2951
Differences in local functional connectivity strength in patients with early and late multiple sclerosis1The Cleveland Clinic, Cleveland, OH, United States
Synopsis
Keywords: Multiple Sclerosis, Multiple Sclerosis
Motivation: Disease progression is variable in multiple sclerosis (MS). Widely-used measures of neuropathology do not show a straightforward relationship to functional decline.
Goal(s): Our work aims to identify changes in brain function that are related to MS disease progression.
Approach: We measured resting state functional connectivity MRI at 7 tesla in 71 adults with MS. We compared cortical grey matter regional homogeneity (ReHo) in participants with early and late stage MS and correlated ReHo with MS disease severity.
Results: Local connectivity, measured by ReHo, was stronger in early MS and was related to disease severity.
Impact: MRI-based measures that track and predict MS disease progression could identify patients who subsequently decline and serve as outcome measures in clinical trials of novel disease modifying treatments.
Introduction
In people diagnosed with multiple sclerosis (MS), disease progression can occur at all disease stages and regardless of disease course. Although MRI is critical to the diagnosis and monitoring of MS, conventional measures such as lesion burden are not strongly related to clinical impairment and are only partial predictors of disease progression. A measure that strongly relates to clinical measures of disability and predicts disease progression would be valuable for disease monitoring and as an outcome measure in clinical trials of novel treatments. Here, we use high resolution MRI at 7 tesla to assess the relationship of between MS-related disability and regional homogeneity1 (ReHo) of functional connectivity in cortical grey matter.Methods
Seventy-one participants with MS (mean age: 52.0 ± 8.2; 16 males; median Expanded Disability Status Scale (EDSS): 3.5, range 1.5-7) were enrolled in an IRB-approved protocol. Six participants were classified as early MS (EMS; time from diagnosis ≤ 5 years, EDSS ≤ 4.5) and 20 were classified as late MS (LMS; time from diagnosis > 5 years, EDSS ≥ 5). Measures of disease severity included EDSS and the Multiple Sclerosis Functional Composite (MSFC).A whole-brain T1-weighted MP2RAGE sequence (0.75mm isotropic voxel size) and a rsfMRI scan were acquired on a Siemens 7T Magnetom with a SC72 gradient (Siemens Medical Solutions, Erlangen) using a 1-Tx and 32-Rx channel head coil (Nova Medical). RsfMRI acquisition parameters were: 132 repetitions of 81 1.5mm thick axial slices acquired with TE/TR=21ms/2800ms, voxel size 0.75×0.75×1.5mm3, matrix 160×160, FOV 210mm×210mm, receive bandwidth = 1562 Hz/pixel. Subjects were instructed to keep their eyes closed during scans.
RsfMRI scans were corrected for motion and measured physiologic noise, detrended, and lowpass filtered.2,3 ReHo maps were calculated in all cortical grey matter voxels.1 For each participant, the T1-weighted MP2RAGE and cortical parcellation maps (Freesurfer 7.1; 2009 Destrieux atlas4) were coregistered and warped to rsfMRI space. The median ReHo value (neighborhood size 19) was calculated in each of 75 cortical regions (150 bilateral parcels). Parcels with ReHo values in less than 50 voxels were excluded from further analysis.
Unpaired t-tests were used to compare median ReHo values in each parcel between EMS and LMS participants. Results were corrected using the false discovery rate. For each significant parcel, median ReHo values were correlated with MSFC values and associated measures in the full sample.
Results
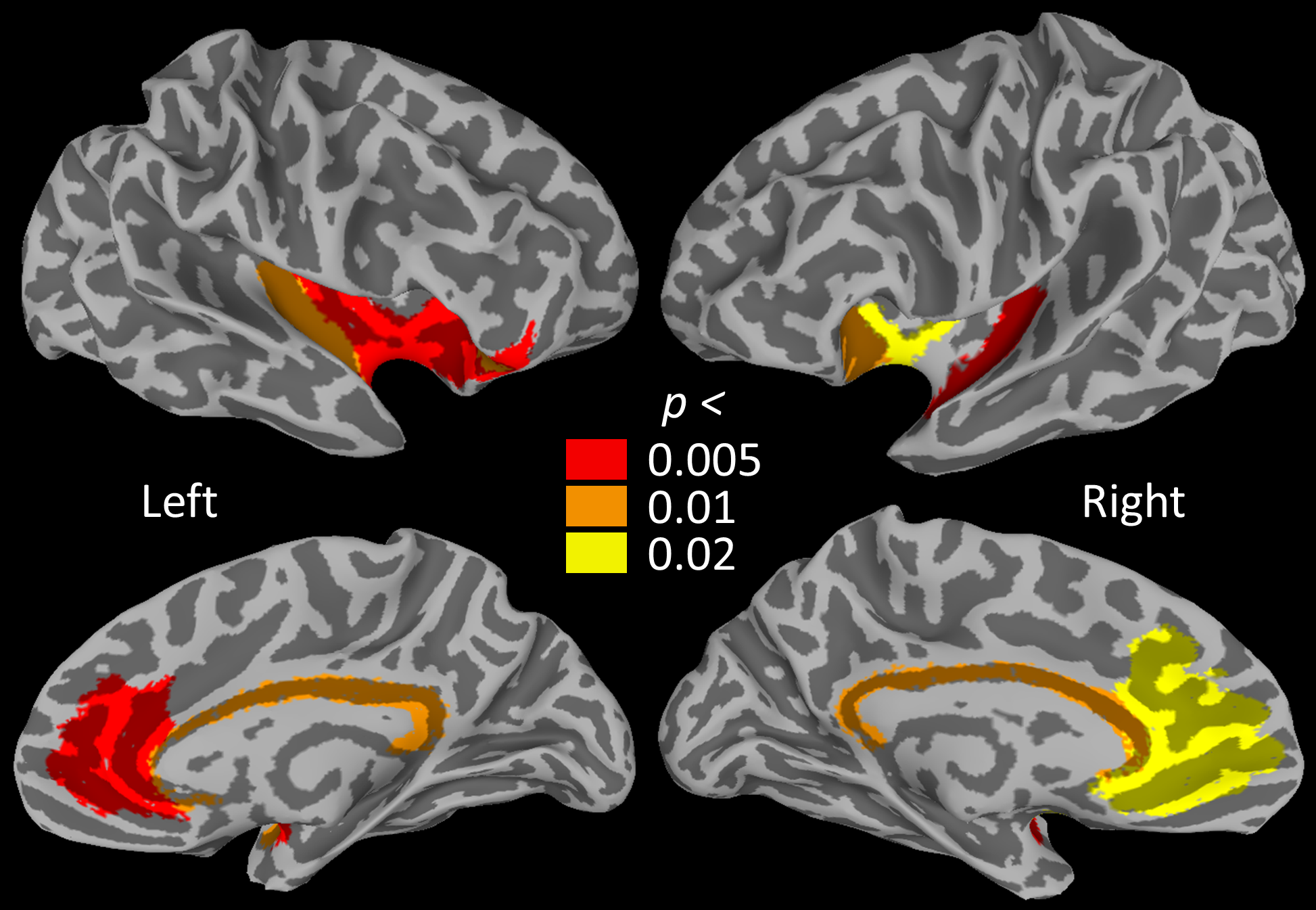
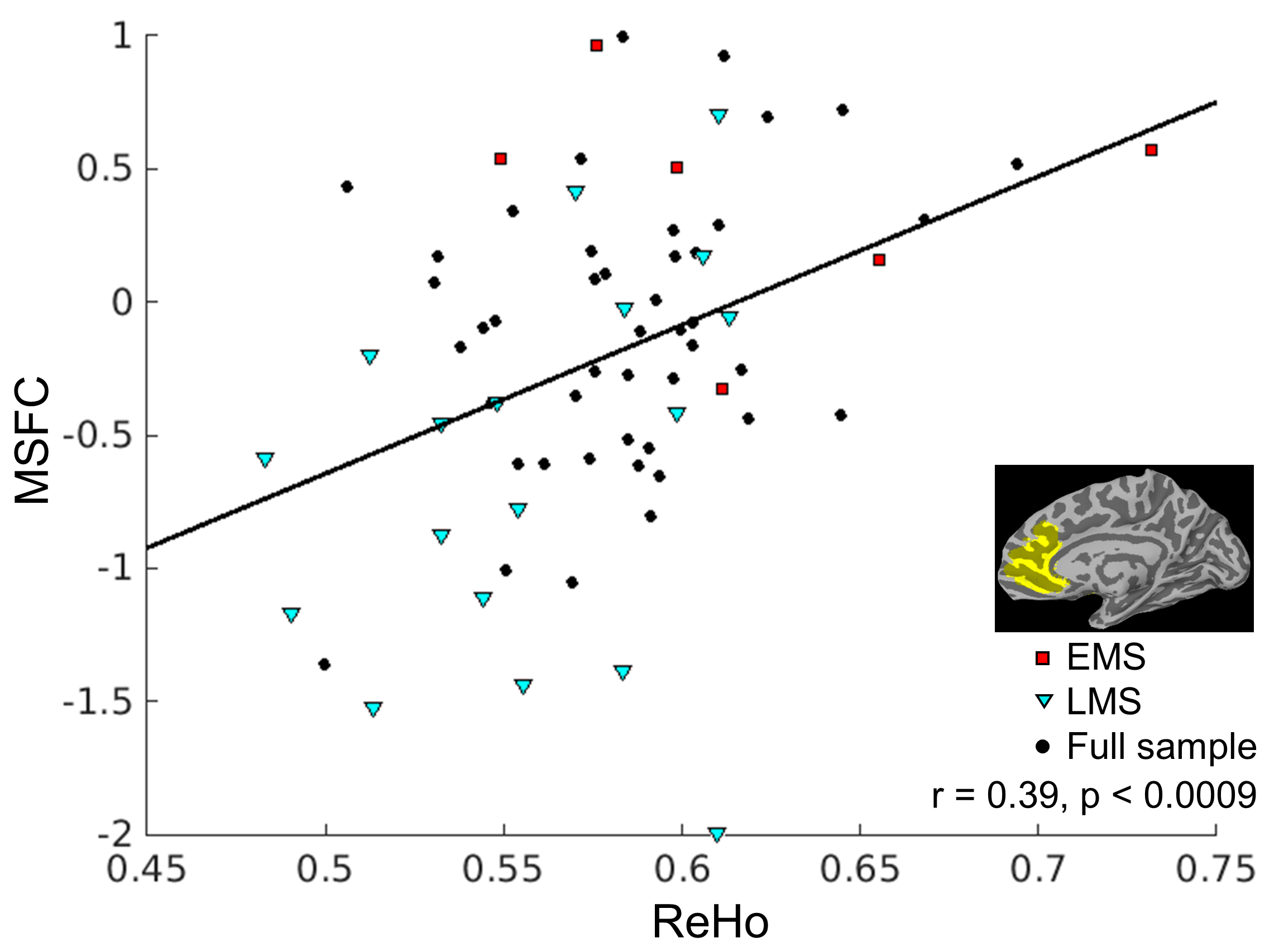
Figure 1 and Table 1 report cortical grey matter regions where ReHo was significantly lower in LMS compared to EMS. No regions showed higher ReHo in LMS. In the full sample, MSFC score was significantly related to ReHo in all regions except the left orbitalfrontal gyrus and horizontal ascending ramus of the lateral fissure (HALF; Table 1). Higher MSFC indicates lower disability. Figure 2 shows the relationship between MSFC and ReHo in the right anterior cingulate. Relationships between MSFC and ReHo measures were driven by the motor function components of the MSFC.| | Left | Right | ||||
| | EMS v LMS | MSFC (n=71) | EMS v LMS | MSFC (n=71) | ||
| | p | r | p | p | r | p |
| Anterior cingulate | 0.005 | 0.28 | 0.020 | 0.012 | 0.39 | 0.0009 |
| Pericallosal sulcus | 0.007 | 0.34 | 0.004 | 0.006 | 0.35 | 0.003 |
| Orbitofrontal gyrus | 0.002 | 0.17 | 0.162 | - | - | - |
| HALF | 0.005 | 0.19 | 0.117 | - | - | - |
| Insula: | | | | | | |
| Circular sulcus, anterior | 0.002 | 0.30 | 0.013 | 0.007 | 0.30 | 0.014 |
| Circular sulcus, inferior | 0.008 | 0.31 | 0.009 | 0.004 | 0.32 | 0.007 |
| Short gyri | 0.005 | 0.32 | 0.008 | 0.014 | 0.35 | 0.004 |
| Long gyrus/central sulcus | 0.002 | 0.33 | 0.005 | - | - | - |
Discussion
ReHo represents the homogeneity of the BOLD time series within a spatially constrained cluster. Our results agree with previous work showing that, in MS, local connectivity strength is weaker in those with higher levels of disability.5,6 The neuropathological basis of these changes is unclear, and could involve local grey matter damage or degeneration of associated white matter. Future work will assess the relationship of ReHo longitudinal clinical measures and specific domains of disability.Acknowledgements
This work was supported by the Department of Defense (MS150097). We thank Siemens Healthineers Tobias Kober for use of WIP944 and Thomas Benner for use of WIP770B.References
1. Zang Y, Jiang T, Lu Y et al. (2004) Regional homogeneity approach to fMRI data analysis. NeuroImage. 22(1): 394-400.
2. Beall EB and Lowe MJ. (2014) SimPACE: generating simulated motion corrupted BOLD data with synthetic-navigated acquisition for the development and evaluation of SLOMOCO: a new, highly effective slicewise motion correction. Neuroimage. 101:21-34.
3. Glover et al. (2000) Image-Based Method for Retrospective Correction of Physiological Motion Effects in fMRI: RETROICOR. Magnetic Resonance in Medicine. 44:162-67.
4. Destrieux C, Fischl F, Dale A et al. (2010) Automatic parcellation of human cortical gyri and sulci using standard anatomical nomenclature. NeuroImage. 53(1): 1:15.
5. Zhu Y, Huang M, Zhao Y et al. (2020) Local functional connectivity of patients with acute and remitting multiple sclerosis. Medicine. 99(43):e22860.
6. Dogonowski AM, Andersen KW, Madsen KH et al. (2013) Multiple sclerosis impairs regional functional connectivity in the cerebellum. Neuroimage Clin. 4:130-8.
Figures