2958
Patient-Centered Neurological Evaluation of Functional MRI Outcomes in Multiple Sclerosis1Vanderbilt University Institute of Imaging Science, Nashville, TN, United States, 2Vanderbilt University School of Medicine, Nashville, TN, United States, 3Department of Neuroinflammation, Queen Square Institute of Neurology, London, United Kingdom, 4Department of Radiology and Radiological Sciences, Vanderbilt University Medical Center, Nashville, TN, United States, 5Department of Biomedical Engineering, Vanderbilt University, Nashville, TN, United States, 6Department of Neurology, Neuroimmunology Division, Vanderbilt University Medical Center, Nashville, TN, United States
Synopsis
Keywords: Multiple Sclerosis, Multiple Sclerosis
Motivation: Multiple sclerosis (MS) is the most common neurodegenerative disease in young adults with significant gaps in spinal cord (SC) imaging necessitating advanced techniques like fMRI to better characterize MS pathology.
Goal(s): We aim to explore SC functional connectivity (FC) via resting-state functional MRI (fMRI) to disentangle the complex interactions between biological variables, disease metrics, and synchronous BOLD activity.
Approach: We acquired mFFE and fMRI images in MS patients and healthy controls (HC), performed image post-processing, and analyzed correlations between 6 gray matter (GM) networks.
Results: SC FC differs significantly depending on cohort and subject characteristics, like disease metrics and biological variables like gender.
Impact: Implications include a robust analytical evaluation of the rs-fMRI signatures arising in the MS SC and their relationship to functional integrity. By understanding fMRI in the SC of MS patients, we may better understand the human experience of MS.
Introduction
Multiple sclerosis (MS) is a chronic demyelinating disease with over 1 million individuals affected in the US. MS diagnosis follows from lesions disseminated in time and space, including lesions in the spinal cord (SC)1. However, the SC has been often understudied given the challenges of imaging a small, physiologically noisy space despite the association with SC lesions and a higher risk of relapse2. Functional MRI (fMRI) can probe SC function in MS patients; resting-state (rs-fMRI) relies on blood oxygenation level-dependent (BOLD) contrast to link neuronal activity with local tissue hemodynamic processes, which when spatially correlated provides a measure of functional connectivity (FC)3. Prior SC rs-fMRI outlined ventral-ventral (motor) and dorsal-dorsal (sensory) gray matter connectivity in healthy controls4,5. In MS, fMRI FC correlated with abnormal DTI indices6, suggesting related structural-functional abnormalities. The question remains whether SC fMRI FC alterations are related to disability and clinical manifestations of MS, connecting the radiological with the neurological.Methods
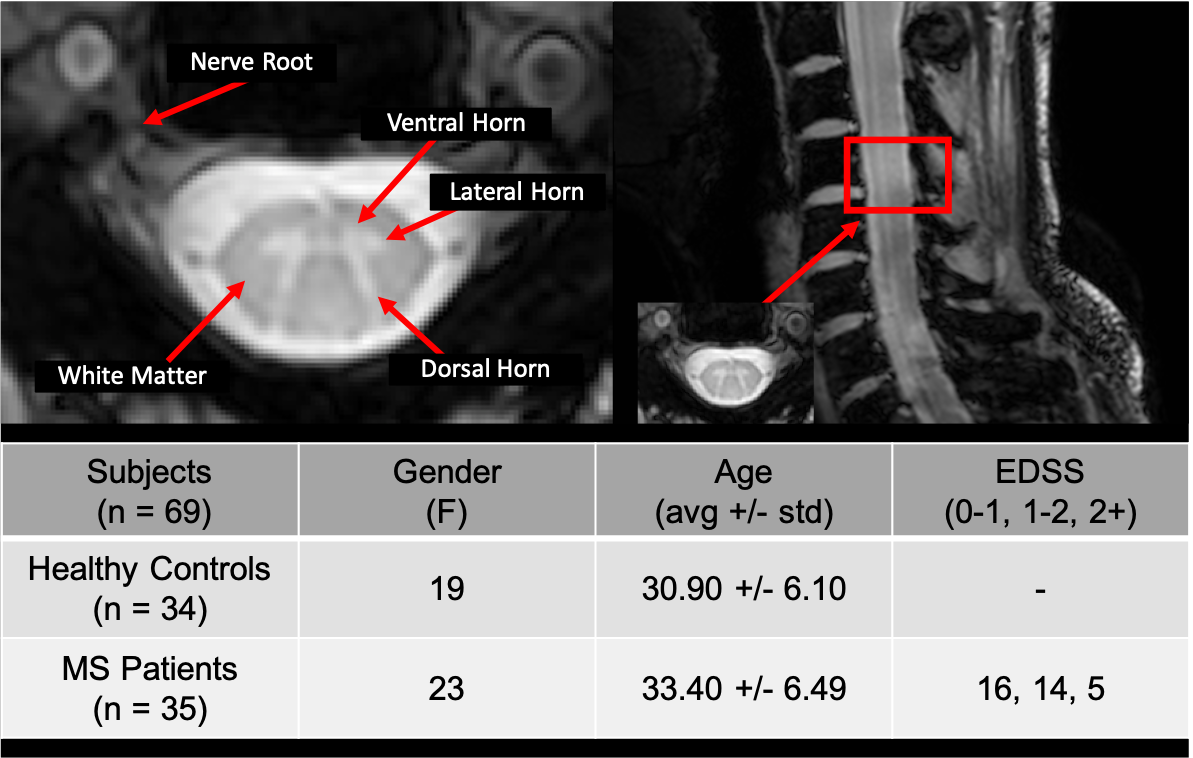
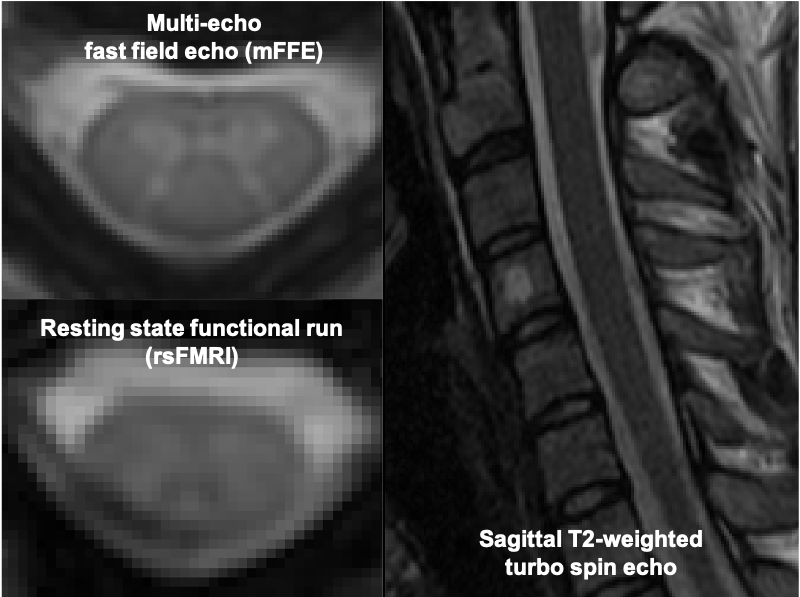
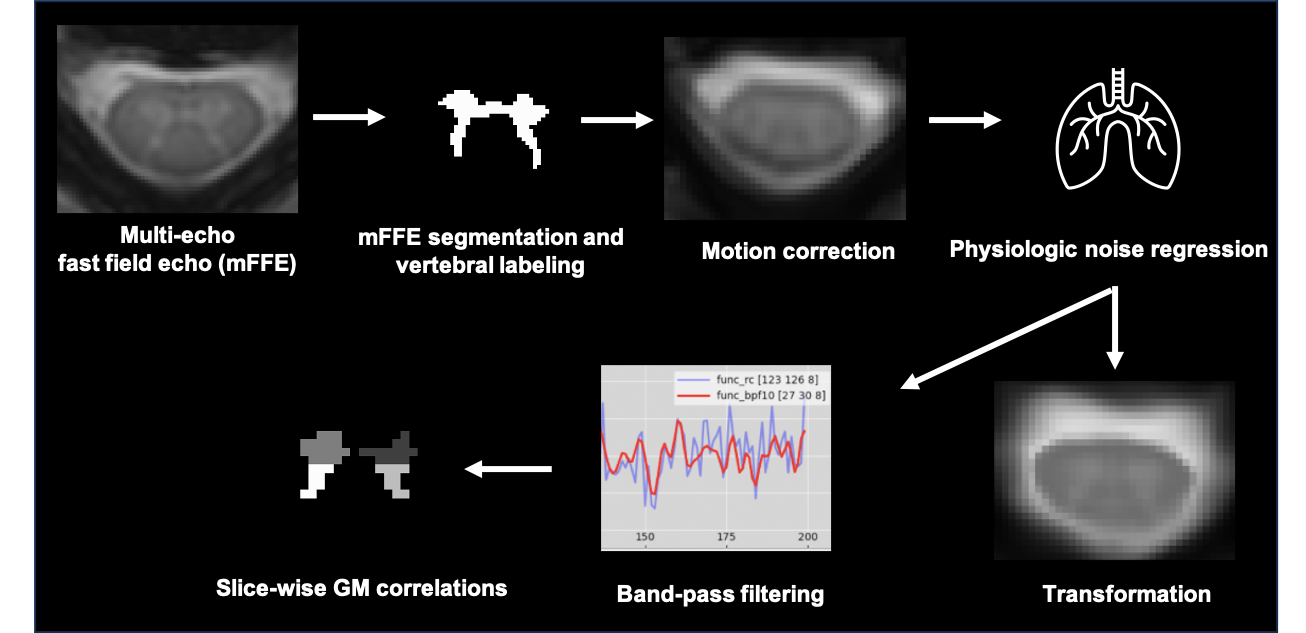
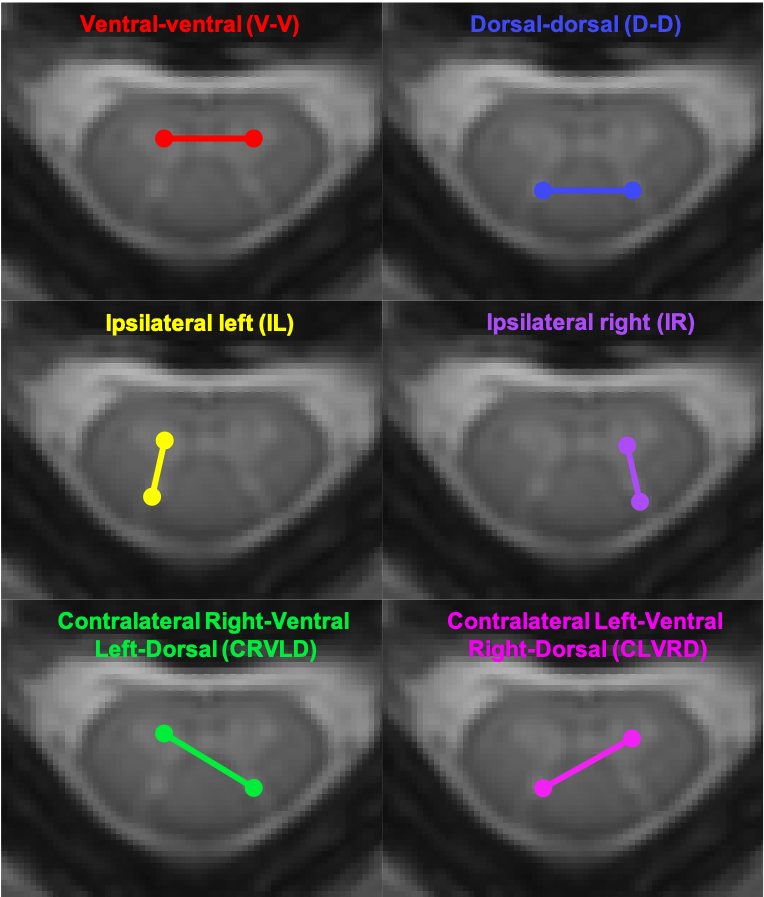
All studies were approved by the local IRB with informed consent prior to examination. 34 healthy controls (HCs, age 30.90+/-6.20, 19 females) and 35 relapsing-remitting MS patients (age 33.40+/-6.49, 23 females, EDSS<3.5) were enrolled. Subjects completed sensorimotor testing, including the timed up-and-go (TUG)7, 25-foot walk, and extremity strength and vibration sensitivity8, prior to scanning. MRI was performed on a 3T Philips Elition (Philips Medical Systems, Best, The Netherlands) using a dual-channel transmit body coil and 16-channel neurovascular coil for signal reception. Imaging was centered at C3 (Figure 1) and physiological data (cardiovascular/respiratory traces) were acquired using chest bellows and pulse oximeter. The rs-fMRI acquisition is described in Figure 2. Image processing (Figure 3) was adapted from Barry et al. and Combes et al.4,6 and utilized Spinal Cord Toolbox (SCT)9 and FSL10,11. Data output included FC among each of 6 GM networks with corresponding Pearson-correlation coefficients (Figure 4). FC was averaged across all slices per subject, and all subjects per cohort/bin. We binned subjects into quartiles for each SMT and clinical measurement to examine individual contributions of FC within a cohort. We evaluated intra-subject GM network FC differences, mean FC between MS patients and HCs, and comparison of quartiles between MS patients and controls for each SMT metric and biologic variable. Student’s t-test was used to compare within-subject FC, Welch’s test for MS vs HC FC per region, and multiple linear regression to account for confounding variables when considering FC and disease metrics.Results
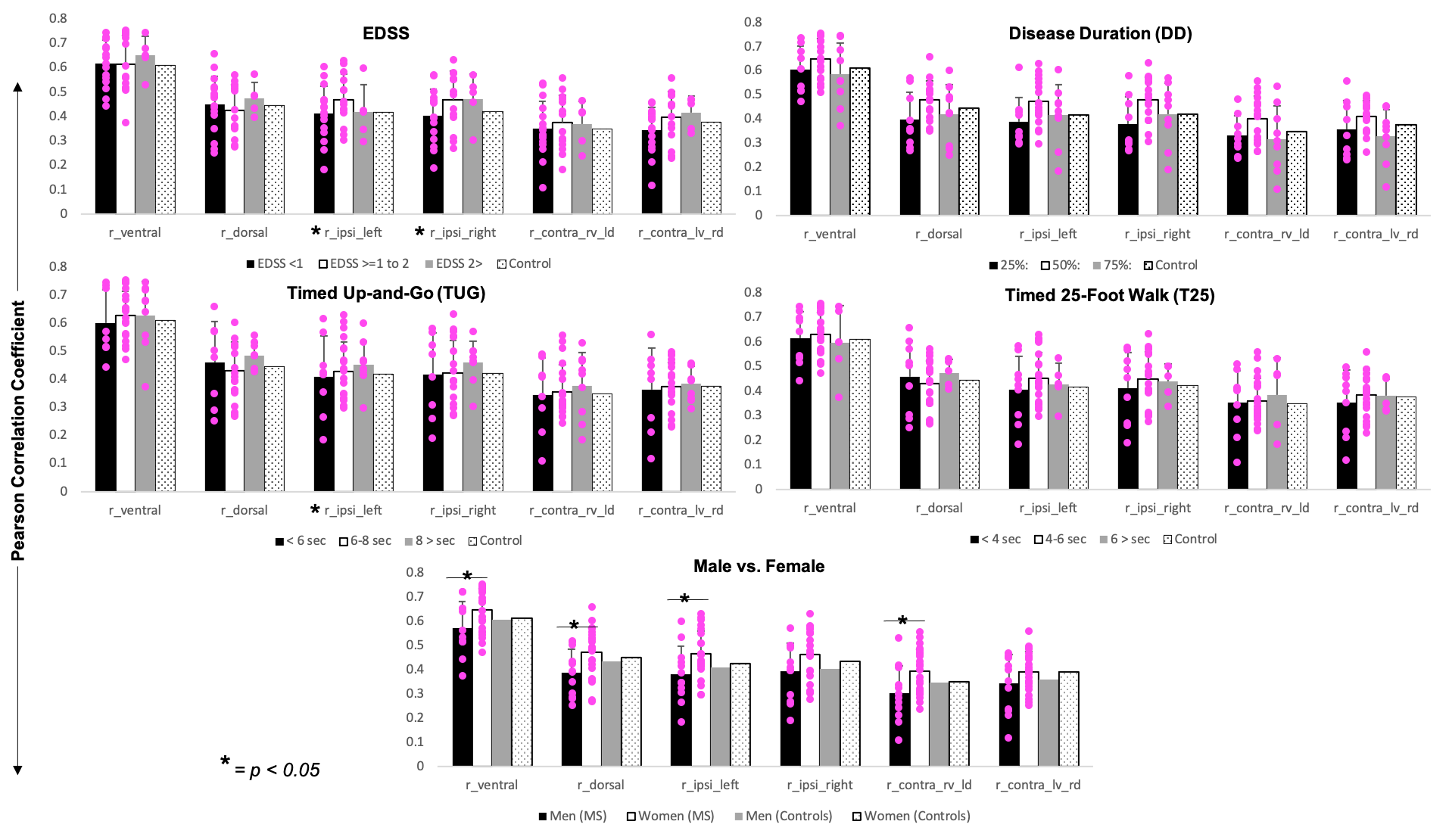
For both HC and MS patients, the average ventral-ventral (V-V) FC was significantly greater than dorsal-dorsal (D-D) FC (p<0.01) compared to the other networks, though the V-V and D-D FC did not differ significantly between cohorts. When binning patients based on gender and disability, D-D FC and gender and V-V and gender were significantly correlated (p=0.03, p=0.04) when controlling for age, EDSS, TUG, 25-foot walk, and disease duration. MS females have significantly higher V-V, D-D, ipsilateral left (IL), and contralateral right ventral left dorsal (CRVLD) FC (p=0.05, p=0.03, p=0.05, p=0.03) compared to MS males, with no significance between control female and males. In patients, most metrics showed increased FC across bottom to middle quartile ranges. When considering the middle quartiles of each disability metric and controlling for age and gender, EDSS was significantly correlated with IL and IR FC (p<0.01, p=0.05) and TUG was significantly correlated with IL FC (p<0.01) (Figure 5).Discussion
Considering MS is a heterogenous disease, we anticipated FC for patients at the high- and lower disability quartiles would diminish differences between grouped cohorts and thus binned our data to capture this variation. FC peaked in the middle quartiles of disability metrics. In MS, the integrity of functional networks may be compromised, as suggested by increased FC earlier in the disease process and decreased FC as adaptive mechanisms become exhausted 12,13. We confirmed previous findings of high ventral FC compared to other regions and gender-differences in FC5,6, though we found gender-differences of increased female FC in MS but not in healthy controls. Women with MS often have a better prognosis and less neurodegenerative brain changes compared to men and, since resting state brain and SC networks are functionally integrated14,15, we posit higher connectivity may delay disease progression. Additionally, ipsilateral FC and EDSS and TUG were associated, suggesting altered intra-slice connectivity may contribute to disease severity.Conclusion
fMRI evaluation of FC in the MS SC shows differences in both gender and disability. Further research involving FC and lesion burden is needed to evaluate lesion impact and disentangle the effects of biologic and disease metrics on connectivity assessments.Acknowledgements
I would like to acknowledge Dr. Gore, Dr. Smith, the VUIIS radiology technicians, and the subjects who contributed to this work.References
1. Mantero V, Abate L, Balgera R, Mantia L La, Salmaggi A. Clinical Application of 2017 McDonald Diagnostic Criteria. J Clin Neurol. 2018;14(3):387-392.
2. Moccia M, Ruggieri S, Ianniello A, Toosy A, Pozzilli C, Ciccarelli O. Advances in spinal cord imaging in multiple sclerosis. Ther Adv Neurol Disord. 2019;12:1756286419840593. doi:10.1177/1756286419840593
3. Cohen-Adad J, Gauthier CJ, Brooks JCW, et al. BOLD signal responses to controlled hypercapnia in human spinal cord. Neuroimage. 2010;50(3):1074-1084. doi:https://doi.org/10.1016/j.neuroimage.2009.12.122
4. Barry RL, Rogers BP, Conrad BN, Smith SA, Gore JC. Reproducibility of resting state spinal cord networks in healthy volunteers at 7 Tesla. Neuroimage. 2016;133:31-40. doi:https://doi.org/10.1016/j.neuroimage.2016.02.058
5. Conrad BN, Barry RL, Rogers BP, et al. Multiple sclerosis lesions affect intrinsic functional connectivity of the spinal cord. Brain. 2018. doi:10.1093/brain/awy083
6. Combes AJE, O’Grady KP, Rogers BP, et al. Functional connectivity in the dorsal network of the cervical spinal cord is correlated with diffusion tensor imaging indices in relapsing-remitting multiple sclerosis. NeuroImage Clin. 2022;35:103127. doi:https://doi.org/10.1016/j.nicl.2022.103127
7. Sebastião E, Sandroff BM, Learmonth YC, Motl RW. Validity of the Timed Up and Go Test as a Measure of Functional Mobility in Persons With Multiple Sclerosis. Arch Phys Med Rehabil. 2016;97(7):1072-1077. doi:10.1016/j.apmr.2015.12.031
8. Newsome SD, Wang JI, Kang JY, Calabresi PA, Zackowski KM. Quantitative measures detect sensory and motor impairments in multiple sclerosis. J Neurol Sci. 2011;305(1-2):103-111. doi:10.1016/j.jns.2011.03.003
9. De Leener B, Lévy S, Dupont SM, et al. SCT: Spinal Cord Toolbox, an open-source software for processing spinal cord MRI data. Neuroimage. 2017. doi:10.1016/j.neuroimage.2016.10.009
10. Jenkinson M, Beckmann CF, Behrens TEJ, Woolrich MW, Smith SM. FSL. Neuroimage. 2012;62(2):782-790. doi:10.1016/j.neuroimage.2011.09.015
11. Smith SM, Jenkinson M, Woolrich MW, et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage. 2004;23 Suppl 1:S208-19. doi:10.1016/j.neuroimage.2004.07.051
12. Faivre A, Rico A, Zaaraoui W, et al. Assessing brain connectivity at rest is clinically relevant in early multiple sclerosis. Mult Scler. 2012;18(9):1251-1258. doi:10.1177/1352458511435930
13. Roosendaal SD, Schoonheim MM, Hulst HE, et al. Resting state networks change in clinically isolated syndrome. Brain. 2010;133(Pt 6):1612-1621. doi:10.1093/brain/awq058
14. Ceccarelli A. Structural and functional brain damage in women with multiple sclerosis: A mini-review of neuroimaging sex-based studies . Front Neurol . 2022;13. https://www.frontiersin.org/articles/10.3389/fneur.2022.1057446.
15. Vahdat S, Khatibi A, Lungu O, et al. Resting-state brain and spinal cord networks in humans are functionally integrated. PLoS Biol. 2020;18(7):e3000789. doi:10.1371/journal.pbio.3000789
Figures