2920
Correlation Between Cortical Thickness and Motor Functions in Individuals with Cerebral Small Vessel Disease Burdens1Key Laboratory of Endocrine Glucose & Lipids Metabolism and Brain Aging, Ministry of Education; Department of Radiology, Shandong Provincial Hospital Affiliated to Shandong First Medical University, jinan, China, 2Department of Psychiatry and Psychotherapy, Jena University Hospital, Jena, Germany; Center for Intervention and Research on adaptive and maladaptive brain Circuits underlying mental health (C-I-R-C), Jena-Magdeburg-Halle, Germany, 3Department of Radiology, Beijing Tsinghua Changgung Hospital, beijing, China, 4School of Medical Imaging, Binzhou Medical University, No. 346 Guanhai Road, Yantai, jinan, China
Synopsis
Keywords: Gray Matter, Gray Matter, Cerebral small vessel disease, timed up and go, cortical thickness, motor impairment, right insular cortex
Motivation: Delve into the cortical territories most vulnerable to cerebral small vessel disease (CSVD)
Goal(s): Determine the pivotal cortical zones that play a crucial role in mediating motor dysfunction in patients affected by CSVD, and scrutinize the risk factors that could potentially influence these pertinent cerebral areas.
Approach: Cortical thickness measurements were acquired utilizing an integrated approach of magnetic resonance imaging (MRI) and FreeSurfer technology.
Results: The right insular cortex holds a crucial position in the cascade of motor impairments observed in individuals diagnosed with CSVD. Body Mass Index (BMI) emerges as a potentially vital risk factor.
Impact: Focusing on the cortical thickness of the right insular cortex in individuals with CSVD and the risk factors that influence it (such as BMI) may lead to a better understanding and early intervention for motor impairment in individuals with CSVD.
Introduction
Cerebral small vessel disease (CSVD) is a common condition among the elderly, often leading to varying degrees of motor impairment1. Recognizing the pivotal role the cerebral cortex holds in orchestrating human motor functions, our research delves into the cortical regions most profoundly affected by CSVD burdens. Additionally, we probed potential risk factors influencing cortical thickness, aiming to establish foundational knowledge for mitigating cognitive and functional detriments associated with CSVD. Our study further elucidates the specific cortices potentially mediating these gait disturbances in individuals with CSVD and examines the interplay between different gyri that jointly determine the motor capabilities of those afflicted. Such nuanced comprehension offers invaluable perspectives on the gait challenges confronted by individuals with CSVD.Methods
This is a cross-sectional study. Between January 2021 and October 2022, we recruited 177 individuals with CSVD and 70 healthy controls. Criteria for individuals with CSVD inclusion encompassed: (1) Age exceeding 40; (2) Manifestation of recent small subcortical infarct, lacune (presumed vascular in origin), white matter hyperintensity (presumed vascular in origin), perivascular space, cerebral microbleed, cortical superficial siderosis, brain atrophy, cortical cerebral microinfarct, or a score derived from the most recent MRI consensus criteria for CSVD2. Exclusionary criteria included: (1) Pronounced musculoskeletal ailments; (2) Inability to independently walk a continuous distance of over 10 meters;(3) MRI contraindications or aversion to undergoing an MRI procedure. All subjects participated in the TUG assessment to gauge their mobility and gait challenges. For the acquisition of cortical thickness information, we utilized the Desikan-Killiany Atlas (DKT atlas) as the standard template provided by FreeSurfer.Results
A variance analysis of the cortical thickness across the 68 cerebral regions pinpointed significant variations in six gyri: the bilateral lateral occipital gyri, bilateral insula gyri, left rostral anterior cingulate gyrus, and right pars orbital gyrus (Figure 2). After adjusting for age, gender, educational level, and total brain volume, the differences in the aforementioned six brain regions remained statistically significant. Age consistently emerged as a pivotal risk factor across all six gyri (Figure 3). CSVD burdens influenced five gyri, with the exception being the right pars orbital gyrus. Intriguingly, Aβ1-42 levels were uniquely associated with the left lateral occipital gyrus (Figure 3). Beyond age and the severity of CSVD, BMI also plays a crucial role in influencing the thickness of the right insula (P = 0.001, standardized B = -0.234), although its impact on the other five cortical regions does not reach statistical significance. Adjusted correlation tests with the TUG demonstrated a significant linkage solely with the bilateral insula gyri (P = 0.005, P < 0.001, FEW-corrected, R = -0.213, R= -0.268). In the stepwise regression, we incorporated age and group distinctions—factors with a marked bearing on TUG results—and treated the thickness of the six gyri as independent variables. The thickness of the right insula gyrus was discerned to have a significant correlation with TUG performance (P = 0.024, standardized B = -0.152 Figure 3). We observed that within these six brain regions, the cortical thickness of the CSVD-S group significantly differed from that of the HCs group. Notably, in the right insula, discernible differences can even be seen among all three groups (Figure 4). Mediation analysis unveiled the right insula gyrus as a partial mediator between severe CSVD and TUG results (Figure 5). Moreover, the right insula gyrus entirely mediated the nexus between the left rostral anterior cingulate and TUG outcomes.Discussion
Notably, a diminished thickness in the right insula was partially correlated with the TUG test performance in individuals with severe CSVD. This suggests that the right insula's thickness may play a crucial role in the CSVD burdens and motor functions. BMI may serve as a significant risk factor influencing the thickness of the right insula. It's plausible that the right insula maintains a functional interplay or connectivity with the left rostral anterior cingulate gyrus, so they may jointly participate in brain networks or circuits associated with motor functions. A deeper probe into the insular cortex's role within neural networks and its functional ties pertinent to motor functions is imperative for a comprehensive grasp of motor challenges in individuals with CSVD.Conclusions
Our insights shed light on the pivotal cortical regions intertwined with the motor deficits and intentional behaviors characteristic of individuals with CSVD. We've delved into the determinants shaping cortical thickness and propose that, within individuals with CSVD, intricate neural networks and functional interconnections spanning diverse cortical strata might jointly dictate their motor prowess. We should also pay attention to the impact of BMI on the thickness of the right insula.Acknowledgements
We would like to acknowledge study participants involved in the clinical datasetReferences
1. de Laat KF, Reid AT, Grim DC, et al. Cortical thickness is associated with gait disturbances in cerebral small vessel disease. Neuroimage. 2012;59(2):1478-1484. doi:10.1016/j.neuroimage.2011.08.005
2. Duering M, Biessels GJ, Brodtmann A, et al. Neuroimaging standards for research into small vessel disease-advances since 2013. The Lancet Neurology. 2023;22(7):602-618. doi:10.1016/s1474-4422(23)00131-x
Figures
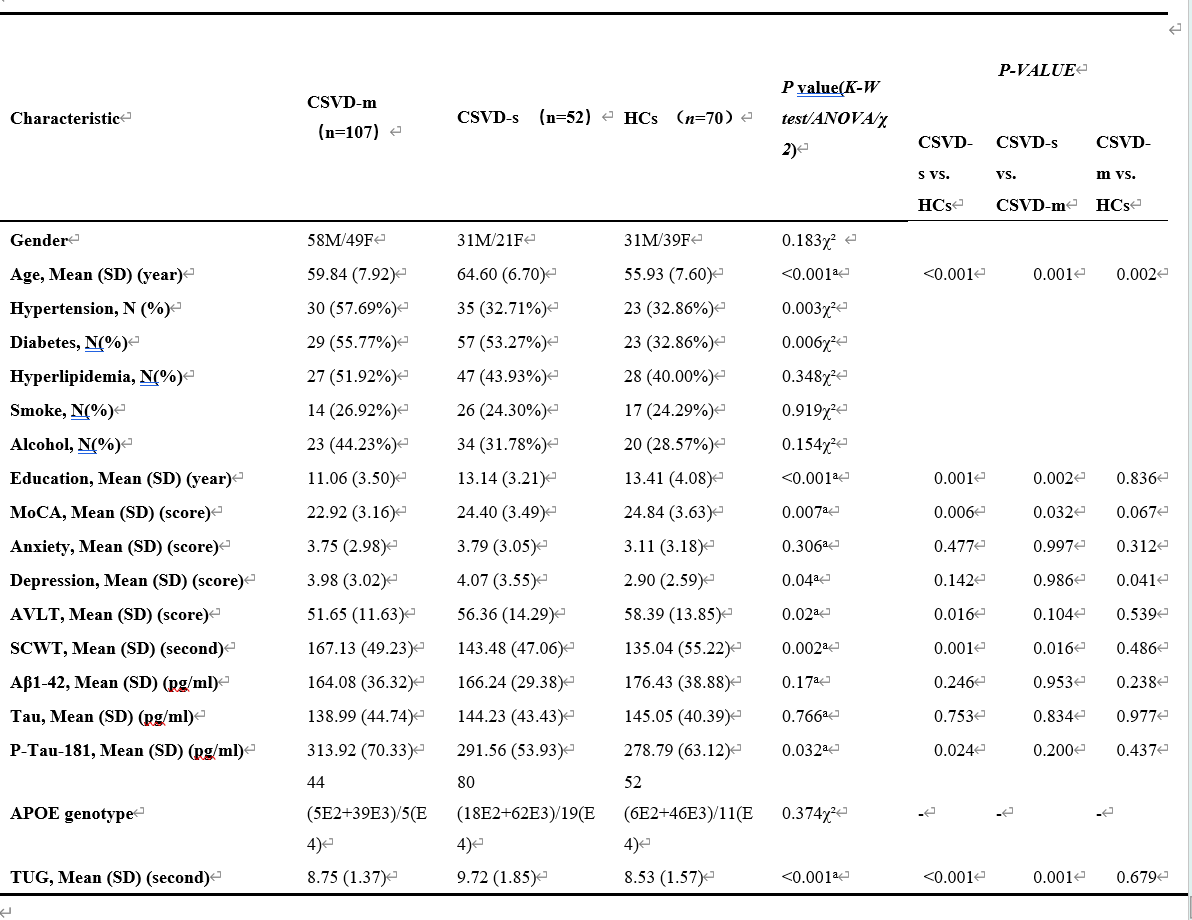
Figure 1. Participant characteristics.
Notes: CSVD-S = CSVD patients with severe CSVD burden scores; CSVD-M = CSVD patients with mild or moderate CSVD burden scores; HCs = healthy controls.
χ2: chi-square test, a: Kruskal-Wallis test(K-W test), b:One-way ANOVA analysis.
MoCA: Montreal Cognitive Assessment, SCWT: Stroop Colour Word Test.
TUG: Timed Up and Go Test: A clinical assessment tool used to evaluate an individual's mobility and balance.
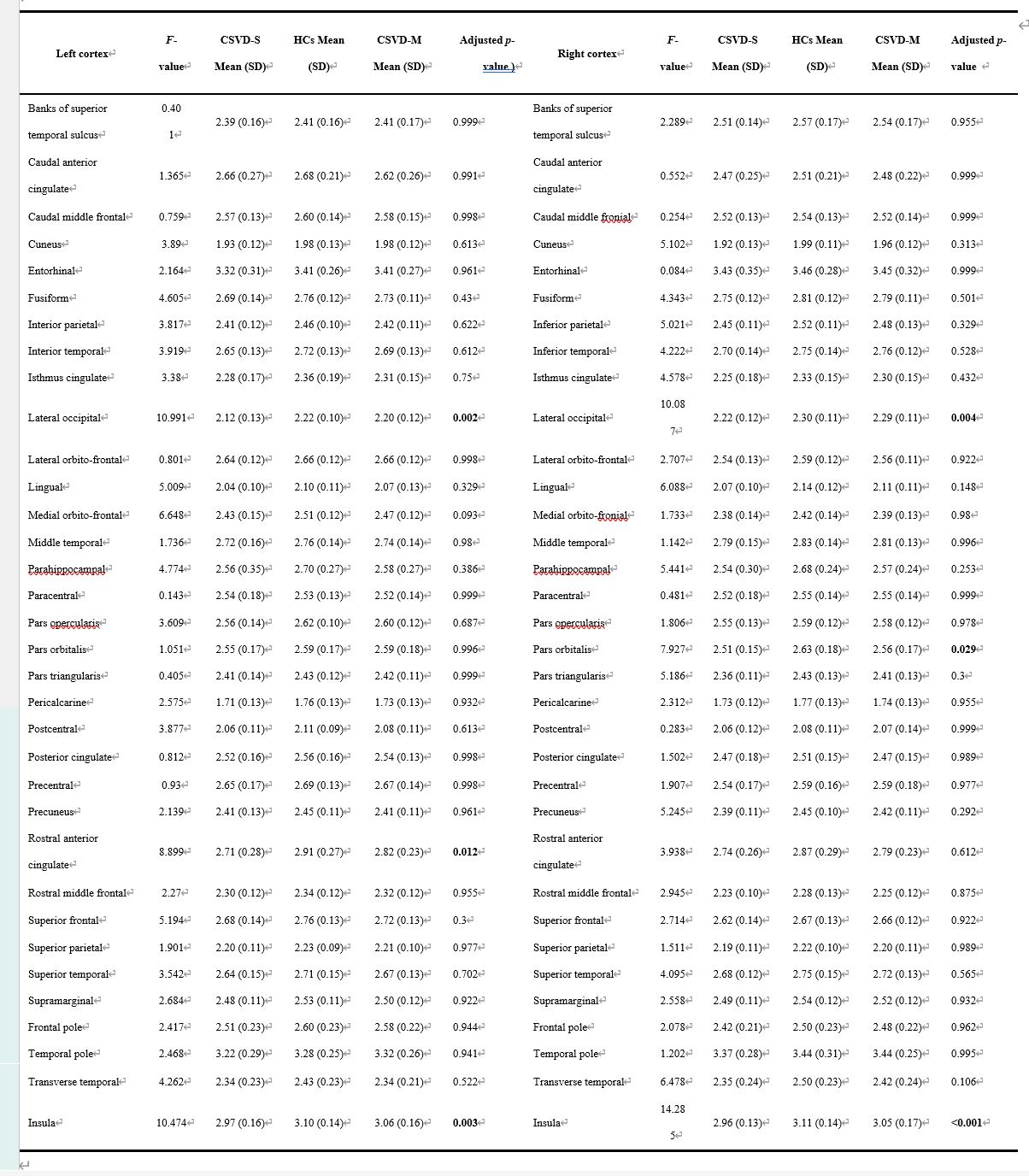
Figure 2.
In the chart presented, we conducted a univariate analysis of variance (ANOVA) across 68 brain regions for the three groups: CSVD-S, CSVD-M, and HCs. The p-values were then subjected to FWE correction using the Holm-Sidak method. Six brain regions showed significant differences with FWE-corrected p-values, which have been highlighted in bold. Additionally, we calculated the mean cortical thickness and its standard deviation for each region in the three groups, presenting the results in the format of mean (standard deviation).
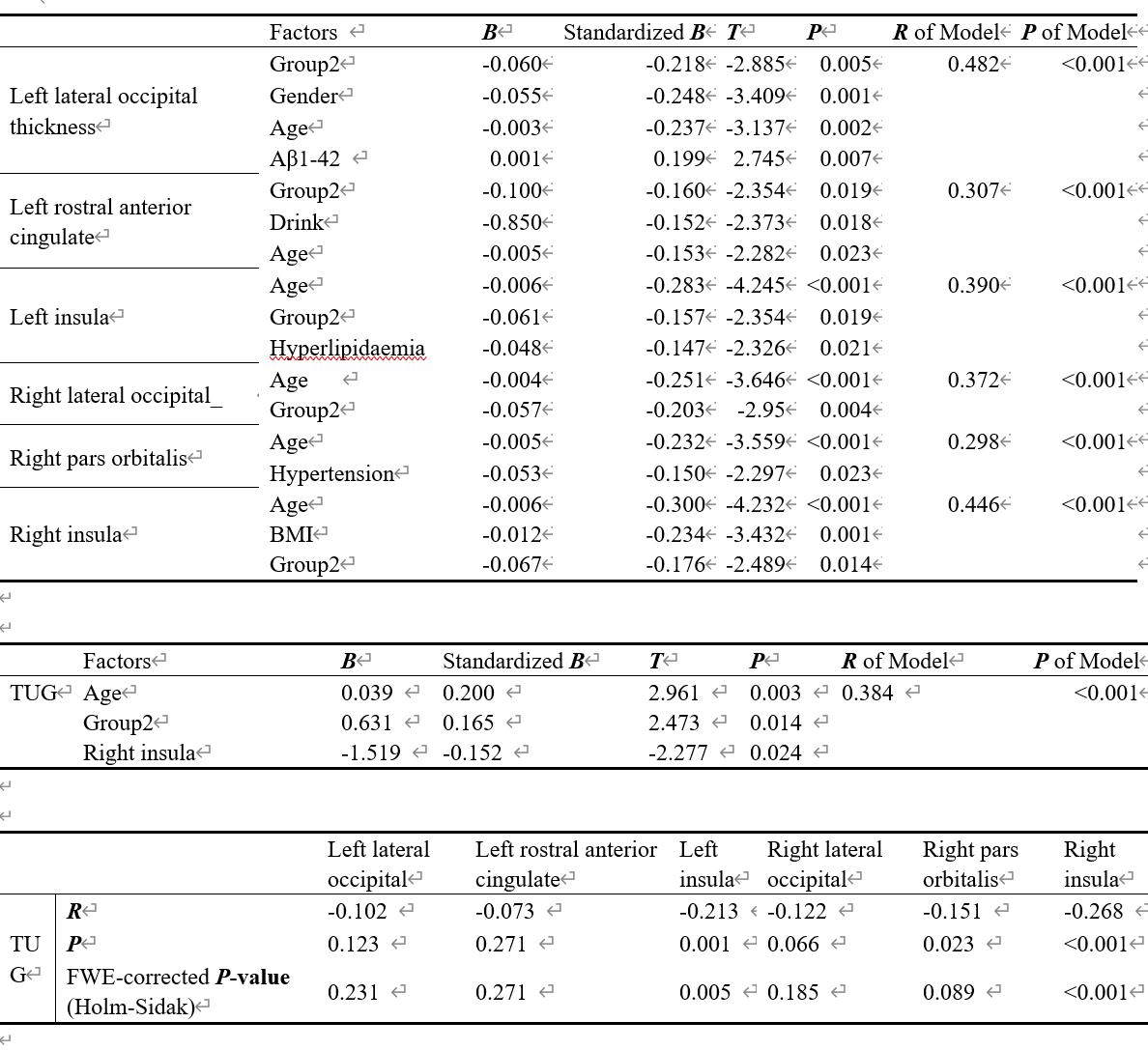
Figure 3.
The first table represents the results after our preliminary screening of risk factors for the six brain gyri. From this screening, we selected the risk factors most closely related to the gyri (P<0.1) and conducted stepwise regression analysis to pinpoint the most probable risk factors affecting cortical thickness in cerebral small vessel disease. In Table 2, we incorporated age and group type, and then performed a stepwise regression analysis between the six cortices and TUG. Table 3 presents a correlation analysis between the six brain gyri and the TUG.
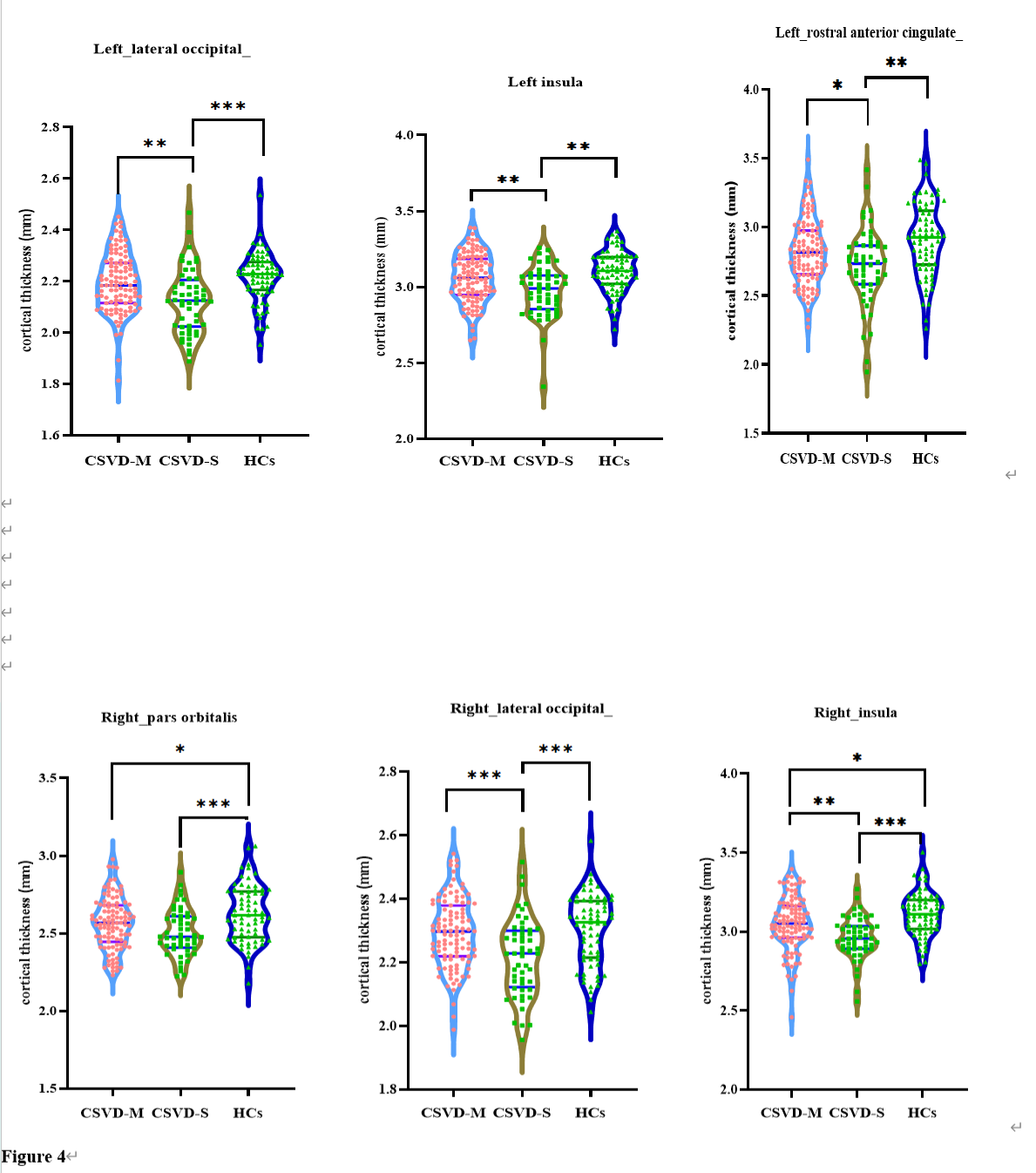
Figure 4
We observed that within these six brain regions, the cortical thickness of the CSVD-S group significantly differed from that of the HCs group. Notably, in the right insula, discernible differences can even be seen among all three groups. *P < 0.05; **P < 0.01; ***P < 0.001. CSVD-S refers to patients with severe CSVD burden scores, CSVD-M denotes patients with mild or moderate CSVD burden scores, and HCs represents healthy controls.
Group2: Individuals with severe CSVD burdens (2, 3, 4)
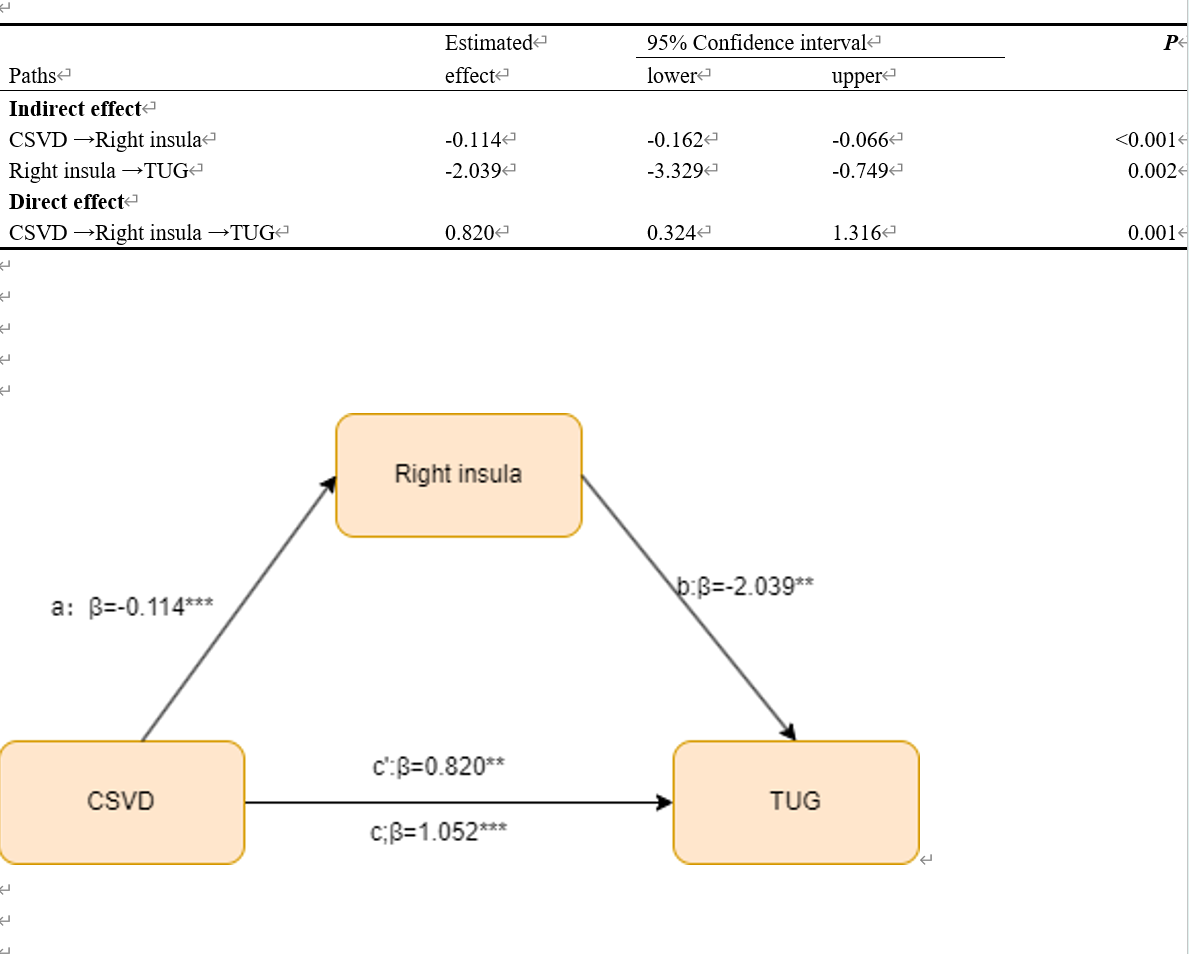
Figure 5. Mediation analysis model.
In patients with severe cerebral small vessel disease, the thickness of the right insular gyrus exhibited a partial mediating effect on the TUG test