2999
Advanced Analytics Tools Guide Clinical MRI Protocol Optimization and Quantify Value1Department of Medical Physics, University of Wisconsin-Madison, Madison, WI, United States, 2Department of Radiology, University of Wisconsin-Madison, Madison, WI, United States, 3Department of Emergency Medicine, University of Wisconsin-Madison, Madison, WI, United States, 4Department of Biomedical Engineering, University of Wisconsin-Madison, Madison, WI, United States, 5Department of Medicine, University of Wisconsin-Madison, Madison, WI, United States
Synopsis
Keywords: Data Processing, MR Value
Motivation: Quantifying clinical MRI utilization is essential to identifying opportunities to improve workflow and efficiency and contribute to better patient access and increased value.
Goal(s): We aim to demonstrate the benefits of analytics tools to measure utilization and guide protocol optimization.
Approach: An advanced analytics methodology was developed to identify workflow improvements and measure the impact of protocol interventions.
Results: We quantified the impact of three interventions: 1) MR enterography protocol modification, 2) focused protocols for hepatocellular carcinoma surveillance, and 3) improved communication strategies for oblique image prescription for rectal cancer staging. All interventions were shown to improve MRI workflow and reduce exam time.
Impact: It is currently challenging to quantify the utilization of clinical MRI exams. Through the use of analytics tools to characterize MR exam utilization, opportunities for improvement can be identified. Such tools are essential to improve the value of MRI.
Introduction
Insight into exam utilization is essential to improving MRI value. By optimizing utilization, access to MRI and overall volume can be improved. This improves patient experience since patients are spending less time in the scanner and have better access to care. Imaging analytics can measure utilization to identify areas for potential improvement. Analytics tools can then be used to measure impact.The purpose of this study is to develop an analytics methodology to measure the utilization of clinical MRI exams and demonstrate the utility of the tool to quantify exam efficiency and variability, and guide interventions that improve value.
Methods
Image-level data were acquired retrospectively under approval from the Institutional Review Board, which provided a waiver of informed consent.Studies were extracted from the local Picture Archiving and Communication System (PACS; Change Healthcare, Nashville, TN), Radiology Information System (RIS), and the electronic health record (Epic, Verona, WI) using a data analysis module (Clarity, Epic, Verona, WI). Data from incomplete exams were excluded. Extracted data included the exam time and series acquisition time. The exam time is defined as the time between the first and last image acquisition. Data compilation and analysis were completed using Python.
Student's t-test compared averages, Chi-Square test compared categorical values, and Mood’s median test compared medians. P<0.05 was considered significant.
To demonstrate the utility of this methodology, we quantified the impact of interventions for three MR protocols (Table 1):
1. MR Enterography (MRE):
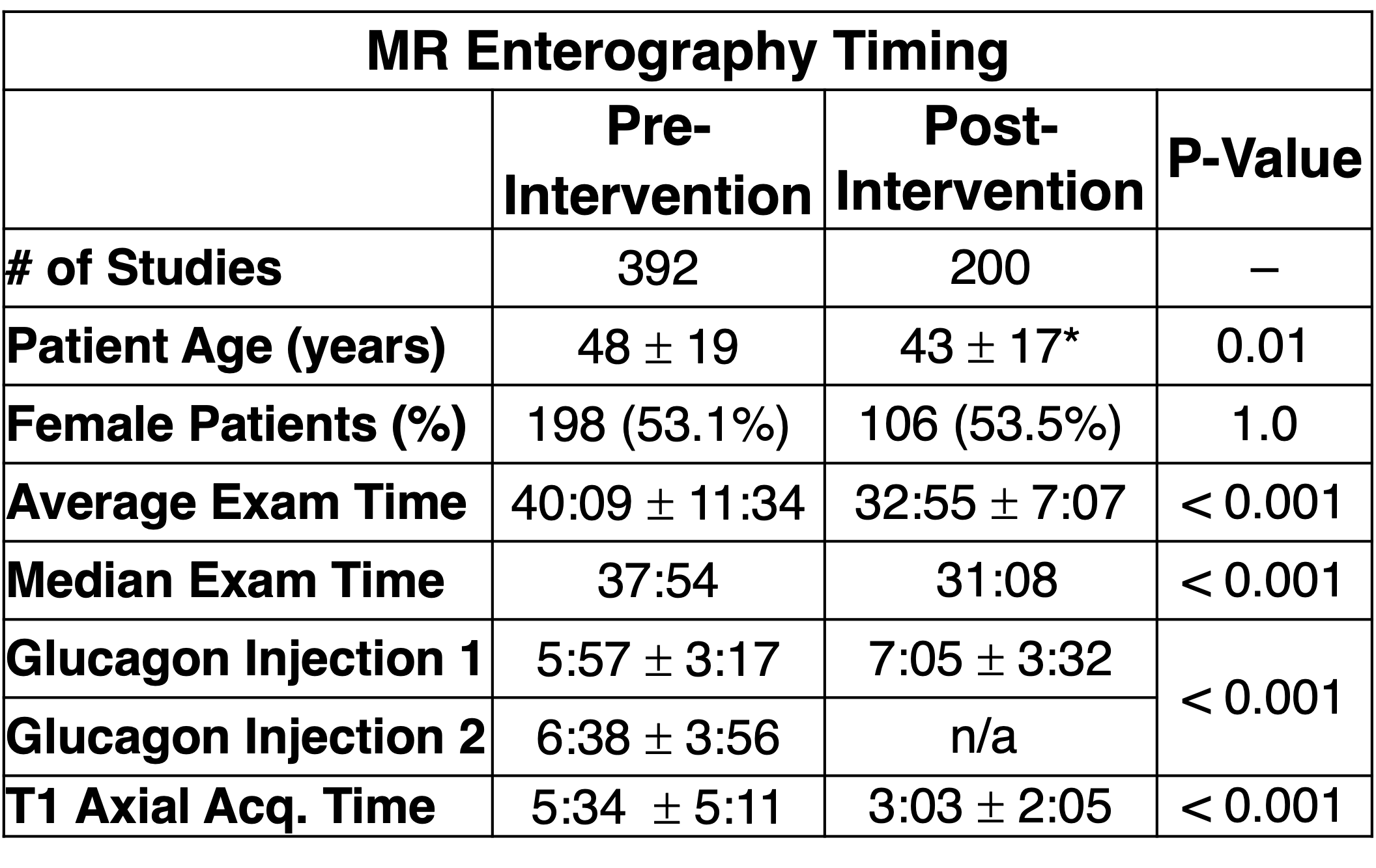
MRE is used in patients with known or suspected Crohn's disease to assess for the presence of active small bowel disease and related complications1. For protocol modification, the two glucagon injections were consolidated into one and delayed 2D T1-weighted axial imaging was replaced with a 3D axial T1-weighted acquisition. Data were acquired from November 2018–October 2019 and February 2022–January 2023 before and after intervention, respectively.
2. Hepatocellular Carcinoma (HCC) screening and surveillance:
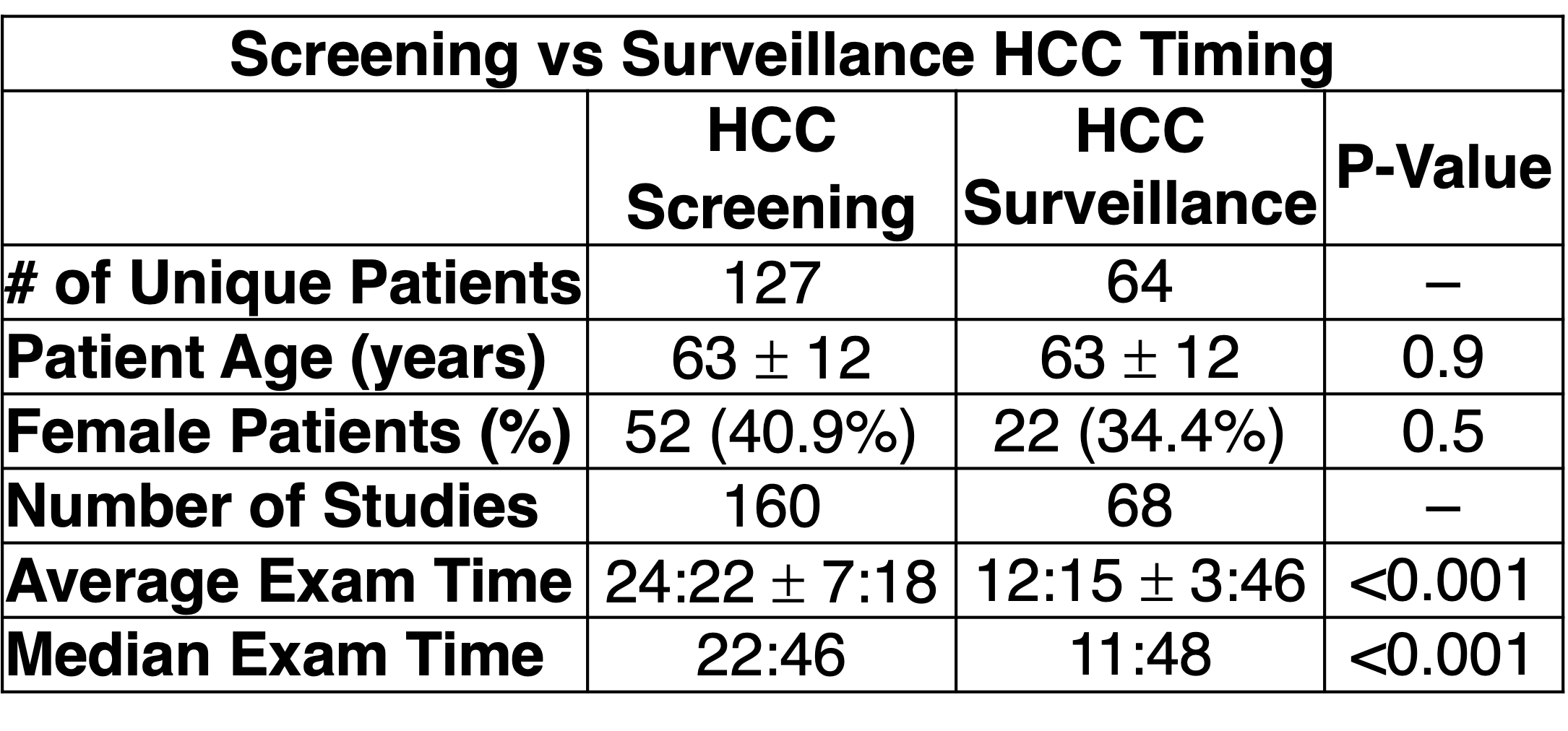
It is recommended that patients with cirrhosis undergo initial screening for HCC followed by surveillance every 6 months2. After initial screening with a complete liver MRI protocol, surveillance is performed with a focused HCC protocol. We evaluated the impact of the focused protocol on exam time. Data were acquired for complete and focused protocols from January 2022–December 2022 and historical data were obtained for patients with a surveillance exam in 2022.
3. Rectal Cancer Staging:
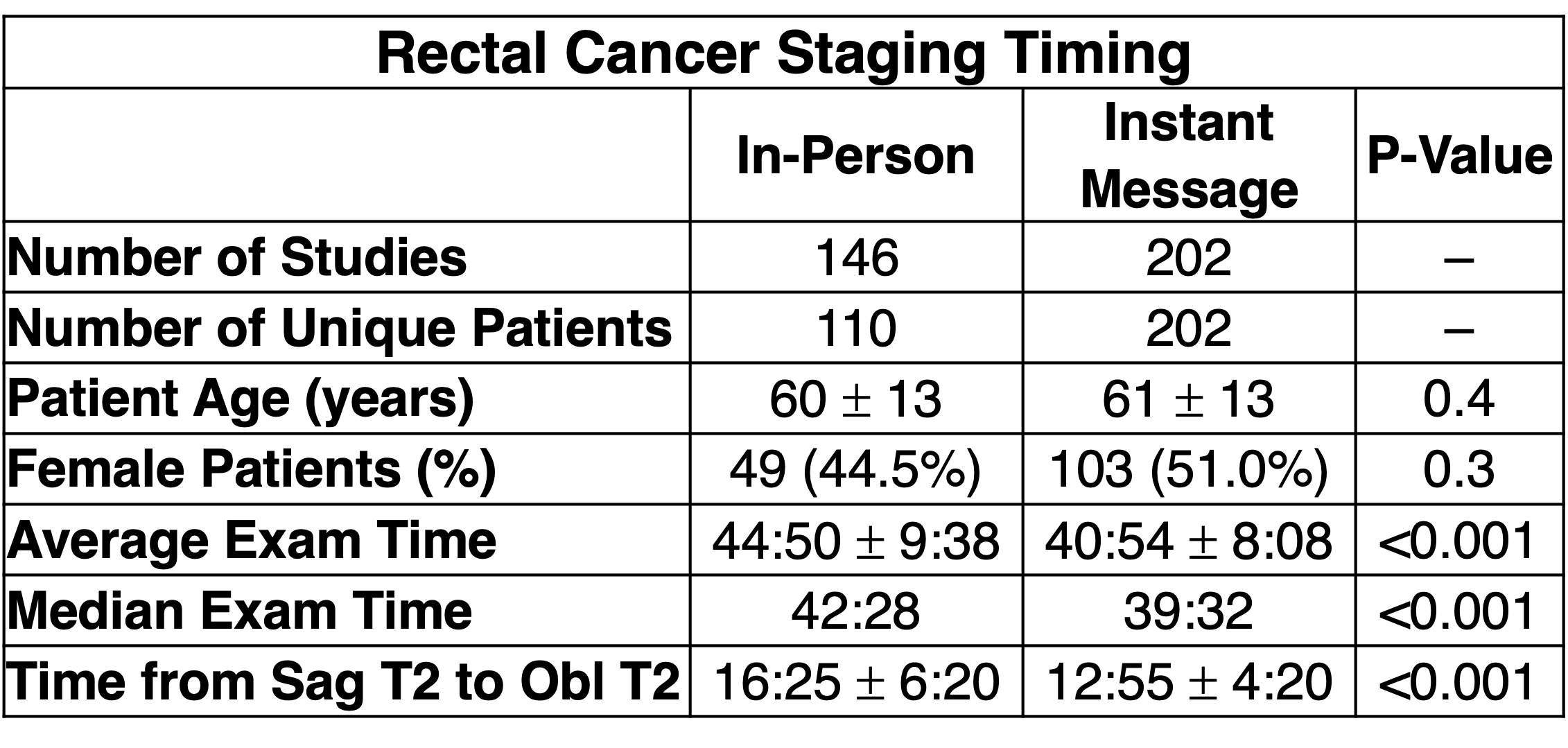
MRI is routinely used to perform TNM staging of newly diagnosed rectal cancer3. Radiologists are contacted after the sagittal T2w acquisition for image plane prescription for high-resolution oblique 2D-imaging planes through the tumor. Previously, this required a physical trip to the scanner console. A workflow overhaul eliminated the trip through the use of PACS-embedded communication technology (Webex, Cisco, San Jose CA). Using Webex’s screenshot and instant messaging (IM) functionality, radiologists now send an annotated screenshot with the image prescription directly from PACS. Data were acquired from April 2020–March 2021 before and June 2021–May 2022 after the implementation of IM.
Results
1. Enterography (Table 2):Prior to intervention, glucagon injections required 6 minutes each, the 2D T1w axial acquisition averaged 5.6±5.2 minutes, and the MRE exam took 40.2±11.6 minutes. After intervention, the average single glucagon injection required 7.1±3.5 minutes, the 3D T1w axial acquisition averaged 3.1±2.1 minutes, and the average exam duration decreased to 32.9±7.1 minutes (p<0.05).
2. HCC screening and surveillance (Table 3&4):
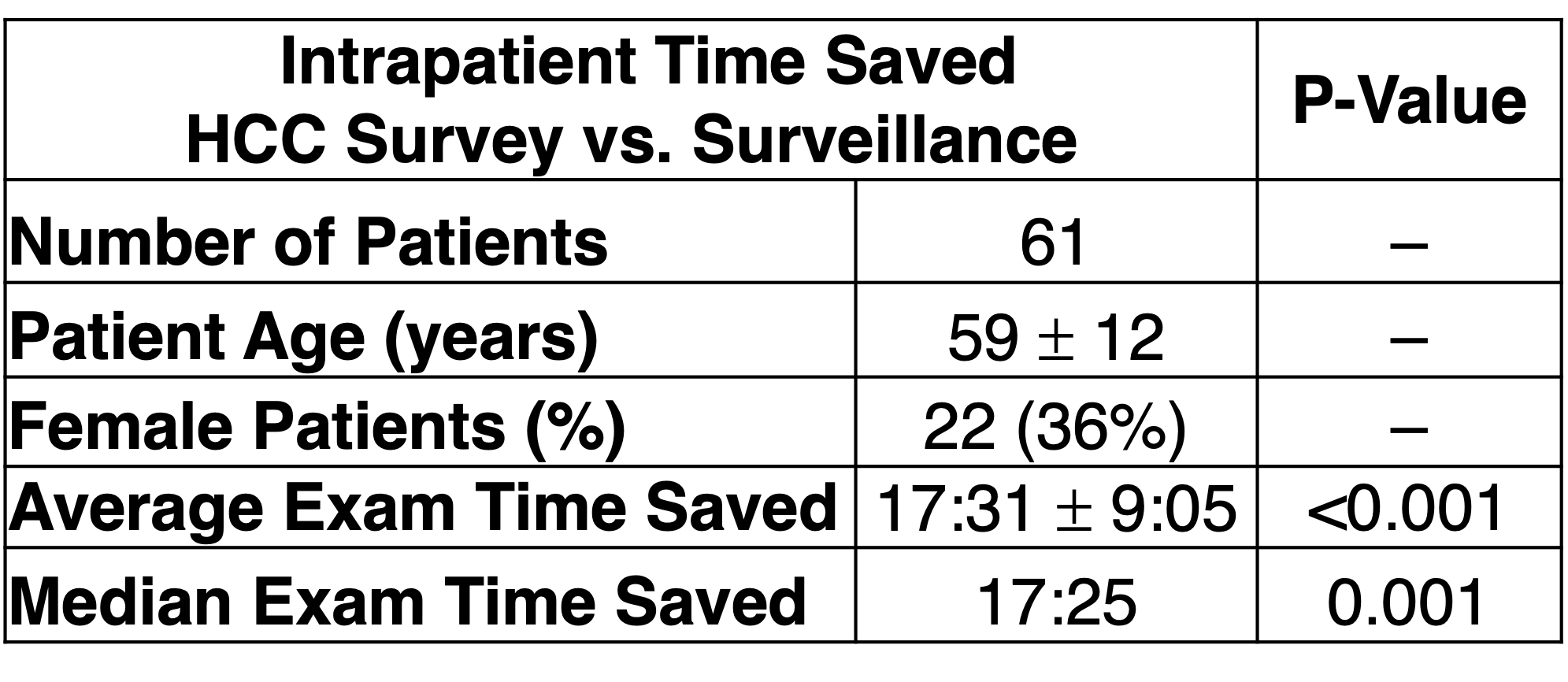
The average screening protocol took 24.4±7.3 minutes, and the surveillance protocol took 12.3±3.8 minutes. In an intrapatient comparison between screening and surveillance protocols, the focused protocol saved 17.5±9.1 minutes on average (p<0.05).
3. Rectal Cancer Staging (Table 5):
Prior to IM, the average exam time between the sagittal T2w and oblique short/long axis T2w series was 16.4±6.3 minutes. Afterward, the average exam time was 12.9±4.3 minutes (p<0.05).
Discussion and Conclusion
In this work, we successfully developed an analytics methodology for quantifying MRI utilization and demonstrated its value through interventions with three protocols. The protocol modification for MRE, focused protocol for HCC surveillance, and improved communication strategies for rectal cancer staging all resulted in a reduction in exam time. We conclude that the application of analytics tools for assessment of MRI utilization provides an objective strategy that permits data-driven decisions to modify protocols and improve value.A limitation to this study is that the time between the images is measured as the time between the end of the previous series, and the start of the next series. However, this metric does not account for other potential patient-related reasons why there could be a prolonged gap between series. Future studies would benefit from additional exam timestamps collected.
Acknowledgements
We wish to acknowledge support from GE Healthcare who provides research support to the University of Wisconsin. Dr. Reeder is the John. H Juhl Endowed Chair of Radiology.
References
1. Low RN, Francis IR, Politoske D, Bennett M. Crohn’s disease evaluation: Comparison of contrast-enhanced MR imaging and single-phase helical CT scanning. J Magn Reson Imaging. 2000;11(2):127-135. doi:10.1002/(SICI)1522-2586(200002)11:2<127::AID-JMRI8>3.0.CO;2-G
2. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358-380. doi:10.1002/hep.29086
3. Amin MB, Greene FL, Edge SB, et al. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67(2):93-99. doi:10.3322/caac.21388
Figures
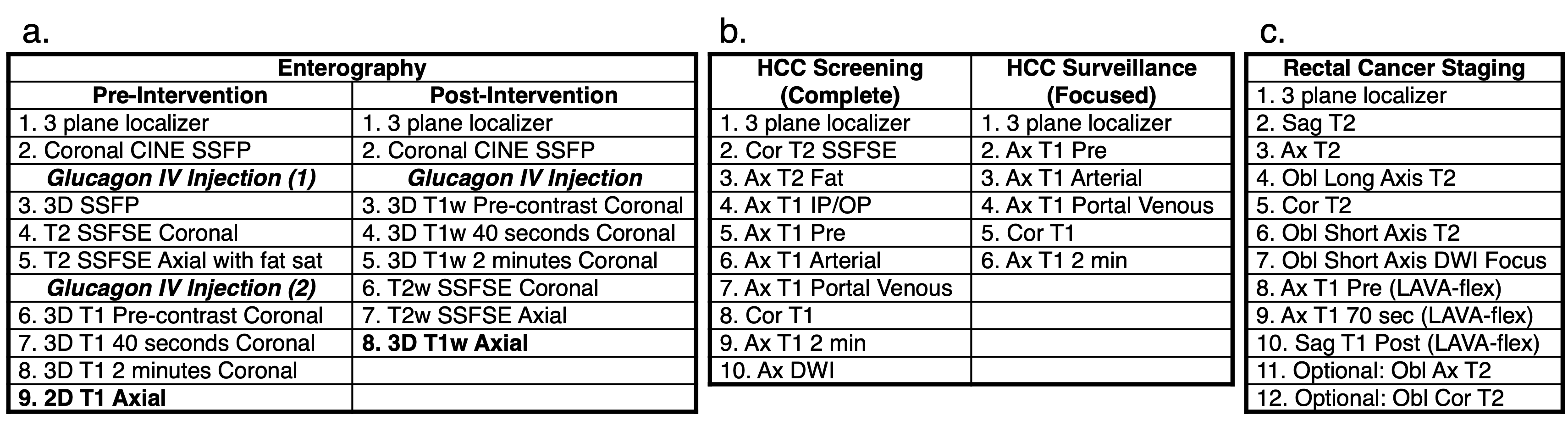
Table 1:
a. MR enterography protocol before and after intervention.
b. Screening versus surveillance protocol for HCC.
c. The rectal cancer staging protocol. This protocol requires prescription of high-resolution oblique 2D imaging planes. Radiologists are contacted after the sagittal T2w acquisition, and the prescription is needed before the oblique long-axis T2w acquisition.