establishes a baseline for studies using oral deuterated glucose at 3T in cancer and other diseases.Acknowledgements
This research was supported by Cancer Research UK (EDDPMA-May22\100068), the Cancer Research UK Cambridge Centre, the NIHR Cambridge Biomedical Research Centre (BRC-1215-20014), and the Marmaduke-Sheild Fund. MM acknowledges support from the Cambridge Experimental Cancer Medicine Centre, PW from the Gates Cambridge Trust (#OPP1144), JB from the National Cancer Imaging Translational Accelerator (NCITA).
References
1. De Feyter HM, Behar KL, Corbin ZA, Fulbright RK, Brown PB, McIntyre S, Nixon TW, Rothman DL, de Graaf RA. Deuterium metabolic imaging (DMI) for MRI-based 3D mapping of metabolism in vivo. Sci Adv 2018; 4(8):eaat7314.
2. Gursan A, Hendriks A, Welting D, de Jong P, Klomp D, Prompers J. Deuterium body array for simultaneous measurement of hepatic and renal glucose metabolism and gastric emptying with dynamic 3D deuterium metabolic imaging at 7T. NMR Biomed 2023;
3. Nam KM, Gursan A, Bhogal AA, Wijnen JP, Klomp DWJ, Prompers JJ, Hendriks AD. Deuterium echo-planar spectroscopic imaging (EPSI) in the human liver at 7T. Magn Reson Med 2023; 90:863-874.
4. Kaggie JD, Khan AS, Matys T, Schulte RF, Locke MJ, Grimmer A, Frary A, Graves MJ, McLean MA, Gallagher FA. Deuterium metabolic imaging and hyperpolarized 13C-MRI of the normal human brain at clinical field strength reveals differential cerebral metabolism. Neuroimage 2022 Aug 15;257:119284.
5. Wang J, Qiu M, Yang QX, Smith MB, Constable RT. Measurement and correction of transmitter and receiver induced nonuniformities in vivo. Magn. Reson. Med. 2005; 53:408-417.
6. Purvis, L.A., Clarke, W.T., Biasiolli, L., Valkovič, L., Robson, M.D., Rodgers, C.T., 2017. OXSA: An open-source magnetic resonance spectroscopy analysis toolbox in MATLAB. PloS one 12, e0185356.
7. Asano H, Elhelaly AE, Hyodo F, Iwasaki R, Noda Y, Kato H, Ichihashi K, Tomita H, Murata M, Mori T, Matsuo M. Deuterium magnetic resonance imaging using deuterated water-induced 2H-tissue labeling allows monitoring cancer treatment at clinical field strength.
Figures
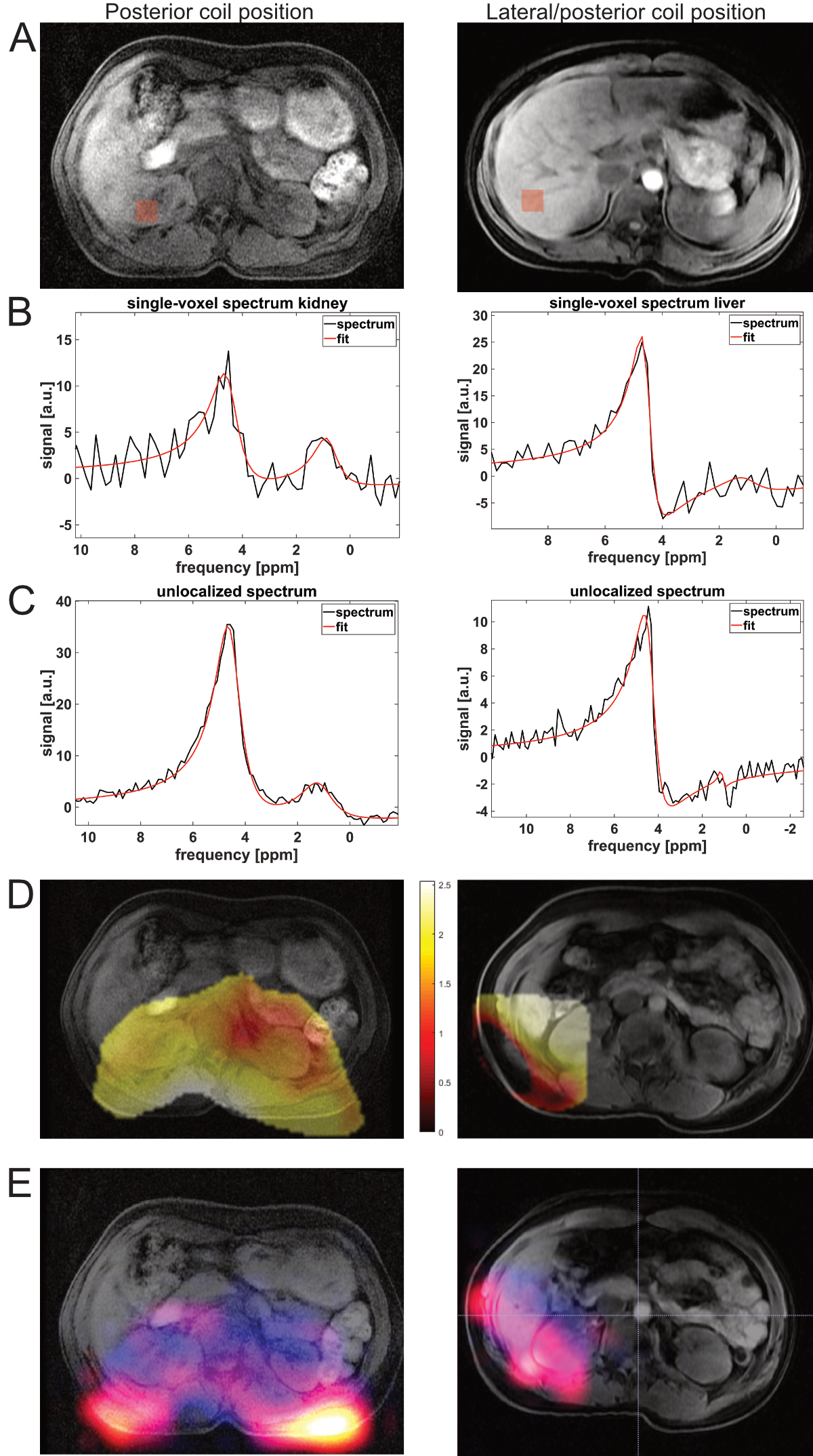
Figure 1: Comparison of data acquired with deuterium coil placed under the lower back (left column) or wrapped around the right side (right column). (A) T1W image showing in red the approximate voxel location extracted from MRSI in (B), which includes the spectral fit in OXSA. (C) OXSA fit to unlocalized MRS. (D) Map of relative B1 (actual/nominal flip) from the slice at the centre of coil. (E) Color overlay showing both lipids (“hot” colorscale) and water in blue.
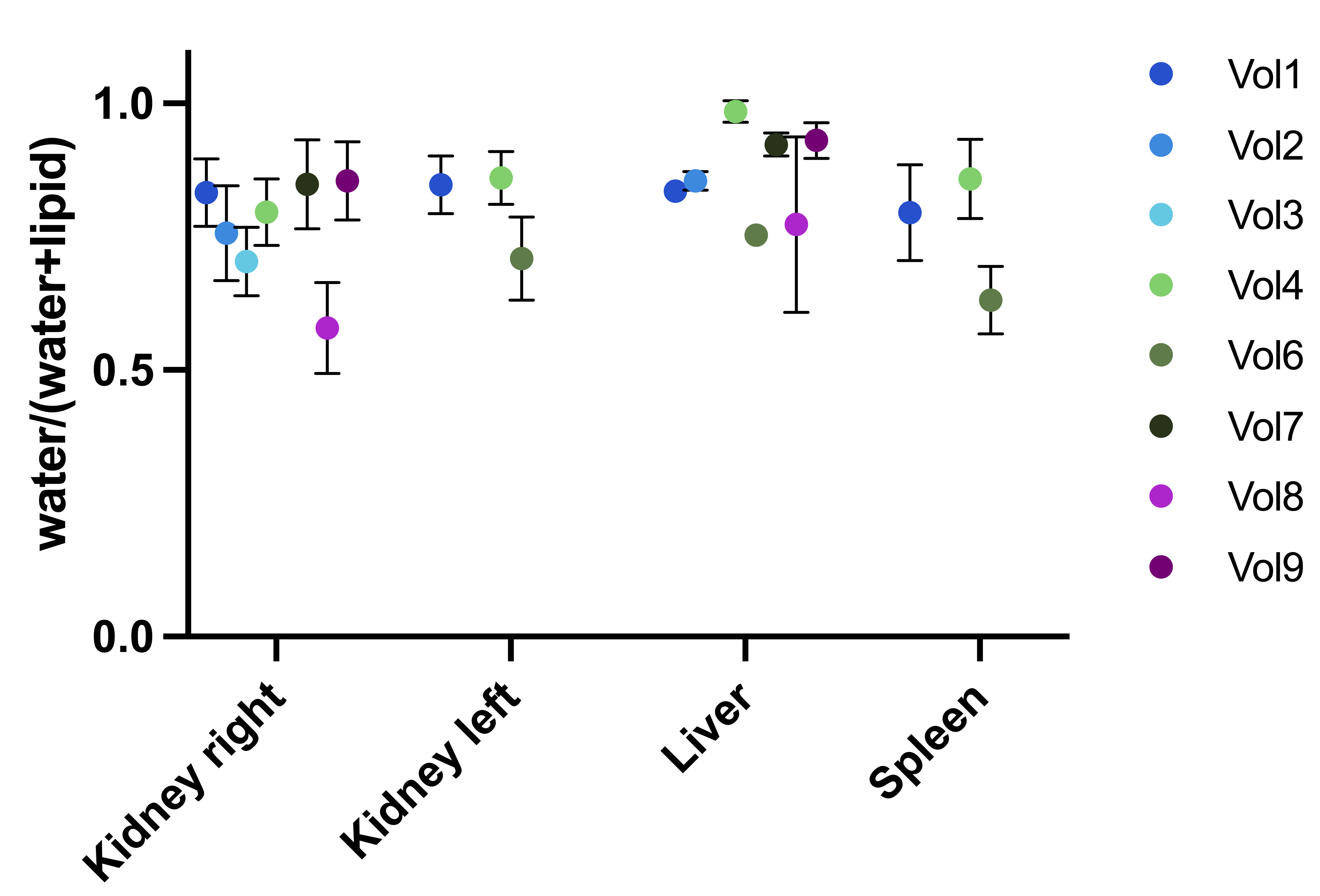
Figure 2: The ratio of water to (water+lipid) peaks from spectral fitting in OXSA. For each organ, the mean and SD of measurements from all voxels within the organ are shown where the CRB of any peak was <10.
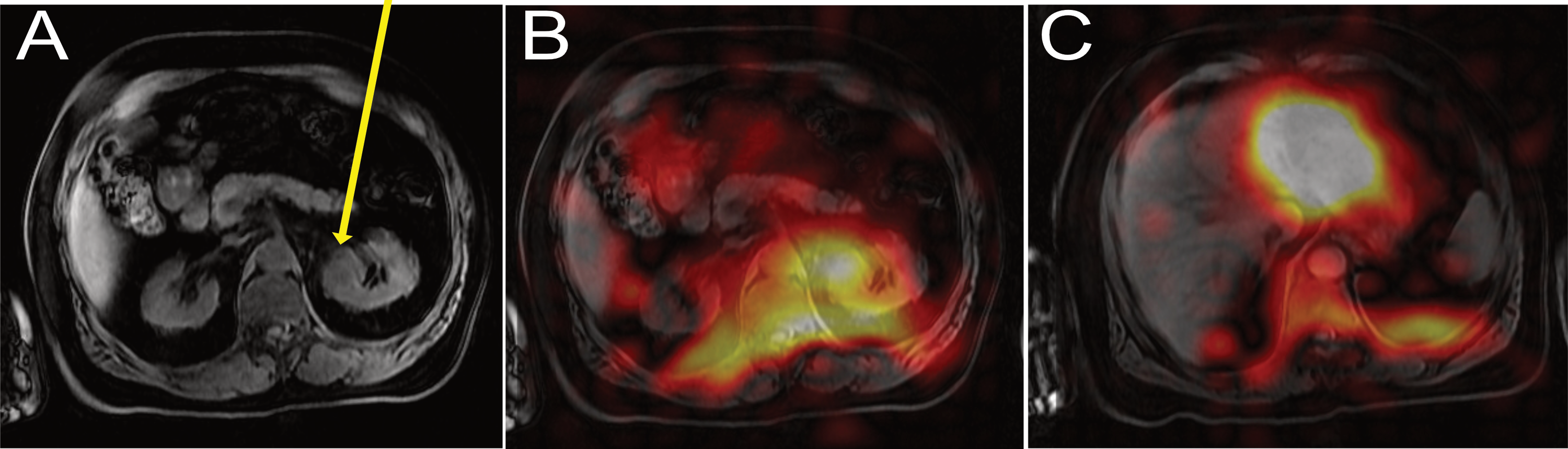
Figure 3: Patient with a renal oncocytoma after drinking D2O. (A) Anatomic image at the level of the tumour (arrow). (B) and (C) Fitted water amplitude zerofilled to 128x128 and overlaid on anatomic images at the level of the tumour and stomach respectively, 12 min after drinking the labelled water.