2925
Decreased cortical thickness in obsessive compulsive disorder: a meta-analysis of brain structural magnetic resonance imaging studies.1Department of Radiology and Huaxi MR Research Center (HMRRC), West China Hospital of Sichuan University, Chengdu, China
Synopsis
Keywords: Gray Matter, Nervous system, obsessive compulsive disorder; structure MRI; whole brain
Motivation: Although studies indicate abnormalities in cingulo-opercular and default mode networks in obsessive-compulsive disorder (OCD), neuroimaging evidence of brain structural alterations is still limited and contradictory.
Goal(s): To compare cortical thickness (CTh) between patients with OCD and healthy controls.
Approach: We performed a meta-analysis on CTh and conducted subgroup analyses and meta-regression analyses to explore the effects of confounding factors on CTh.
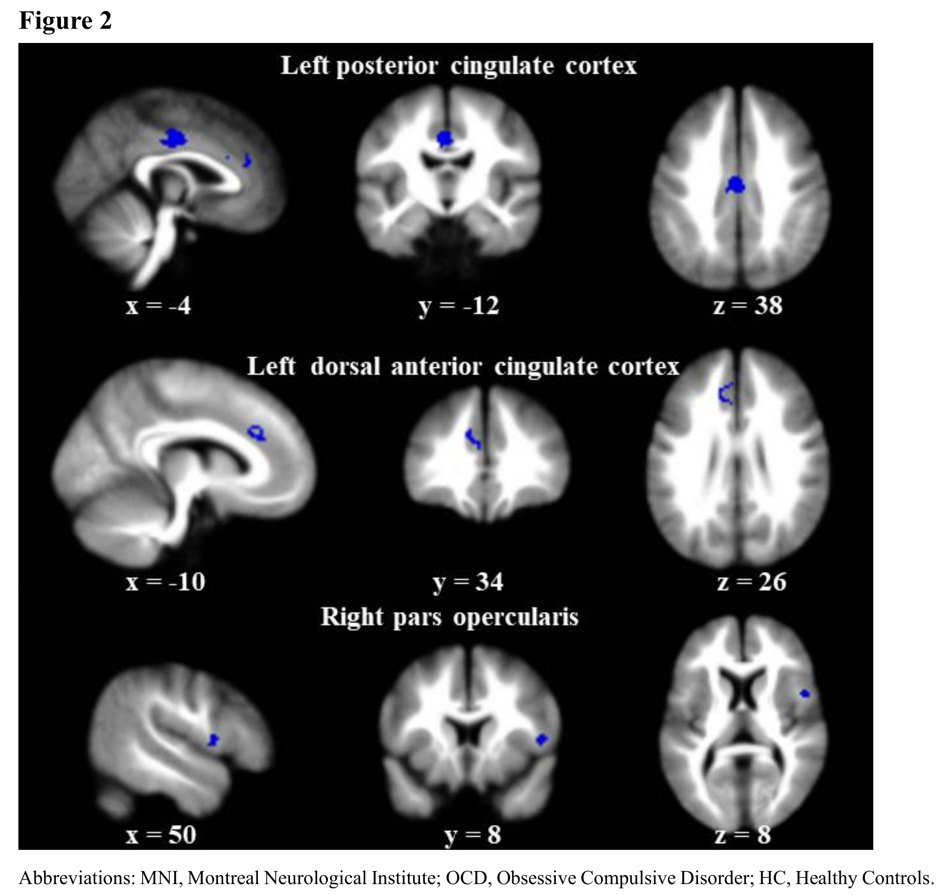
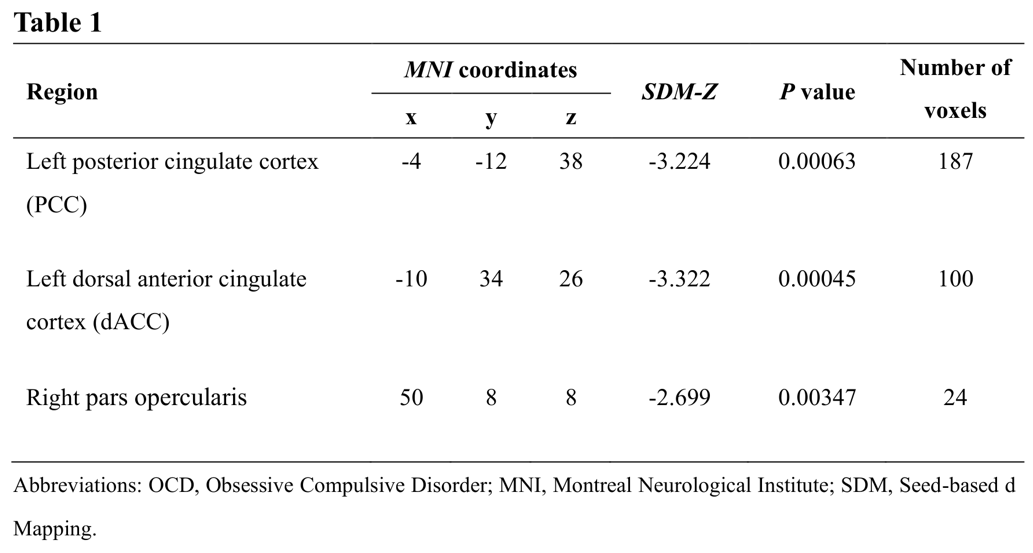
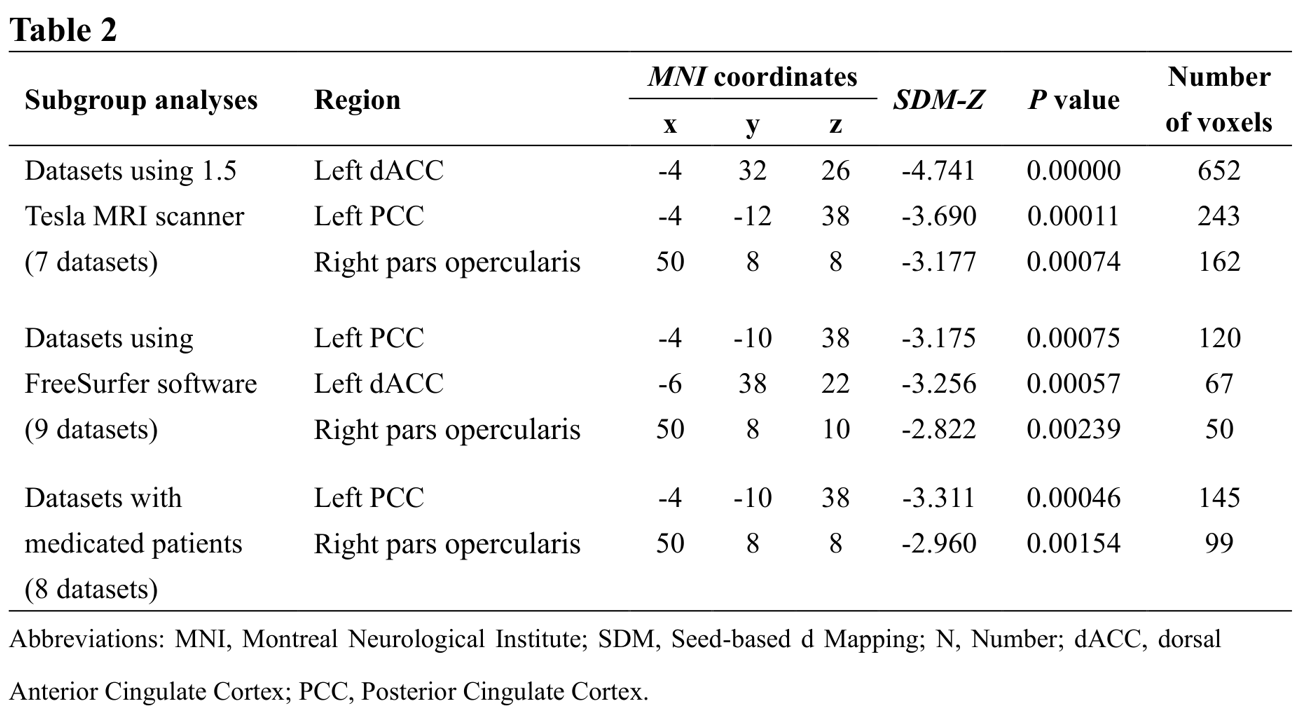
Results: Our study found decreased CTh in the left posterior cingulate cortex (PCC), left dorsal anterior cingulate cortex (dACC), and right pars opercularis in OCD. Medicated-subgroup analysis showed no between-group differences in dACC, though reduced CTh of PCC and pars opercularis remained.
Impact: Our study found decreased CTh in cingulo-opercular and default mode networks in patients with OCD, which helped explore the neural mechanism of OCD, and also suggested that medication might have an impact on CTh alterations in OCD.
Introduction
Obsessive compulsive disorder (OCD) is a chronic mental disorder with significant health burden. Despite its universality and disability, the neurobiological mechanisms are not fully understood. With the improvement of magnetic resonance imaging (MRI) technology and deeper understanding of brain, the abnormal brain structure of OCD has attracted researchers’ attention. Cortical thickness (CTh) is thought to be a heritable and relatively stable structural feature and representative characteristic in reflecting cellular structural abnormalities1. However, due to the small sample size and potential confounding factors, the results on CTh of OCD are inconsistent.Methods
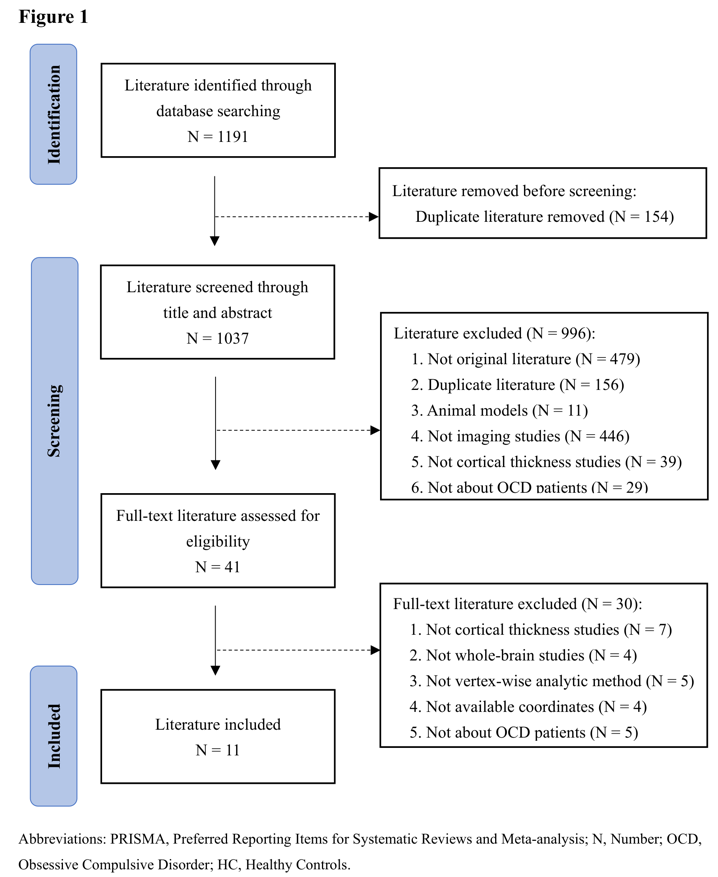
This meta-analysis followed PRISMA guidelines and was conducted using seed-based d mapping software (SDM). We searched in PubMed, Embase, Web of Science, and Science Direct from inception to July 1, 2023, and screened studies that compared the whole-brain CTh between OCD and healthy controls (HCs). For the meta-analyzing, SDM performed random-effects evaluation to create the mean map, merging the data from all involved studies. In addition, we conducted subgroup analyses (i.e. medication status, MRI scanner field strength, and CTh analyzing software) and meta-regression analyses (variables including patients’ sex ratio, age, age at symptom onset, and scores of Yale-Brown Obsessive Compulsive Scale [Y-BOCS]). Finally, we carried out jackknife sensitivity analyses, heterogeneity assessment, and publication bias.Results
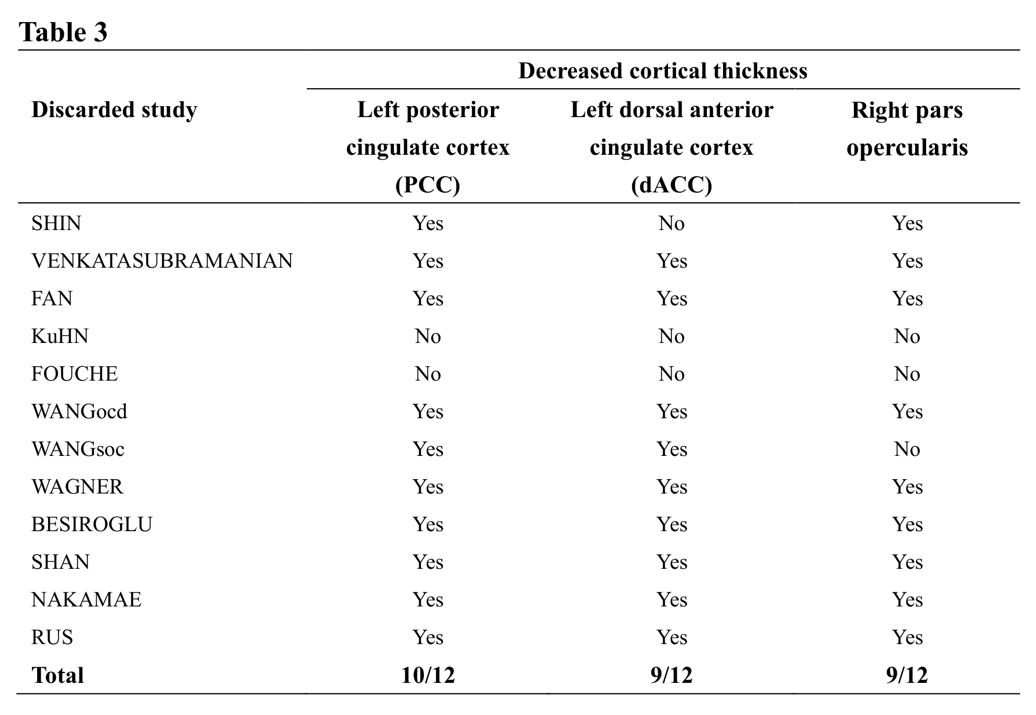
We included 11 articles, containing 12 datasets with 982 patients (mean age: 30.6; 51.9% women) and 843 HCs (mean age: 29.4; 49.7% female) (Figure 1). Compared to HCs, OCD group showed decreased CTh in the left posterior cingulate cortex (PCC) (Z= -3.224, P= 0.00063), left dorsal anterior cingulate cortex (dACC) (Z= -3.322, P= 0.00045), and right pars opercularis (Z= -2.699, P= 0.00347) (Figure 2, Table 1). For 7 datasets using 1.5 Tesla MRI scanner and 9 datasets using FreeSurfer, OCD group showed thinner CTh in the left PCC, left dACC, and right pars opercularis, consistent with the pooled meta-results. Subgroup analysis of 8 datasets with medicated patients only showed reduced CTh in the left PCC and right pars opercularis, but no between-group difference in the left dACC (Table 2). Neither patients’ sex ratio, mean age, age at onset, nor Y-BOCS score were significantly associated with CTh alterations.In the jackknife sensitivity analyses, decreased CTh in the left PCC remained statistically significant in 10/12 datasets, and in the left dACC and right pars opercularis preserved in 9/12 datasets (Table 3), confirming high replicability and reliability of this meta-analysis. In the pooled meta-analysis, none of regions with decreased CTh showed significant heterogeneity between studies (all I2= 0%). In the publication bias analyses, egger tests were not significant in the left PCC (P= 0.060) and right pars opercularis (P= 0.067), but significant in the left dACC (P= 0.006).
Discussion
Our results showed decreased CTh in the cingulo-opercular network (CON) and default mode network (DMN), underlying the neuroanatomical mechanism of OCD. In addition, we found that medicated status might affect the CTh alterations.Previous studies demonstrated that abnormal neural structure of patients with OCD gradually developed from prenatal to adulthood2. Our findings further supported the idea of neuroanatomical abnormalities in adult patients, reflecting a more stable and long-standing CTh reduction. Consistent with our results, studies focused on other structural characteristics also showed decreased gray matter volume3 and cortical surface area4 in cingulum. Located in CON, dACC and pars opercularis are involved in error processing and emotion regulation, and abnormal structure of which may result in compulsive behaviors accompanying feelings of distress. As an important region in DMN, PCC plays a role in thoughts and attention focus, and structural abnormalities may relate to the declines in thoughts transfer, then leading to obsessive thoughts. Therefore, neuroanatomical abnormalities in the PCC, dACC, and pars opercularis may account for the clinical symptoms and deficits in advanced cognitive function in OCD.
Regarding medication effect on brain structure, one study found different CTh alterations between medicated patients with OCD and unmedicated patients5, and similarly, we also found that medicated-subgroup results were not fully consistent with pooled results, suggesting medication might be a confounding factor for CTh analysis in OCD.
Egger test was significant in the left dACC. One possible explanation was that we only included published data and datasets were not much sufficient, which may result in some available data not being taken into account and concealing some publication bias.
Conclusion
In summary, our findings supported the importance of decreased CTh in the CON and DMN underlying the pathophysiology of OCD. In addition, we suggested controlling for confounding factors such as medication status, as well as expanding sample size to validate the CTh reduction in OCD in future.Acknowledgements
No acknowledgement found.References
1. Thompson PM, Hayashi KM, de Zubicaray G, Janke AL, Rose SE, Semple J, et al. Dynamics of gray matter loss in Alzheimer's disease. J Neurosci. 2003; 23(3): 994 - 1005.
2. Odile A. van den Heuvel, Guido van Wingen, Carles Soriano-Mas, et al. Brain circuitry of compulsivity. Eur Neuropsychopharmacol. 2016 May; 26(5): 810-27.
3. Joaquim Radua, Odile A. van den Heuvel, Simon Surguladze, et al. Meta-analytical comparison of voxel-based morphometry studies in obsessive-compulsive disorder vs other anxiety disorders. Arch Gen Psychiatry. 2010 Jul; 67(7): 701-11.
4. Ganesan Venkatasubramanian, Amit Zutshi, Sachin Jindal, et al. Comprehensive evaluation of cortical structure abnormalities in drug-naïve, adult patients with obsessive-compulsive disorder: A surface-based morphometry study. J Psychiatr Res. 2012 Sep; 46(9): 1161-8.
5. Willem B. Bruin, Luke Taylor, Rajat M. Thomas, et al. Structural neuroimaging biomarkers for obsessive-compulsive disorder in the ENIGMA-OCD consortium: medication matters. Transl Psychiatry. 2020 Oct 8; 10(1): 342.
Figures