2957
Subtraction Map Pipeline to Assess Longitudinal Changes in Multiple Sclerosis at Portable Ultra-Low-Field MRI1NINDS, NIH/Oxford, Bethesda, MD, United States, 2Nuffield Department of Clinical Neurosciences, Oxford University, Oxford, United Kingdom, 3NINDS, NIH, Bethesda, MD, United States, 4Hyperfine Inc, Guilford, CT, United States, 5NIH, Bethesda, MD, United States
Synopsis
Keywords: Visualization, Low-Field MRI, Multiple Sclerosis, Longitudinal, White Matter Lesions
Motivation: Ultra-low-field (ULF) MRI is more patient-accessible due to its cost effectiveness and portability and could in principle allow more frequent follow-up in disabling neurological diseases like multiple sclerosis (MS). However, using ULF MRI to track longitudinal changes is challenging due to reduced SNR and CNR.
Goal(s): To develop an ULF longitudinal subtraction pipeline.
Approach: We developed a subtraction pipeline for ULF images and assessed longitudinal changes in 14 scans from 12 MS participants. Results were compared with an MS neurologist’s impression of high-field images.
Results: Our pipeline was able to detect new lesions and longitudinal changes in MS on par with high-field MRI.
Impact: A longitudinal subtraction pipeline, implemented on ultra-low field MR images, was useful for monitoring interval changes in patients with MS, augmenting the clinical utility of follow-up MRI.
Introduction
Ultra-Low Field Magnetic Resonance Imaging (ULF MRI) has the potential to transform the accessibility of MRI due to its reduced cost, diminished infrastructural demands, and enhanced portability1. An exciting prospect of ULF MRI is its promise to enable cost-effective, frequent longitudinal follow-up scans at the point-of-care, particularly relevant in neurological disorders like multiple sclerosis (MS). In MS, radiological follow-up with conventional MRI is essential for detecting new demyelinating white matter lesions (WML) and changes within these lesions, offering critical insights into disease activity and treatment response2.Even with more conventional high-field MRI (1.5T, 3T), changes in MS lesions can be subtle. Subtraction maps accentuate the visibility of new lesions and changes in lesion size, greatly facilitating the identification of pathologic changes for radiologists and clinicians. Such maps can be generated by voxelwise subtractions of registered and normalized longitudinal MRI images3. However, in the context of ULF MRI, the development of subtraction map pipelines presents added challenges. Processing ULF MRI scans is inherently complex, compounded by the fact that open-source MRI software tools are primarily optimized for more conventional 1.5T or 3T MRI systems. Prior research has highlighted the clinical utility of ULF MRI in the context of MS, demonstrating its ability to detect WML exceeding 4mm4. However, the sensitivity of detecting longitudinal changes in MS at ULF is not known. We aim to develop a subtraction pipeline at ULF to assess longitudinal changes in MS.
Methods
Longitudinal ULF MRI data were acquired in participants of the Natural History of MS Study protocol at the NIH (NCT00001248). Ethical approval was obtained from the institutional IRB, and all participants provided written informed consent.ULF FLAIR scans were acquired using the 64mT Hyperfine SWOOP system (software version: rc8.6.0) and included the standard FLAIR Axial scan (3D FLAIR, TR=4s TE=166.72, TI=1426ms, scan time=10.15 minutes with an in-plane resolution of 1.7mm x 1.7mm and a slice thickness of 5mm).
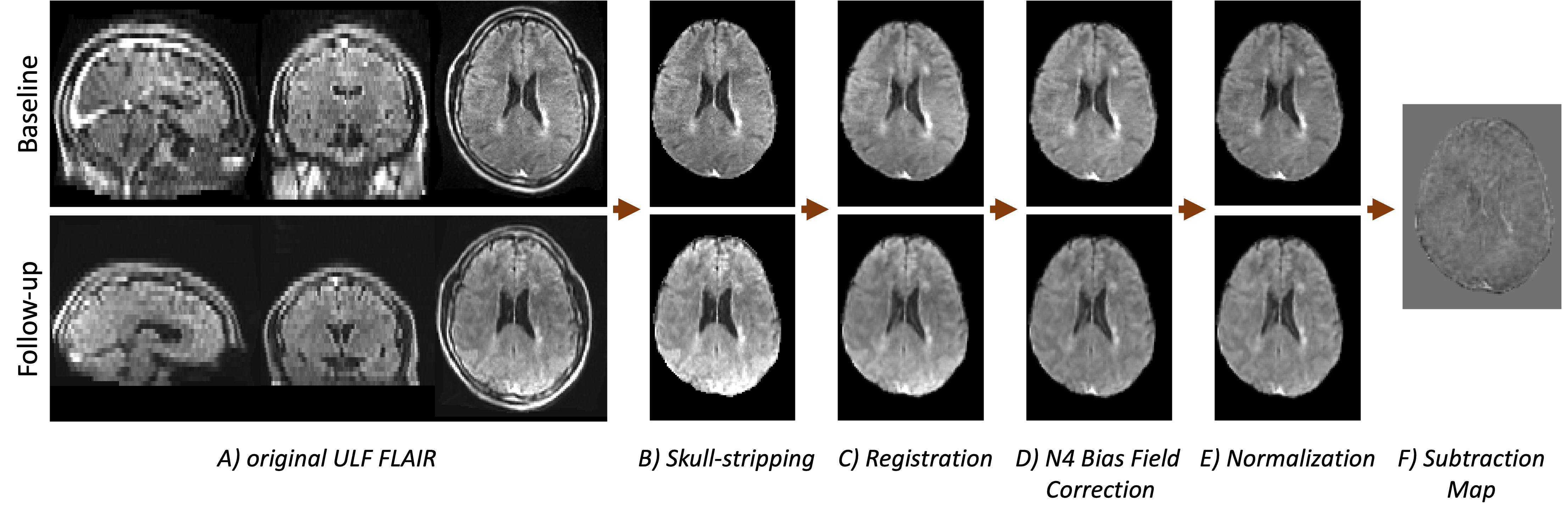
Images were skull-stripped using Synth Strip5 (Fig 1B) and then nonlinearly registered using ANTs's multivariate template construction tool6 with linear interpolation (Fig 1C). Skull-stripped images were bias-field corrected7 (Fig 1D), and intensities were normalized using z-score normalization (Fig 1E). Finally, ULF FLAIR images were subtracted from a follow-up scan to create voxelwise subtraction maps (Fig 1F).
The subtraction pipeline was tested in a cohort of 12 participants diagnosed with MS or clinically isolated syndrome (CIS) with at least one follow-up scan (mean time between scans=0.71±0.038[OS([1] years). A neurologist (with 5 years of experience in MS neuroimaging) visually assessed the quality of subtraction maps and registered images in a HF-MRI-blinded fashion, then compared them with the same-day 3T counterparts, thereby gauging the utility of subtraction maps to help detect lesion changes.
Results
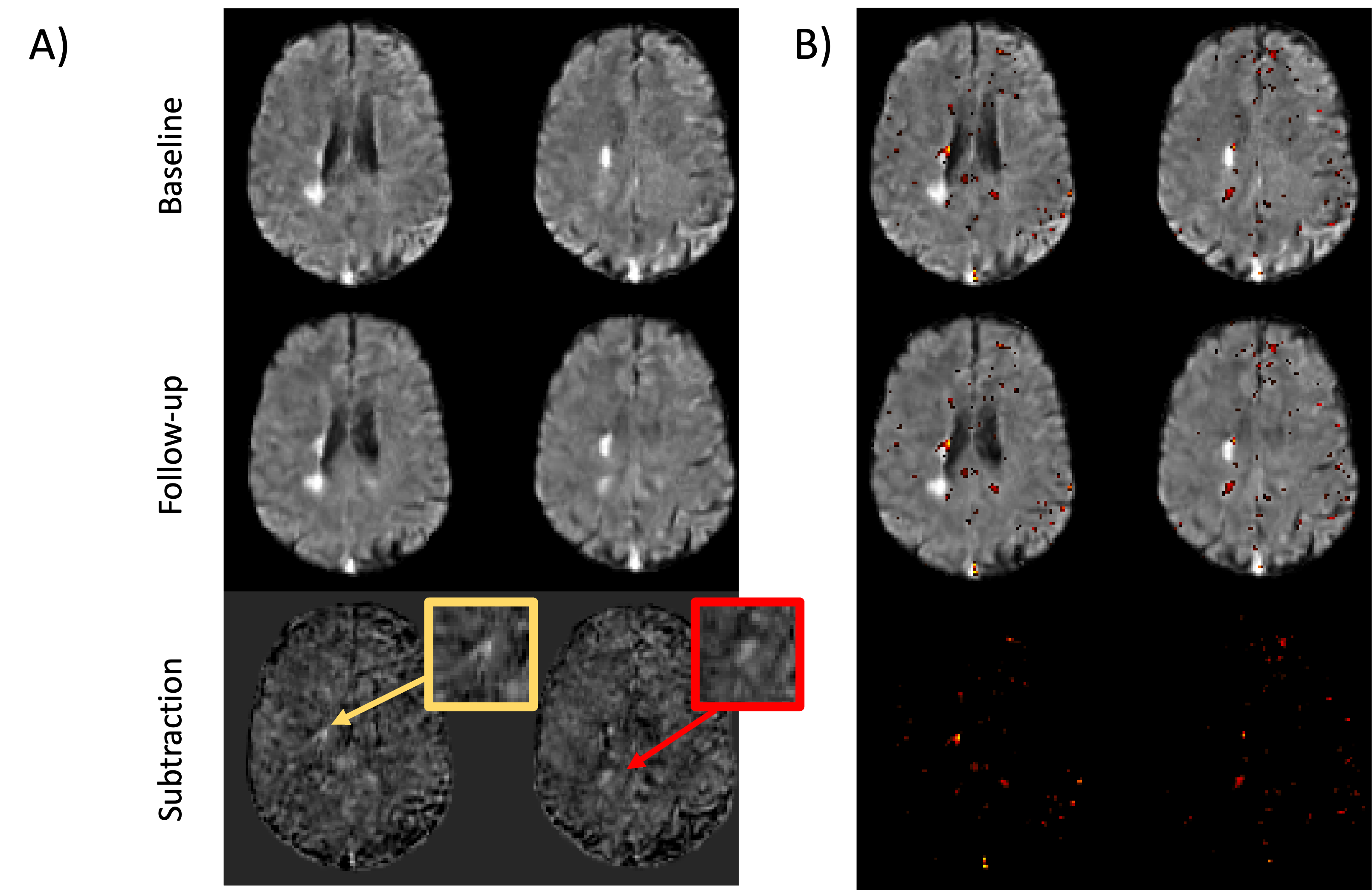
Synthstrip and ANTs multivariate template construction tool consistently performed the best skull stripping and registration when compared visually to other open-source tools. An example case of ULF scan at baseline and after a 1.06-year follow-up are shown before and after subtraction (Fig 2) in a 39-year-old participant diagnosed with relapsing-remitting MS, highlighting two expanding lesions. In one subtly expanding lesion (Fig 2A, yellow box), the lesion center displayed greater homogeneity in comparison to the higher intensity at the lesion edge, corresponding to the area of expansion. The second example (Fig. 2A, red box) shows a more obvious example, where higher intensities correspond to a new lesion. When thresholding and overlaying the subtraction map on the preprocessed FLAIR images, changes in red hues are visible where both lesions are expanding. Importantly, noise in some areas can cause apparent changes in the subtraction images, particularly in some sulci and gyri (Fig 2B). Initial qualitative assessments by the neurologist suggest that subtraction maps can capture new lesions and changes in MS lesions.Discussion
In this study, we present a longitudinal subtraction map for ULF scans that can capture changes in MS lesions and help guide the clinician in identifying interval changes in MS. Nevertheless, further efforts are imperative in normalizing and harmonizing ULF data, especially when considering variability across different FLAIR versions due to scanner updates. Ongoing work is focused on improving registration and exploring normalization techniques, such as white stripe normalization3, to better harmonize serial scans and reduce false positives. Future work will also quantiatively compare ULF subtraction maps and their 3T counterparts to elucidate the pipeline's capacity to discern longitudinal changes in reference to clinical MRI standards, thus enhancing our understanding of the clinical utility of ULF MRI in the context of longitudinal MS monitoring.Acknowledgements
No acknowledgement found.References
1. Arnold TC, Freeman CW, Litt B, Stein JM. Low-field MRI: Clinical promise and challenges. J Magn Reson Imaging. Jan 2023;57(1):25-44. doi:10.1002/jmri.28408
2. Wattjes MP, Ciccarelli O, Reich DS, et al. 2021 MAGNIMS-CMSC-NAIMS consensus recommendations on the use of MRI in patients with multiple sclerosis. Lancet Neurology. Aug 2021;20(8):653-670. doi:10.1016/S1474-4422(21)00095-8
3. Shinohara RT, Sweeney EM, Goldsmith J, et al. Statistical normalization techniques for magnetic resonance imaging. Neuroimage-Clin. 2014;6:9-19. doi:10.1016/j.nicl.2014.08.008
4. Arnold TC, Tu D, Okar SV, et al. Sensitivity of portable low-field magnetic resonance imaging for multiple sclerosis lesions. Neuroimage Clin. 2022;35:103101. doi:10.1016/j.nicl.2022.103101
5. Hoopes A, Mora JS, Dalca AV, Fischl B, Hoffmann M. SynthStrip: skull-stripping for any brain image. Neuroimage. Oct 15 2022;260:119474. doi:10.1016/j.neuroimage.2022.119474
6. Avants BB, Tustison NJ, Song G, Cook PA, Klein A, Gee JC. A reproducible evaluation of ANTs similarity metric performance in brain image registration. Neuroimage. Feb 1 2011;54(3):2033-44. doi:10.1016/j.neuroimage.2010.09.025
7. Tustison NJ, Avants BB, Cook PA, et al. N4ITK: Improved N3 Bias Correction. Ieee T Med Imaging. Jun 2010;29(6):1310-1320. doi:10.1109/Tmi.2010.2046908
Figures