2955
Central Vein Sign and Trigeminal Lesions of Multiple Sclerosis Visualized by 7.0T MRI1Beijing Tiantan Hospital, Beijing, China, 2Tianjin General Hospital, Tianjin, China, 3MR research collaboration team, siemens healthineers, Beijing, China, 4Department of Neurology, University of California San Fransisco, San Francisco, CA, United States
Synopsis
Keywords: Multiple Sclerosis, Multiple Sclerosis
Motivation: Multiple sclerosis patients are more vulnerable to trigeminal neuralgia, but the mechanism behind this nerve injury is still unclear.
Goal(s): We aim to investigate trigeminal nerve involvement in MS and provide insight into pathology.
Approach: 120 patients underwent 7.0 T multi-modality MRI scans. T1-MPRAGE, T2-FLAIR, FLAWS-MP2RAGE, and T2*W images were collected.
Results: Our study confirmed the high prevalence of trigeminal nerve on 7.0 T MRI and highlighted the presence of a central vein sign in trigeminal nerve lesions. This study contributes to a deeper understanding of the pathophysiology and location-specific nature of trigeminal lesions.
Impact: This finding reinforces that trigeminal nerve involvement represents a characteristic of MS lesions, which has the potential for precising diagnosis in the future.
Introduction
Cranial nerve involvement is a prominent characteristic of multiple sclerosis (MS) lesions, with the optic nerve being the most frequently affected, followed by the trigeminal nerve. The prevalence of trigeminal involvement varies widely, ranging from 2.9% to 23%, depending on MRI resolution and sequence selection but also disease duration1-8. Additionally, MS patients have a 15-fold increased risk of developing trigeminal neuralgia (TN) in the general neurological outpatient population9. The mechanism behind the susceptibility of trigeminal nerve is still unclear.Method
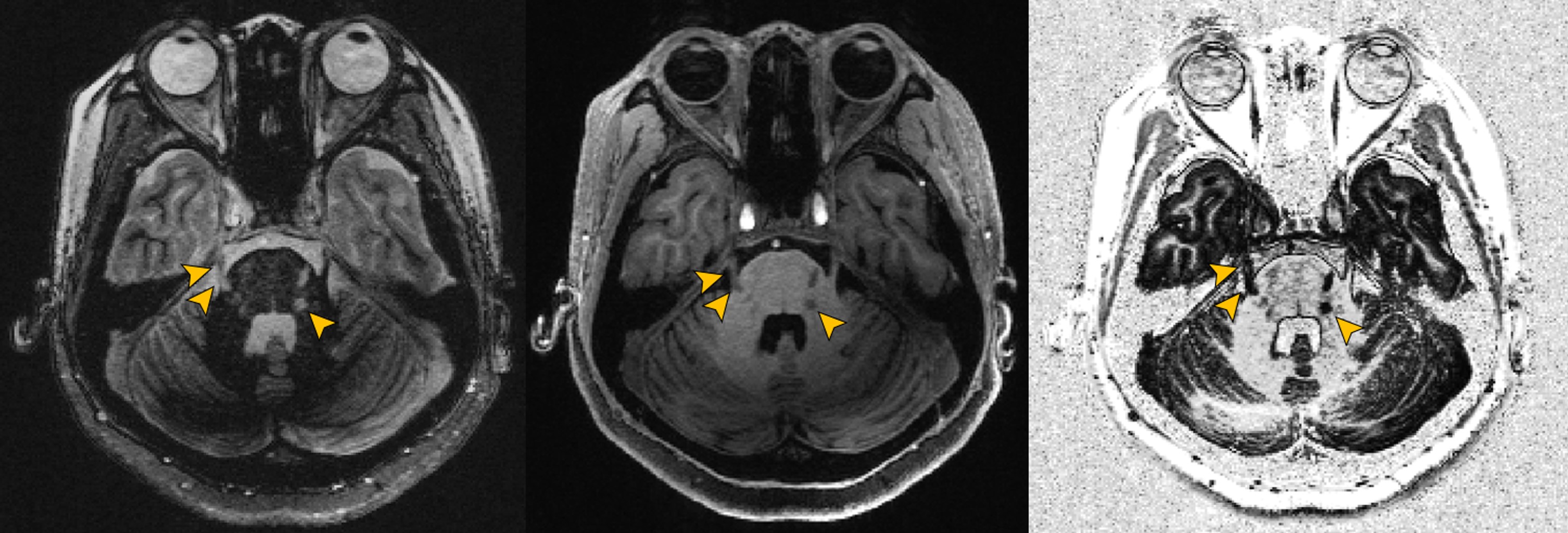
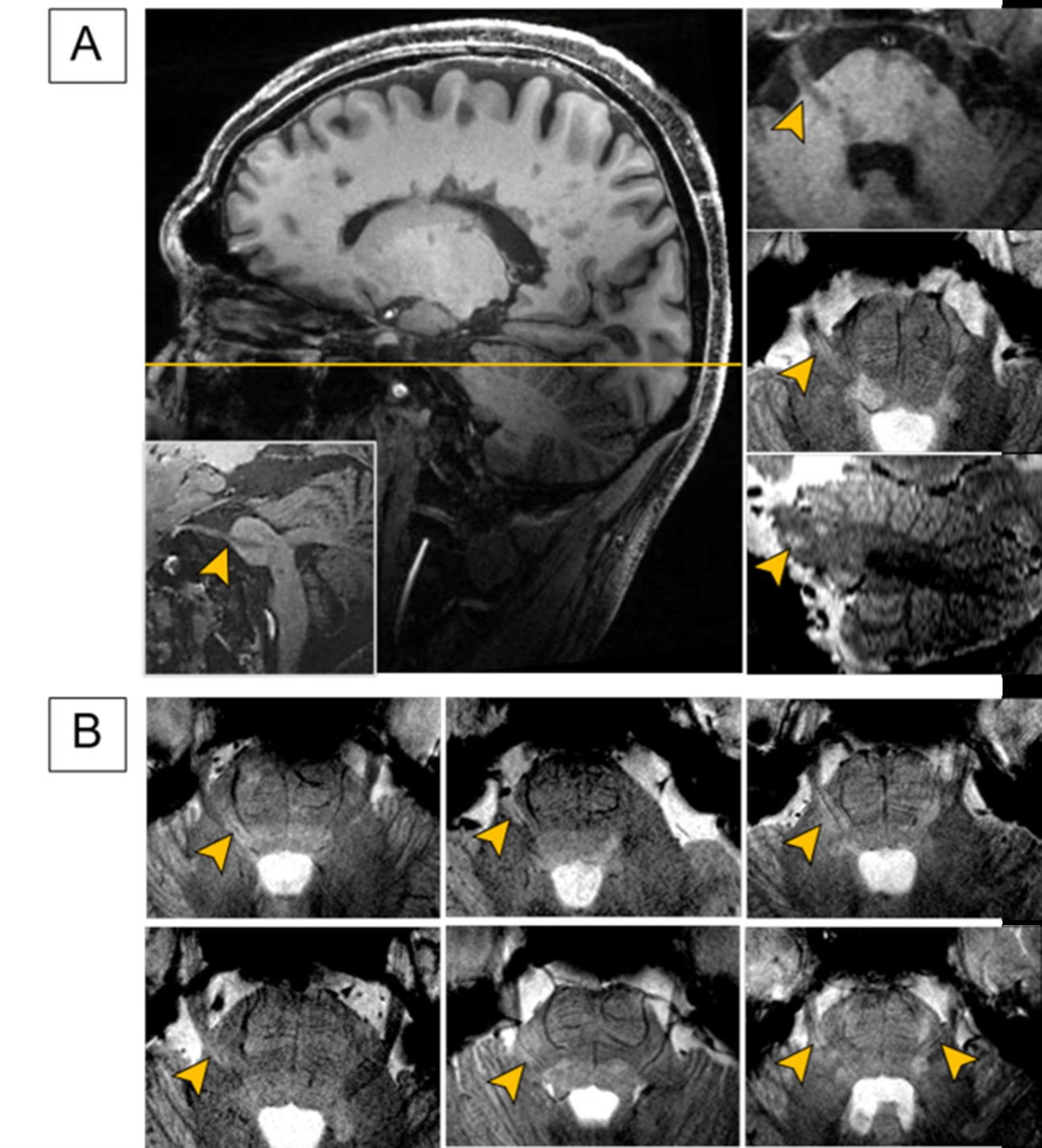
This observational cohort originates from an ongoing China National Registry of Neuro-Inflammatory Diseases (CNRID). Inclusion criteria were the following: age 18 years or older, diagnosis of MS according to the 2017 McDonald criteria, and no clinical relapse within the preceding 3 months. Every participant underwent 7.0 T scanner (MAGNETOM Terra, Siemens Healthcare, Erlangen, Germany), with a 32-channel head coil at Beijing Tiantan Hospital. T1 magnetization-prepared rapid acquisition gradient echo (T1-MPRAGE), T2 fluid-attenuated inversion recovery (T2-FLAIR) and FLuid And White matter Suppression (FLAWS) based on the magnetization-prepared with two rapid gradient echoes (MP2RAGE) sequence (FLAWS-MP2RAGE) were used to identify lesions. T2*W was used to identify central vein sign (CVS) within the trigeminal lesions. The affected area of the trigeminal nerve was divided into three parts: the cisternal segment, root entry zone (REZ), and nuclear zone, based on anatomical and signal abnormalities (Figure 1). The cisternal segment begins where the trigeminal nerve enters the prepontine cistern, and the REZ measures approximately 2 mm long and located within approximately 5-7 mm from the surface of the pons.Result
20/120 (16.7%) patients had a total of 54 trigeminal lesions, of which 11/20 (55%) were bilateral. The linear lesions extended along the trigeminal nerve, from the cisternal segment (16.7%, 9/54) and root entry zone (48.1%, 26/54), to the pontine-medullary nucleus (35.2%, 19/54). 26.9% (7/26) the lesions in root entry zone showed a typical CVS.Discussion
In this pioneering 7T-MRI consecutive cohort of patients with early MS in China, we observed a notable proportion of trigeminal involvement, with 16.7% of patients exhibiting such lesions with most of these lesions being clinically silent. Moreover, a CVS was detected in 26.9% lesions of root entry zone (REZ).The previous research claimed that prevalence of trigeminal nerve involvement in MS varies from 2.9% to 23%, which could be due to differences in selection bias in various cohorts, and MRI resolution. More importantly, most cohorts studying the prevalence of trigeminal involvement primarily focused on a history of MS-related TN, which introduced potential bias.2, 6, 7 Indeed, some patients with trigeminal nerve lesions may not manifest symptoms until several years after the lesion is detected on MRI, consistent with our finding that some patients had trigeminal nerve lesions without having TN.6
Conclusion
In this 7.0 T MRI cohort, the prevalence of trigeminal nerve involvement was 16.7%. Characteristic CVS was detected in 26.9% of lesions in the root entry zone. Our results suggest a unique mechanism of trigeminal nerve involvement in MS, which could provide more diagnostic information in clinics.Acknowledgements
No acknowledgement found.References
1. Mills RJ, Young CA, Smith ET. Central trigeminal involvement in multiple sclerosis using high-resolution MRI at 3 T. Br J Radiol. 2010;83(990):493-8.
2. Truini A, Prosperini L, Calistri V, Fiorelli M, Pozzilli C, Millefiorini E, et al. A dual concurrent mechanism explains trigeminal neuralgia in patients with multiple sclerosis. Neurology. 2016;86(22):2094-9.
3. van der Meijs AH, Tan IL, Barkhof F. Incidence of enhancement of the trigeminal nerve on MRI in patients with multiple sclerosis. Multiple sclerosis. 2002;8(1):64-7.
4. Nakashima I, Fujihara K, Kimpara T, Okita N, Takase S, Itoyama Y. Linear pontine trigeminal root lesions in multiple sclerosis: clinical and magnetic resonance imaging studies in 5 cases. Archives of neurology. 2001;58(1):101-4.
5. Swinnen C, Lunskens S, Deryck O, Casselman J, Vanopdenbosch L. MRI characteristics of trigeminal nerve involvement in patients with multiple sclerosis. Multiple sclerosis and related disorders. 2013;2(3):200-3.
6. Dilwali S, Mark I, Waubant E. MRI lesions can often precede trigeminal neuralgia symptoms by years in multiple sclerosis. Journal of neurology, neurosurgery, and psychiatry. 2023;94(3):189-92.
7. da Silva CJ, da Rocha AJ, Mendes MF, Maia AC, Jr., Braga FT, Tilbery CP. Trigeminal involvement in multiple sclerosis: magnetic resonance imaging findings with clinical correlation in a series of patients. Multiple sclerosis. 2005;11(3):282-5.
8. Sugiyama A, Mori M, Masuda H, Uchida T, Muto M, Uzawa A, et al. Trigeminal root entry zone involvement in neuromyelitis optica and multiple sclerosis. Journal of the neurological sciences. 2015;355(1-2):147-9.
9. Laakso SM, Hekali O, Kurdo G, Martola J, Sairanen T, Atula S. Trigeminal neuralgia in multiple sclerosis: Prevalence and association with demyelination. Acta neurologica Scandinavica. 2020;142(2):139-44.
Figures