2952
Reduced Brain Oxygen Metabolism in Patients with Multiple Sclerosis Measured by Venous Blood Quantitative Susceptibility Mapping1Neurology, Wayne State University School of Medicine, Detroit, MI, United States, 2Radiology, New York University School of Medicine, New York, NY, United States, 3Radiology, Wayne State University School of Medicine, Detroit, MI, United States
Synopsis
Keywords: Multiple Sclerosis, Multiple Sclerosis, Oxygenation; Quantitative Susceptibility Mapping; Neurodegeneration
Motivation: It remains largely unknown whether venous blood susceptibility can be used as an imaging biomarker of neuronal activity in multiple sclerosis (MS).
Goal(s): To assess the oxygen saturation of the internal cerebral veins (ICVs), and their correlations with clinical scores in MS patients.
Approach: Susceptibility of ICVs was measured on QSM data in 18 MS patients and 10 controls. The susceptibility of ICV values were correlated with clinical scores using linear regression in MS patient.
Results: There was a significant reduction in ICV susceptibility (indicating an increased oxygen saturation) in MS patients. The decreased venous susceptibility correlated with cognitive decline in these patients.
Impact: This study provides first-of-its-kind evidence that reduced oxygen consumption in deep cerebral regions may be associated with cognitive decline in patients with multiple sclerosis (MS). Venous blood susceptibility could be an imaging biomarker of cerebral oxygen metabolism in MS.
Introduction
Multiple sclerosis (MS) is a common neurodegenerative disease characterized by multifocal inflammatory and demyelinating lesions in the central nervous system1. Increased level of nitric oxide (NO) radicals was found in inflammatory lesions in MS2, 3. The elevated NO level exerts its neurotoxic effect at several levels, including inhibition of mitochondrial oxygen consumption, disruption of the blood brain barrier, delay in axonal conduction, and overall interference with neuronal metabolism and immune response4, 5. Indeed, several studies have shown reduced brain oxygen metabolism in individuals with MS6-10. Among various techniques measuring cerebral oxygen saturation in vivo, quantitative susceptibility mapping (QSM) derived from MRI phase data is able to directly measure venous blood oxygen saturation associated with deoxyhemoglobin levels11, 12. However, it remains largely unknown whether venous blood susceptibility can be used as an imaging biomarker of neuronal activity in MS. The objective of this study was to investigate the susceptibility of internal cerebral veins (ICVs) in patients with relapsing-remitting MS (RRMS), and their underlying correlations with clinical measures.Methods
Patients with RRMS and age-matched healthy controls (HC) were recruited as described13. The study was approved by the local institutional review board. Written consent forms were obtained prior to the study. Participants were scanned on a 3T MRI (Siemens Verio) using an interleaved rephased/dephased gradient echo sequence14 which generates MRAV (MR angiography and venography) and QSM data (Fig.1). The QSM data was reconstructed as described14 using the data of the fully flow-compensated echo of 12.5ms, which ensured an aliasing-free QSM for measuring venous susceptibility (Fig.1D). At relatively high echo times without flow compensation, the venous susceptibility sources can be confounded by the local phase aliasing, as illustrated in Fig.2. We performed clinical measures in MS patients including disease duration, Expanded Disability Status Scale (EDSS) for disease severity15; timed 25-foot walk (T25-FW) for lower extremity function16; 9-Hole Peg Test (9-HPT) for upper extremity function17; and Paced Auditory Serial Addition Test (PASAT) for cognitive function18. The total lesion load (mm3) of white matter hyperintensity lesions was measured on clinical MRI data as described13.Two raters independently traced the ICVs using a semi-automated region-growing tool on the maximum intensity projection (MIP) of 8 slices of the QSM data. The data was blinded to the raters. To minimize the partial volume effect (PVE), the region-of-interest (ROI) was placed at the middle segment of the ICVs between the thalamostriate veins and medial atrial veins (Fig.1D). The median susceptibility value of the ROI (χicv) was compared using Wilcoxon rank sum test between cohorts. Inter-rater reliability of χicv was assessed by the intraclass correlation coefficient (ICC) analysis19 and linear regression. Linear regression was used to correlate χicv with clinical scores in MS patients. Multiple comparison corrections were performed using the Bonferroni-Holm model20. P<0.05 was considered statistically significant.
Results
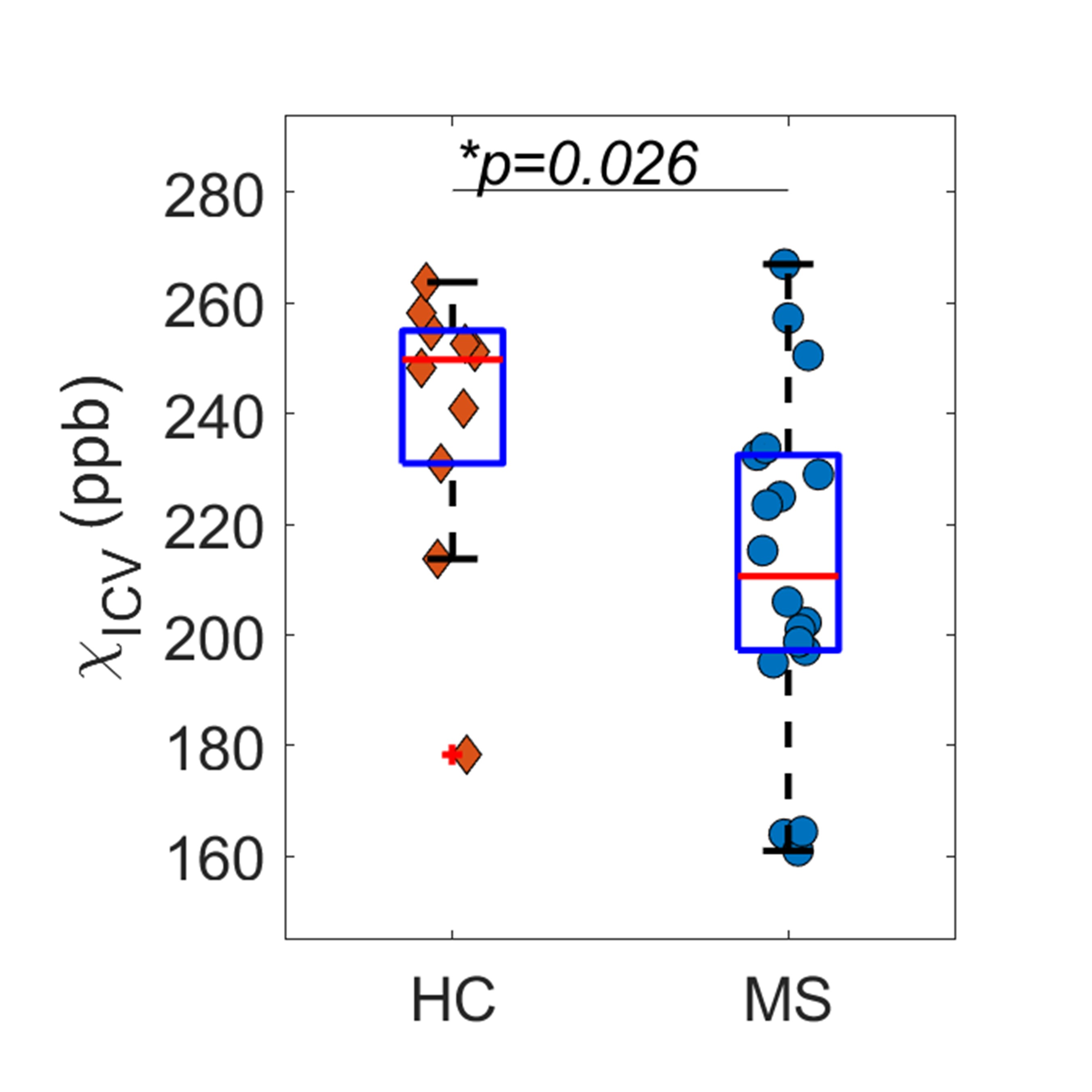
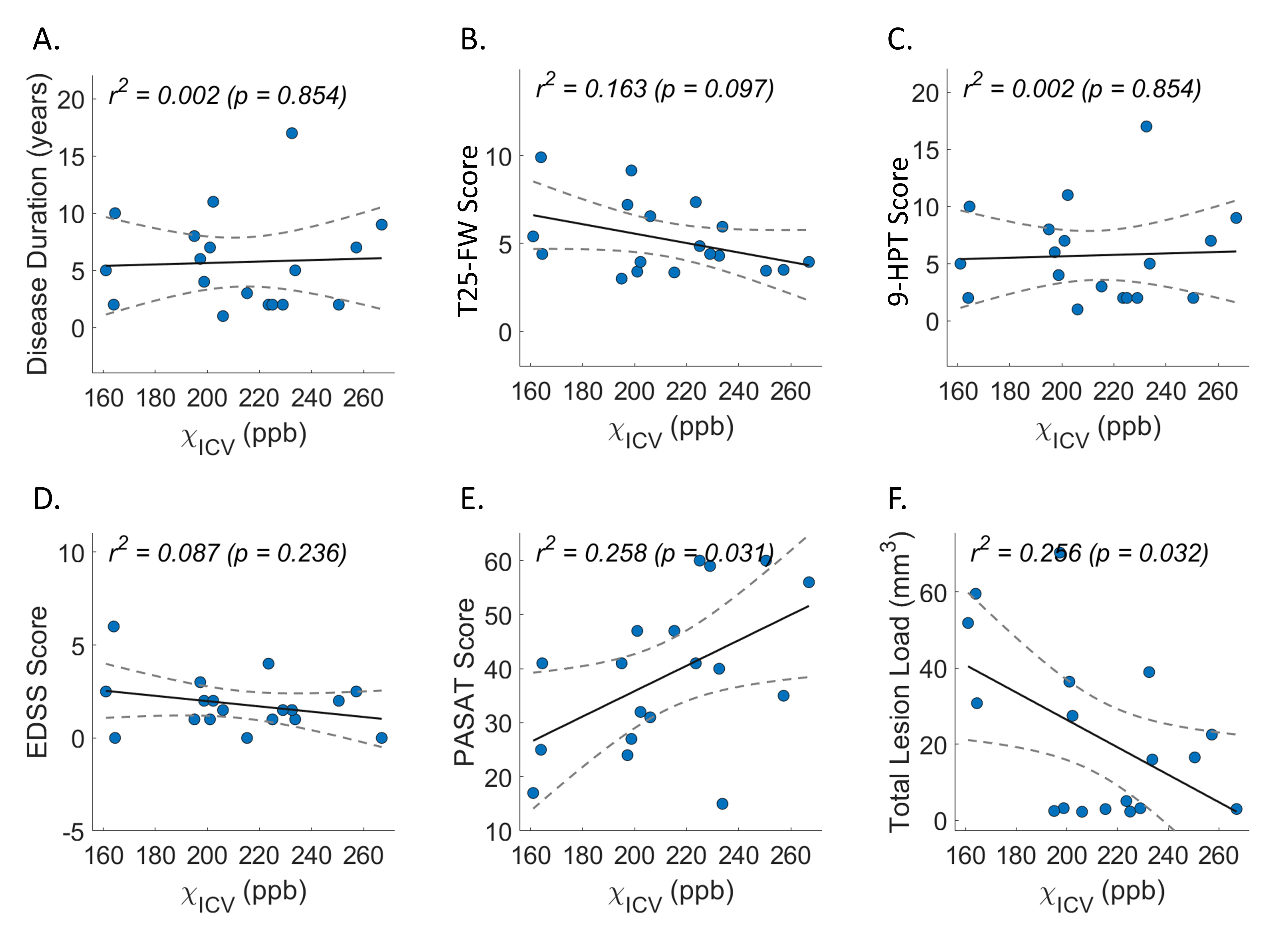
We studied 18 patients with RRMS and 10 age-matched HCs (Fig.3). The inter-rater reliability of χicv was excellent (ICC=0.97, p<0.001 and r2=0.97, p<0.001). There were significantly reduced χicv in RRMS patients (212.4±30.1ppb) compared to HCs (239.4±25.9ppb) as shown in Fig.4. The PASAT (r=0.258, p<0.031) and total lesion load (r=-0.256, p<0.032) were moderately correlated with χicv in MS patients (Fig.5).Discussion and Conclusions
In this study, we observed a reduced susceptibility of ICVs in RRMS patients, indicating decreased deoxyhemoglobin levels in venous blood and, consequently, an increased venous oxygen saturation. This may be associated with reduced oxygen consumption in the deep cerebral regions that drain into the ICVs. These regions include the subcortical nuclei through the thalamostriate veins, the corpus callosum, deep medullary frontal white matter through the septal veins, and periventricular white matter regions through the subependymal veins21. These cerebral regions are highly associated with cognitive function and are the most common locations of MS lesions. The imaging findings are in line with metabolic hypoxia4, 5 in which oxygen may be available, but cells and tissues are unable to utilize it due to reduced neuronal activity. This explanation is further supported by the correlation between the increased venous oxygen saturation and the declined cognitive function as measured by PASAT score18. We also demonstrated the reliability of the method, although significant PVE was observed by the generally lower venous susceptibility compared to the theoretical value of 450 ppb.In summary, this study suggests that venous susceptibility may be an imaging biomarker of reduced neuronal activity and an indicator of cognitive decline in MS. This pilot study warrants a large-scale clinical study to further investigate the cerebral venous susceptibility using PVE-corrected QSM and reserving the superior sagittal sinuses, which are typically discarded during the QSM process22.
Acknowledgements
We thank the MR Core Research Facility at Wayne State University for the support of the data acquisition.References
[1] Grigoriadis N, Van Pesch V: A basic overview of multiple sclerosis immunopathology. European journal of neurology 2015, 22:3-13.
[2] Smith KJ, Lassmann H: The role of nitric oxide in multiple sclerosis. The Lancet Neurology 2002, 1:232-41.
[3] Encinas JM, Manganas L, Enikolopov G: Nitric oxide and multiple sclerosis. Current neurology and neuroscience reports 2005, 5:232-8.
[4] Moncada S, Erusalimsky JD: Does nitric oxide modulate mitochondrial energy generation and apoptosis? Nature Reviews Molecular Cell Biology 2002, 3:214-20.
[5] Aboul-Enein F, Lassmann H: Mitochondrial damage and histotoxic hypoxia: a pathway of tissue injury in inflammatory brain disease? Acta neuropathologica 2005, 109:49-55.
[6] Ge Y, Zohrabian VM, Osa EO, Xu J, Jaggi H, Herbert J, Haacke EM, Grossman RI: Diminished visibility of cerebral venous vasculature in multiple sclerosis by susceptibility‐weighted imaging at 3.0 Tesla. Journal of Magnetic Resonance Imaging: An Official Journal of the International Society for Magnetic Resonance in Medicine 2009, 29:1190-4.
[7] Ge Y, Zhang Z, Lu H, Tang L, Jaggi H, Herbert J, Babb JS, Rusinek H, Grossman RI: Characterizing brain oxygen metabolism in patients with multiple sclerosis with T2-relaxation-under-spin-tagging MRI. Journal of Cerebral Blood Flow & Metabolism 2012, 32:403-12.
[8] Chandler HL, Stickland RC, Patitucci E, Germuska M, Chiarelli AM, Foster C, Bhome-Dhaliwal S, Lancaster TM, Saxena N, Khot S: Reduced brain oxygen metabolism in patients with multiple sclerosis: Evidence from dual-calibrated functional MRI. Journal of Cerebral Blood Flow & Metabolism 2023, 43:115-28.
[9] Sun X, Tanaka M, Kondo S, Okamoto K, Hirai S: Clinical significance of reduced cerebral metabolism in multiple sclerosis: a combined PET and MRI study. Annals of nuclear medicine 1998, 12:89-94.
[10] Cho J, Nguyen TD, Huang W, Sweeney EM, Luo X, Kovanlikaya I, Zhang S, Gillen KM, Spincemaille P, Gupta A: Brain oxygen extraction fraction mapping in patients with multiple sclerosis. Journal of Cerebral Blood Flow & Metabolism 2022, 42:338-48.
[11] Haacke EM, Liu S, Buch S, Zheng W, Wu D, Ye Y: Quantitative susceptibility mapping: current status and future directions. Magnetic resonance imaging 2015, 33:1-25.
[12] Haacke E, Tang J, Neelavalli J, Cheng Y: Susceptibility mapping as a means to visualize veins and quantify oxygen saturation. Journal of Magnetic Resonance Imaging 2010, 32:663-76.
[13] Haacke EM, Bernitsas E, Subramanian K, Utriainen D, Palutla VK, Yerramsetty K, Kumar P, Sethi SK, Chen Y, Latif Z: A Comparison of Magnetic Resonance Imaging Methods to Assess Multiple Sclerosis Lesions: Implications for Patient Characterization and Clinical Trial Design. Diagnostics 2021, 12:77.
[14] Chen Y, Liu S, Buch S, Hu J, Kang Y, Haacke EM: An interleaved sequence for simultaneous magnetic resonance angiography (MRA), susceptibility weighted imaging (SWI) and quantitative susceptibility mapping (QSM). Magnetic resonance imaging 2018, 47:1-6.
[15] Meyer-Moock S, Feng Y-S, Maeurer M, Dippel F-W, Kohlmann T: Systematic literature review and validity evaluation of the Expanded Disability Status Scale (EDSS) and the Multiple Sclerosis Functional Composite (MSFC) in patients with multiple sclerosis. BMC neurology 2014, 14:1-10.
[16] Motl RW, Cohen JA, Benedict R, Phillips G, LaRocca N, Hudson LD, Rudick R, Consortium MSOA: Validity of the timed 25-foot walk as an ambulatory performance outcome measure for multiple sclerosis. Multiple Sclerosis Journal 2017, 23:704-10.
[17] Earhart GM, Cavanaugh JT, Ellis T, Ford MP, Foreman KB, Dibble L: The 9-hole PEG test of upper extremity function: average values, test-retest reliability, and factors contributing to performance in people with Parkinson disease. Journal of Neurologic Physical Therapy 2011, 35:157-63.
[18] Tombaugh TN: A comprehensive review of the paced auditory serial addition test (PASAT). Archives of clinical neuropsychology 2006, 21:53-76.
[19] Shrout PE, Fleiss JL: Intraclass correlations: uses in assessing rater reliability. Psychological bulletin 1979, 86:420.
[20] Holm S: A simple sequentially rejective multiple test procedure. Scandinavian journal of statistics 1979:65-70.
[21] Wang J, Wang J, Sun J, Gong X: Evaluation of the anatomy and variants of internal cerebral veins with phase-sensitive MR imaging. Surgical and radiologic anatomy 2010, 32:669-74.
[22] Buch S, Chen Y, Haacke EM: Susceptibility mapping of the dural sinuses and other superficial veins in the brain. Magnetic resonance imaging 2019, 57:19-27.
Figures
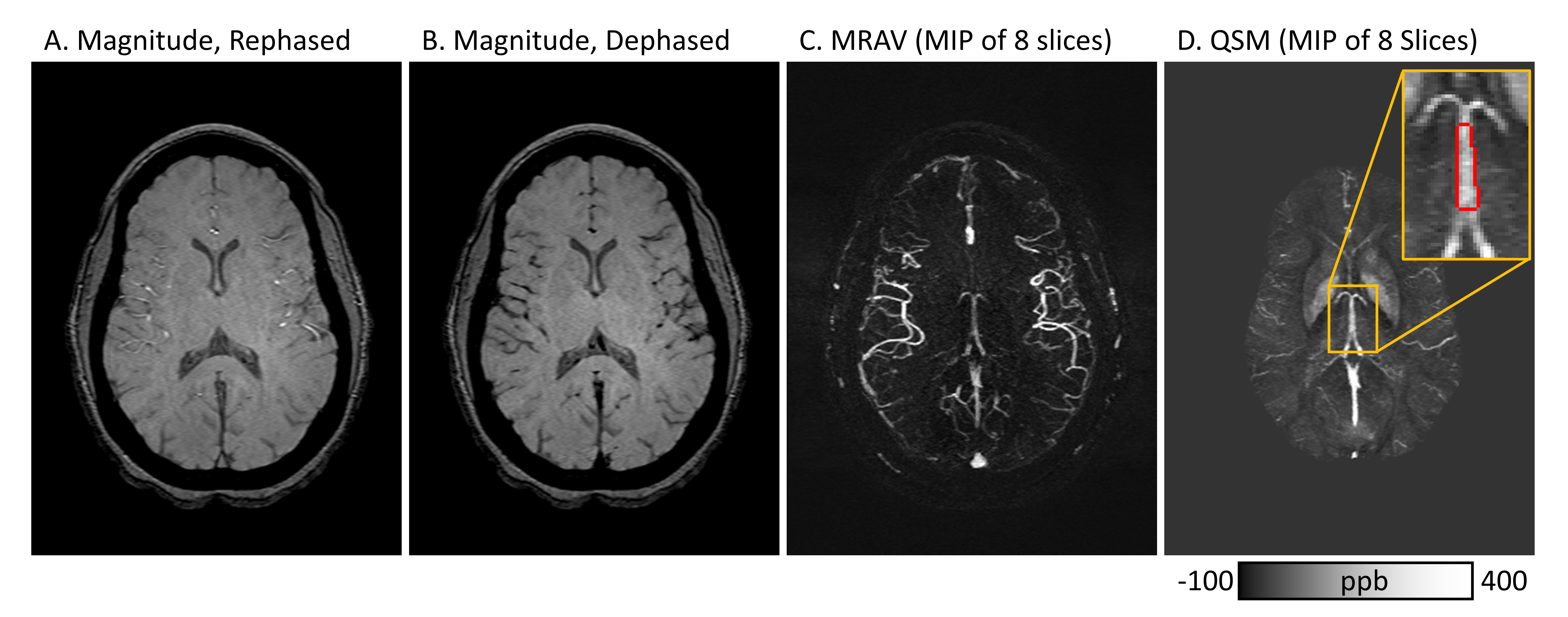
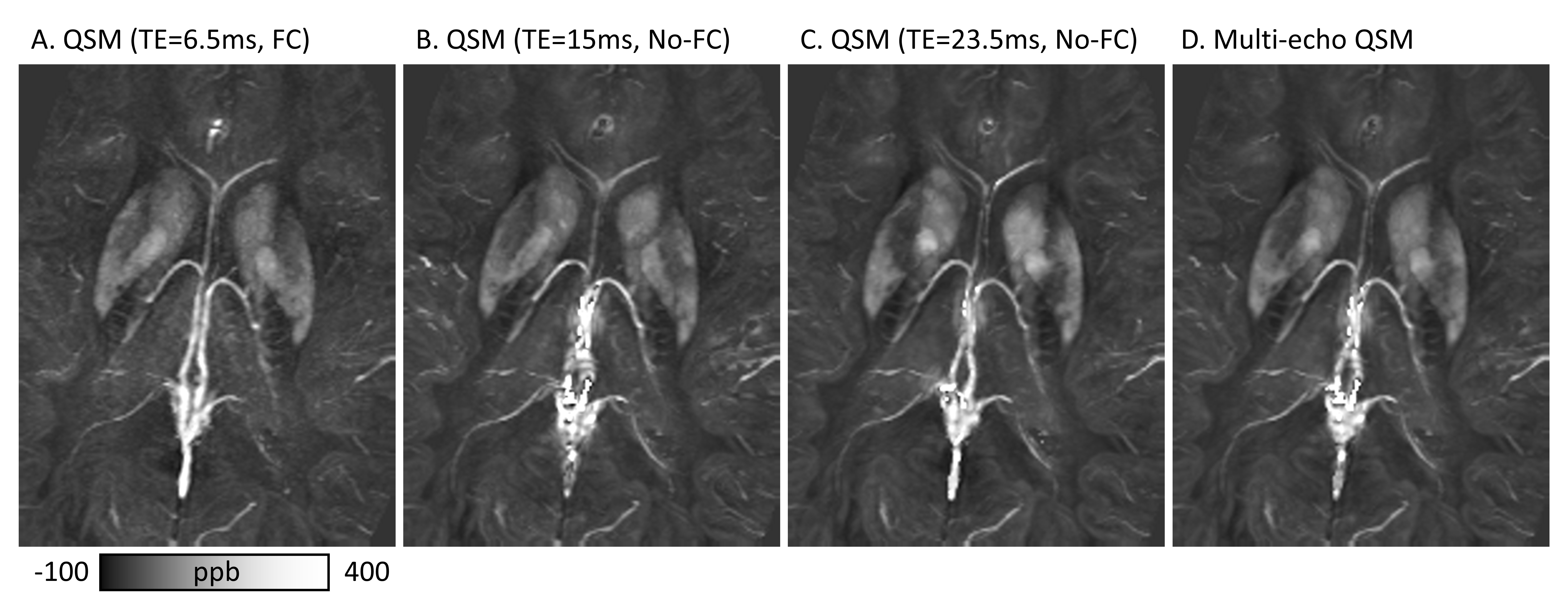
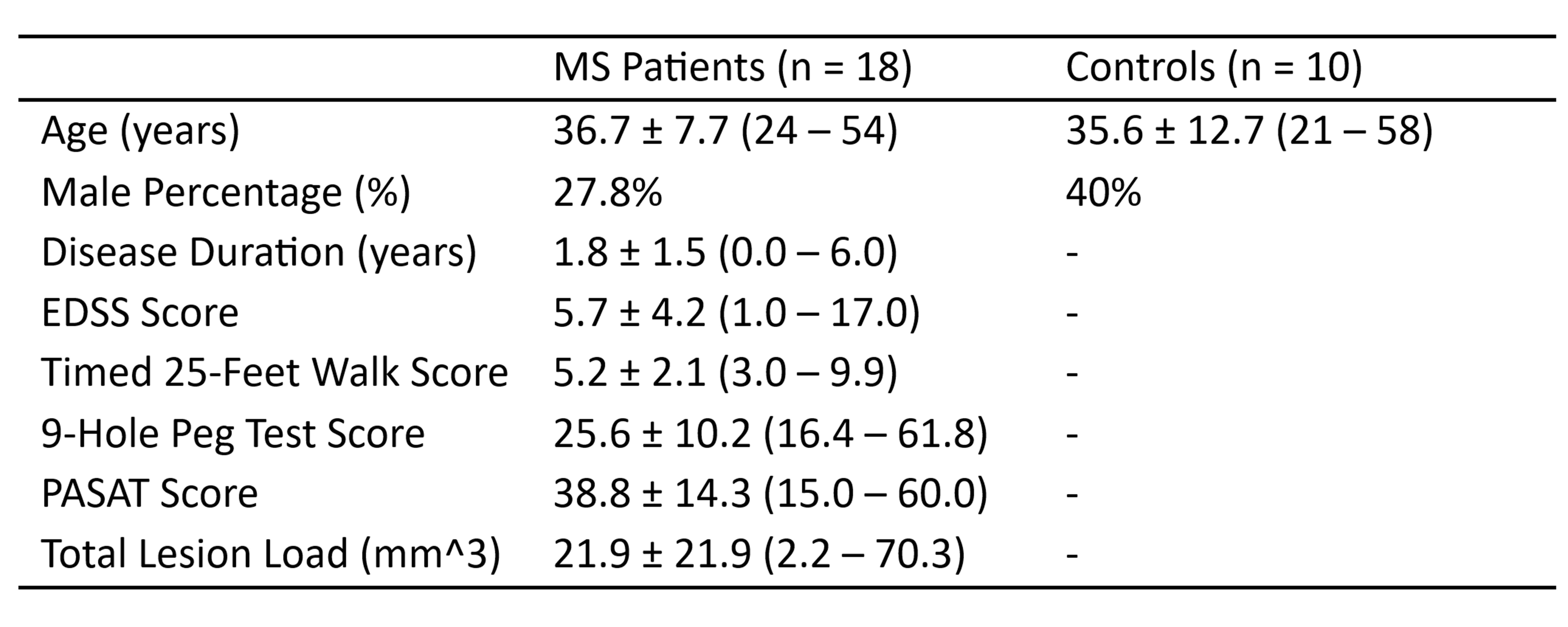
Figure 3. Demographics and clinical scores.