2923
Brain Cortical Changes in Pediatric and Adolescent Patients with Intermittent Exotropia Basic Type: SBM Analysis on MRI Morphological Data1School of Medicine, Chinese University of Hong Kong(Shenzhen), Shenzhen, China, 2Siemens Healthineers (China), Shanghai, China, 3Shenzhen Research Institute of Big Data, Shenzhen, China, 4School of data science, Chinese University of Hong Kong(Shenzhen), Shenzhen, China, 5Department of Neurosurgery, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 6Department of Ophthalmology, Beijing Tongren Hospital, Beijing, China, 7Department of Radiology, Beijing Tongren Hospital, Beijing, China
Synopsis
Keywords: Gray Matter, Head & Neck/ENT, strabismus, ophthalmology, SBM
Motivation: Basic type of intermittent exotropia (IXT) is one of the most common strabismus subtypes in children and adolescents, yet a clear consensus of its etiology and treatment approach is still lacking.
Goal(s): To discover abnormal brain cortical structures related to this disease and explore the central nervous system mechanisms of IXT.
Approach: Basic type IXT patients and healthy volunteers were recruited, cortical structures extracted from their whole-brain MRI morphological data were compared using the SBM method.
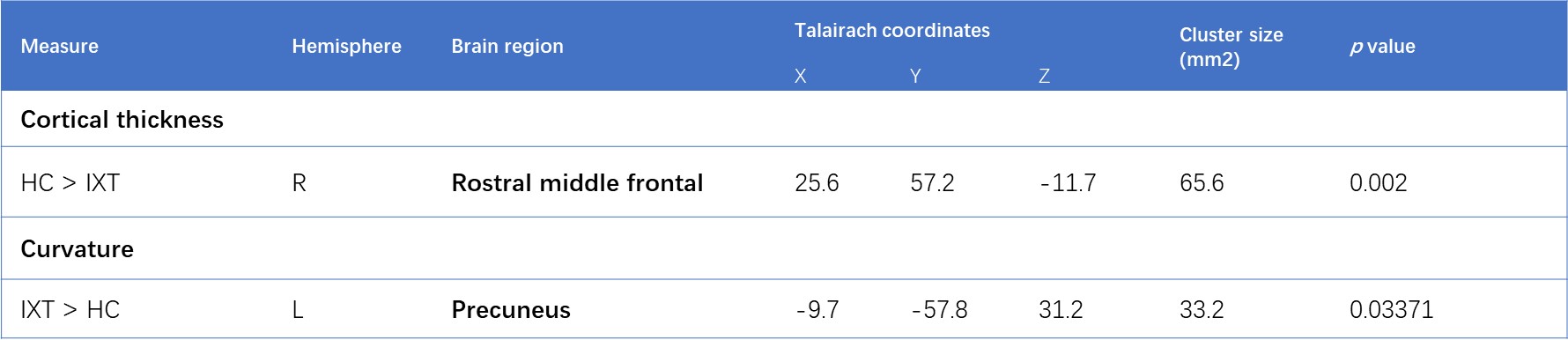
Results: Distinct differences of cortical thickness and curvature between the two groups were found, located in the right rostral middle frontal cortex and the left precuneus.
Impact: Our results suggesting that the primary pathological changes in this disease may differ from traditional perspectives. Based on these findings, we have proposed a new pathogenic hypothesis and introduced novel treatment recommendations.
Introduction
Intermittent exotropia(IXT)is one of the most common eye movement disorders in children and adolescents. Its main symptom is the involuntary outward movement of the eyes. Because the exact pathophysiology of IXT is not fully understood yet, and the outcome of common-used extraocular muscle surgery and no-surgery therapies are not satisfying[2], there’s still no consensus about how to treat those patients. Some recent studies have revealed several brain cortical structure changes in IXT patients. [3] [4] However, these studies lack screening for different subtypes of IXT. Therefore, this study enrolled only subjects with basic type of IXT for a more targeted investigation. SBM (Surface-based morphometry) is used to quantify and compare cerebral cortex features between IXT patients and HCs. Based on our findings, some new neuroimaging evidence for the etiology of basic-type IXT in children and adolescents were found and a new hypothesis regarding its pathogenesis is proposed.Materials and Methods
31 pediatric and adolescent patients diagnosed with basic type IXT (10.94 ± 1.69 years old), along with 37 age-matched (11.14 ± 2.06 years old) healthy controls (HCs) were enrolled.3D T1WI sequence (MPRAGE) was scanned for all subjects with a 3.0 T MRI scanner (Siemens Healthineers, Erlangen, Germany), with below-listed parameters: TR = 2000ms, TE = 2.25 ms, TI= 900ms, matrix = 256 × 256, FOV = 256mm×256mm, 192 slices, voxel size = 1 mm× 1 mm× 1 mm.
FreeSurfer 6.0 software was employed for post-processing of the T1WI images to generate SBM cortical features including cortical volume, cortical thickness, surface area and curvature.
The obtained cortical features were compared between IXT and HC groups with a vertex-level P value set at <0.01, and cluster-level threshold P<0.05.
Results
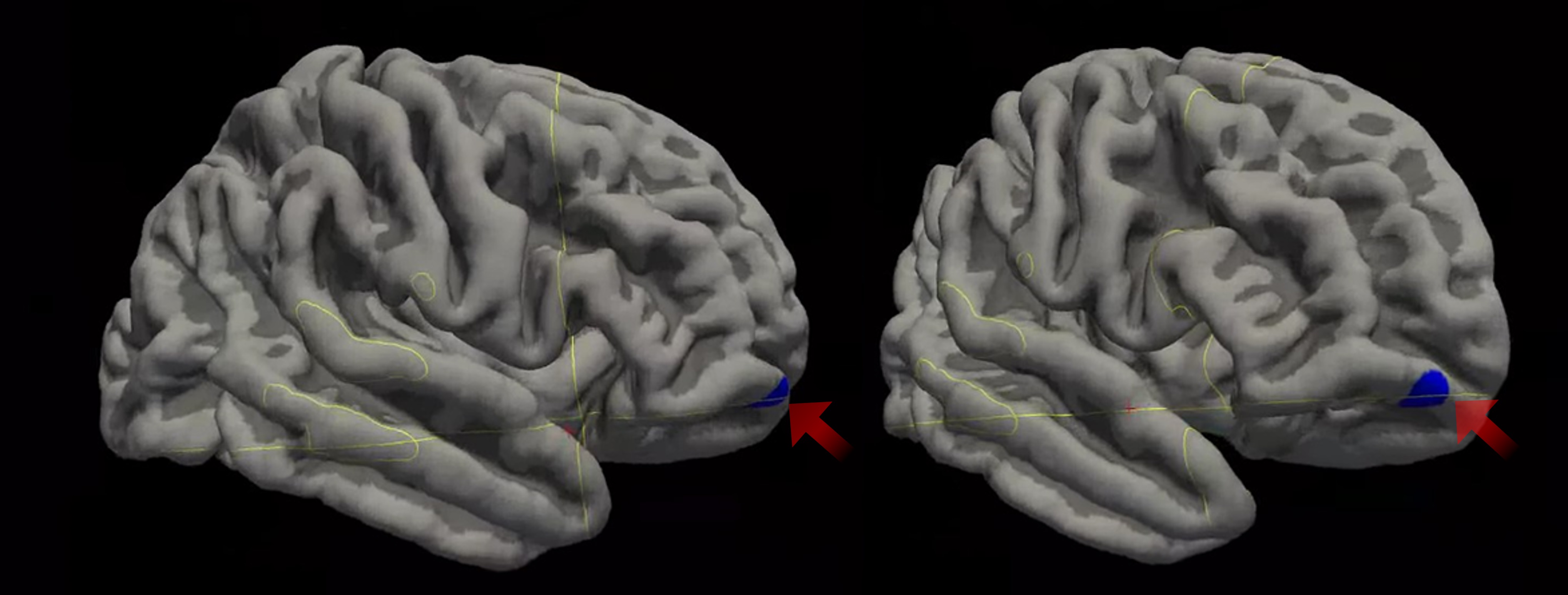
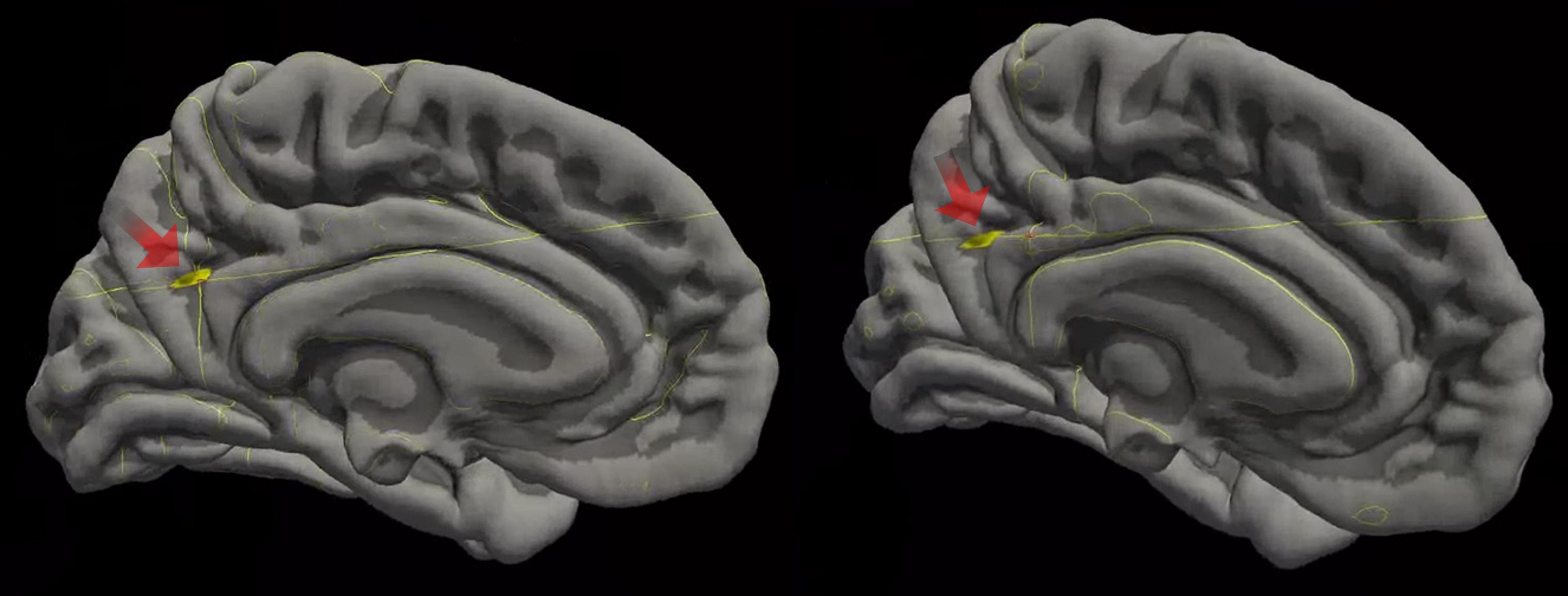
Compared to HCs, IXT patients demonstrated significantly decreased cortical thickness on a cluster located in the right rostral middle frontal cortex (Table 1 and Figure 1) and increased cortical curvature on a cluster located in left precuneus cortex (Table 1 and Figure 2). No significant differences were found in surface area and cortical volume between the two groups.Discussion and Conclusion
The cluster that shows a decrease in cortical thickness is located in the rostral middle frontal gyrus, and the functions that have been found to be associated with vision and eye movements at this location are mainly eye movement control and visual search. [5] Another cluster that showed changes in cortical curvature is in the posterior part of the precuneus, and according to previous findings, brain function of this region is mainly about visuospatial imagery and visuospatial associative memory. [6] [7] And based on our findings, there’s a more significant statistically difference in the cortical thickness changes in the rostral middle frontal gyrus.Studies have demonstrated that surgery early in the course of this disease results in more satisfactory surgical outcomes, which may be related to the fact that binocular visual functions are not yet significantly involved early in the course of the disease and that younger patients have greater neuroplasticity and resilience, so that once ocular deviation is surgically corrected, the binocular visual function can be somehow restored or even improved after proper training. [8, 9] It has also been demonstrated that surgical treatment alone leads to a higher recurrence rate, while the efficacy of visual function training alone is not convincing either, but combined visual function training after surgery can lead to a more satisfactory outcome. [2] [10] This also implies that the clinical symptoms of IXT are not only affected by abnormal ocular motor function but are also related to the impaired function of the higher visual cortex.
Accordingly, we proposed a new hypothesis for the pathogenesis of this disease: firstly, the abnormality of rostral middle frontal gyrus leads to ocular deviation, which results in the inability of the incoming visual signals to be processed properly in the primary visual cortex, and then further involves the higher visual centers and causes binocular visual function loss. This hypothesis is not only consistent with the current consensus on the function of the two brain regions, but also explains the differences in efficacy of different treatment regimens in previous studies, which may further contribute to provide a new rationale for treatment design for those patients.
Acknowledgements
Ren-zhi Wang, Zhaohui Liu, and Xiang Wan are the corresponding authors of this article.References
1. Mohney, B.G., et al., Three-Year Observation of Children 3 to 10 Years of Age with Untreated Intermittent Exotropia. Ophthalmology, 2019. 126(9): p. 1249-1260.2. Dong, Y. and Y.-Y. Liu, Surgery at early versus late for intermittent exotropia: a Meta-analysis and systematic review. International Journal of Ophthalmology, 2021. 14(4): p. 582-588.
3. Wang, X., et al., Abnormal cortical morphology in children and adolescents with intermittent exotropia. Frontiers in Neuroscience, 2022. 16.
4. Zhu, H., et al., Structural and Functional Changes of Brain in Children With Intermittent Exotropia: A Study Combining Multiple MRI Modalities. Journal of Neuro-Ophthalmology, 2023. Publish Ahead of Print.
5. Passingham, R.E. and H.C. Lau, Acting, seeing, and conscious awareness. Neuropsychologia, 2019. 128: p. 241-248.
6. Schott, B.H., et al., Gradual acquisition of visuospatial associative memory representations via the dorsal precuneus. Hum Brain Mapp, 2019. 40(5): p. 1554-1570.
7. Margulies, D.S., et al., Precuneus shares intrinsic functional architecture in humans and monkeys. Proc Natl Acad Sci U S A, 2009. 106(47): p. 20069-74.
8. Repka, M.X., et al., The Relationship of Age and Other Baseline Factors to Outcome of Initial Surgery for Intermittent Exotropia. Am J Ophthalmol, 2020. 212: p. 153-161.
9. Dong, Y., L. Nan, and Y.Y. Liu, Surgery at early versus late for intermittent exotropia: a Meta-analysis and systematic review. Int J Ophthalmol, 2021. 14(4): p. 582-588.
10. Heydarian, S., et al., Non-surgical Management Options of Intermittent Exotropia: A Literature Review. J Curr Ophthalmol, 2020. 32(3): p. 217-225.
Figures