2971
A high-resolution MT-weighted Zero Time Echo sequence for 7T - initial experience with healthy volunteers and Multiple Sclerosis patients1GE Healthcare, London, United Kingdom, 2Department of Radiography, Medical University of Lublin, Lublin, Poland, 3Invicro, Invicro London, London, United Kingdom, 4GE Healthcare, Fairfax, CA, United States, 5ECOTECH, University Maria Curie-Sklodowska, Lublin, Poland
Synopsis
Keywords: Multiple Sclerosis, Neuroinflammation
Motivation: MT-weighted imaging is important for detecting and diagnosing neuro-degenerative disorders. At 7T, high RF power deposition is challenging for MT-weighted sequences and often limits imaging performance.
Goal(s): We demonstrate a high-resolution, MT-weighted, Zero Time Echo (ZTE) sequence which can produce whole-brain images at clinically useful levels of RF power deposition.
Approach: We demonstrate an MT-weighted ZTE sequence for 7T and use it to scan healthy volunteers and subjects with Multiple Sclerosis
Results: Whole-brain MT-weighted ZTE images of high quality and 0.8mm isotropic imaging were produced with clinically useful SAR levels.
Impact: High-resolution MT-weighted ZTE images could provide important novel information for neurologists and psychiatrists.
Introduction
A major motivation of MR at fields of 7T and higher is to obtain MR images with greater sensitivity and resolution. Anatomical MR at 7T can be performed with varying degrees of success using MP2RAGE for T1-weighting, FLAIR for CSF-suppressed T2-weighting and 3D-GRE for T2*-weighting for SWI and QSM1.Another commonly-requested contrast is Magnetisation Transfer (MT). This contrast requires the application of long, high off-resonant RF pulses which give the sequence a high RF power deposition, especially at 7T.
We previously demonstrated a Zero Time Echo MT-weighted sequence2 and showed that the contrast was mostly MT, and was generated by the ASPIR fat saturation pulse. However, that sequence had high RF power deposition, which limited the resolution achievable (1.4mm isotropic) and made the sequence unsuitable for routine clinical use.
Here we present a high-resolution MT-weighted sequence using the same approach, but consideration of the relaxation effects in the RUFIS spoke-train has allowed some improvements. The resulting sequence - "Silent-MT" - produces high-resolution (0.8mm isotropic) MT-weighted ZTE images in scan times varying between 2 (for 1 NEX) and 7 (3 NEX, as used here) minutes for a whole-brain volume, and with a 6-minute average RF power deposition approximately half of the maximum (3.2 W/kg).
We compared Silent-MT from healthy volunteers and patients with Multiple Sclerosis (MS) with corresponding FLAIR images.
Methods
All scans were performed on a General Electric 7T MR950 (7T23 software) using a Nova Medical 2-channel head birdcage coil for RF transmission and a Nova Medical 32-channel array coil for reception. A 3D-radial RUFIS3-based sequence applying Fat Saturation with an ASPIR4 pulse was implemented and optimised for use at 7T. The duty cycle of the Fat Sat pulse was regulated in order to control the MT weighting of the sequence. FLAIR5 images in "SNR-optimal mode" were also acquired in healthy controls and patients with Multiple Sclerosis.Sequence parameters: Silent-MT - matrix 224, FOV 17.6cm, voxel size 0.8mm, NEX 3, spokes/segment 224, scan time 6min 30s. FLAIR - matrix 224x200, FOV 22.4x20cm, isotropic voxel size 1mm, NEX 0.75, TR 10s, TE 103ms, TI 2383ms, ETL 240, ARC phase/slice 2/1, scan time 8min 34s.
The FLAIR images were aligned to the Silent-MT images using flirt (FSL6) in an affine transformation with the normalised mutual information cost function and reconstructed into the same space as the Silent-MT images with sinc interpolation. Images were then reviewed by the authors.
Results
Here we only report initial anecdotal observations of these images; a more complete radiological review is being prepared in a larger cohort.All 7T MR images showed the familiar intensity variations associated with the Nova Medical receiver array coil.
The Silent-MT images showed strong contrast between CSF, Gray and White Matter rather like that which is seen in T2-weighted images. This contrast remained uniform across the cerebrum and cerebellum, and seemed to be less affected by the transmit B1 inhomogeneity normally observed in the head at 300MHz.
Compared to the FLAIR images, some additional features were observed on the Silent-MT images. Many lesions were detected in MS patients, usually in the same location on both contrasts. We qualitatively observed trends of both a greater number of lesions and an overall increase in lesion conspicuity in the Silent-MT images.
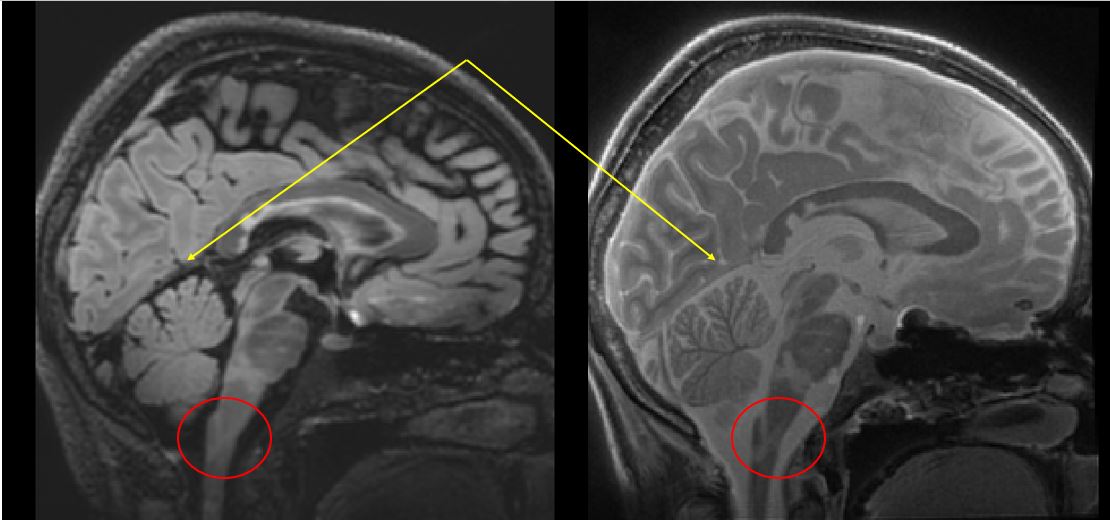
Fig 1 shows FLAIR and Silent-MT in an MS patient. Numerous small lesions in the chronic state are black in FLAIR, but white in Silent-MT. The brain-stem is clearer in the Silent-MT image, as is a possible additional brain-stem lesion inferiorly.
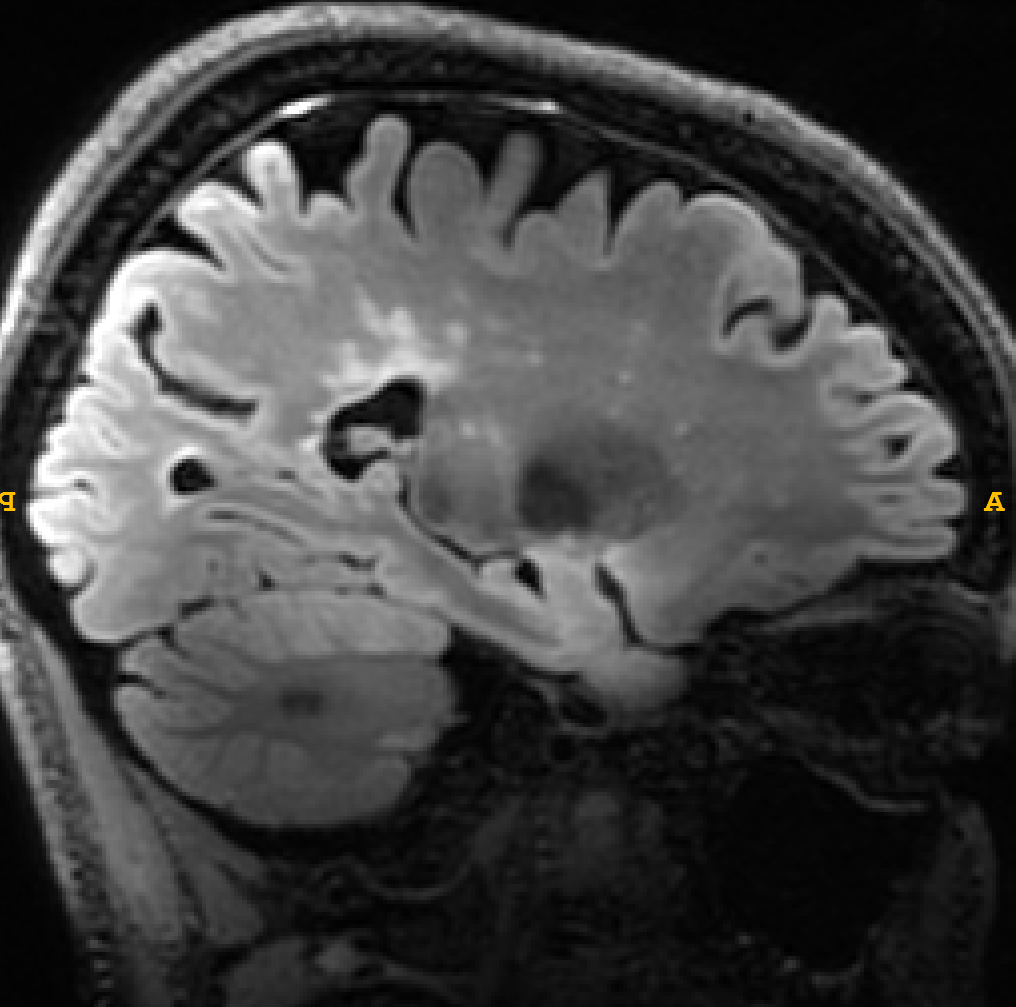
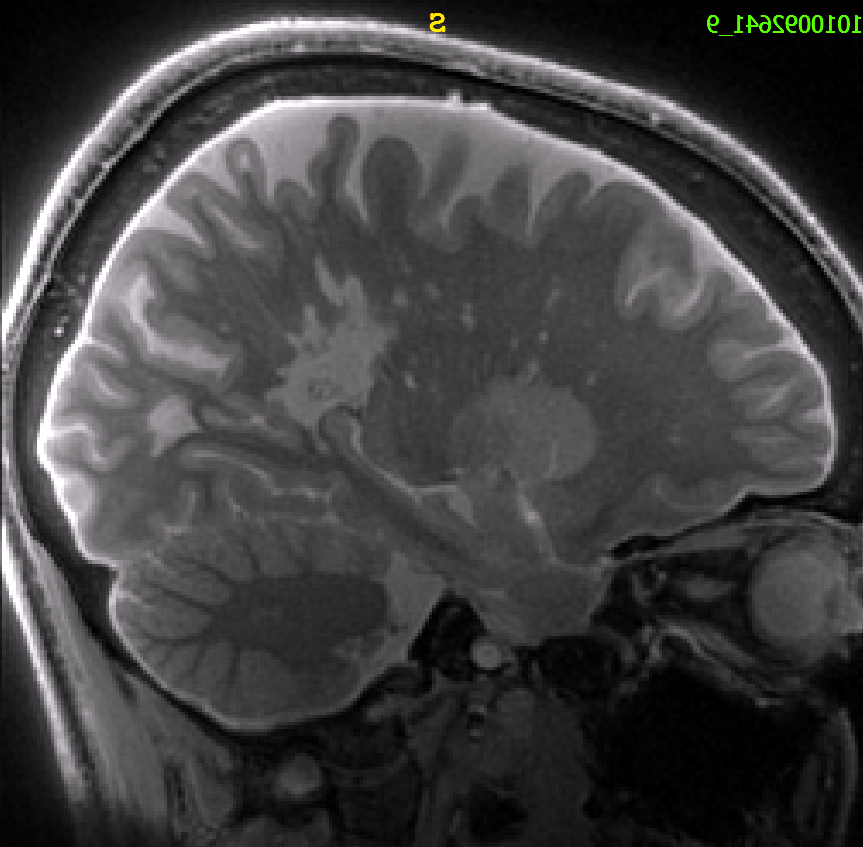
Fig 2 shows FLAIR and fig 3 shows Silent-MT in another MS patient. MS lesions are generally more conspicuous and numerous on the Silent-MT image. The larger supra-tentorial posterior lesion in the Silent-MT suggests greater sensitivity to large biomolecules associated with a perivenular inflammation.
Discussion
Silent-MT offers a robust whole-head contrast for 7T MR. Silent-MT may give unique information about substances with short-T2 signals such as large biomolecules and so provide additional information about patients with MS and neurodegenerative diseases. Short-T2 signals can be observed both indirectly, through the well-studied model of Transfer of Magnetisation from (semi-)solid pools to liquid pools7, and more directly due to Silent-MT's Zero Time of Echo acquisition. This may increase the sensitivity of Silent-MT to the build-up of large biomolecules associated with neuro-inflammation.Acknowledgements
No acknowledgement found.References
1 Waiczies S, Els A, Kuchling J, Markenroth Bloch K, Pankowska A, Waiczies H, Herrmann C, Chien C, Finke C, Paul F, Niendorf T. Magnetic Resonance Imaging of Multiple Sclerosis at 7.0 Tesla. J Vis Exp. 2021 Feb 19;(168).
2 M Symms, M Costagli, G Buonincontri, F Wiesinger, D Kelley, M Janich, G Aringhieri, M Marletta, G Barker, V Zampa, M Cosottini, M Tosetti. Zero Time of Echo imaging with an Adiabatic Fat Suppression Pulse at 7T. Proc ISMRM 2018 (Paris) #326.
3 D Madio, I Lowe. Ultra-fast imaging using low flip angles and FIDs. Magn Reson Med. 1995Oct;34(4):525-9.
4 https://mriquestions.com/spair-v-spir.html
5 M Saranathan, T Tourdias, AB Kerr, J Bernstein, GA Kerchner, MH Han, BK Rutt. Optimization of Magnetization-Prepared 3-Dimensional Fluid Attenuated Inversion Recovery Imaging for Lesion Detection at 7 T. Invest Radiol 2014;49:290-298
6 https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/
7 Henkelman RM, Huang X, Xiang QSS, Stanisz GJ, Swanson SD, Bronskill MJ. Quantitative Interpretation of Magnetization Transfer. Magnetic resonance in medicine 1993; 29(6): 759–766.
Figures