2918
Pulmonary functional imaging for patients with obstructive lung disease using UTE MRI1Department of Radiology, Second Affiliated Hospital of Naval Medical University, Shanghai, China, 2College of Health Sciences and Engineering, University of Shanghai for Science and Technology, Shanghai, China, 3GE Healthcare, Beijing, China, 4Department of Thoracic Surgery, Second Affiliated Hospital of Naval Medical University, Shanghai, China
Synopsis
Keywords: Lung, Lung, UTE;fractional ventilation;pulmonary function tests;
Motivation: This study aimed to assess the feasibility of using single breath-hold UTE MRI to quantify pulmonary function and its spatial uniformity in patients with obstructive lung disease.
Goal(s): Comparison of FV in patients with different respiratory stages and correlation with PFTs.
Approach: FV map was obtained from UTE MRI, and IQR of FV was calculated. Group differences of UTE parameters were compared, and correlation between UTE MRI with PFT parameters was assessed.
Results: We found significant differences in whole lung FV and left lung FV among groups, with a positive correlation between FV and PFT parameters such as FEV1 and MMEF.
Impact: This study demonstrates the potential of UTE MRI for assessing pulmonary function in obstructive lung disease patients. By providing regional functional information, UTE MRI might be a useful tool in lung disease management.
Introduction
Lung diseases exhibit diverse patterns, necessitating methods that offer regional information. Currently, evaluation of lung function and structure is conducted by two separate processes for tracking pulmonary conditions and disease advancement. Methods in clinical practice include pulmonary function tests (PFTs) and body plethysmography. Additionally, chest CT are routinely employed to assess structural characteristics associated with airways and regionally parenchymal abnormalities1. However, these approaches have limitations, especially in pediatric cases. In contrast, MRI offers morphological and functional insights without ionizing radiation, making it crucial for early disease detection. However, lung MRI faces challenges due to respiratory and cardiac motion, as well as low MRI signal2-4. Ultrashort echo time (UTE) MRI have gained prominence for imaging short T2* compounds, thus providing the foundation for pulmonary structural and functional evaluation5,6. Analyzing intensity changes in lung parenchyma over respiratory and cardiac cycle can offer diagnostically relevant information for lung ventilation and perfusion without the need for contrast agents or special breathing conditions7,8. This approach utilized real-time MRI with Fourier-decomposition analysis to quantify fractional ventilation and perfusion9. Fischer et al. expanded this method by incorporating respiratory and cardiac self-gating imaging with Fourier analysis for ventilation and perfusion assessment10, eventually translating it to UTE for lung functional quantification11. In this study, we aimed to evaluate the feasibility of using single breath-hold UTE MRI across different respiratory phases to quantify the pulmonary function and its spatial homogeneity for patients with obstructive lung disease, and investigate the correlation between UTE MRI and PFT parameters.Materials and Methods
This prospective study was approved by the Ethics Committee of our hospital. A total of 18 patients with obstructive lung disease confirmed by CT and PFTs were enrolled. According to the severity of the disease, we categorized patients into 3 groups: 1) People with normal pulmonary function; 2) Ventilation abnormalities suggested by pulmonary function; 3) Ventilation abnormalities due to pulmonary masses. PFT parameters including forced vital capacity (FVC), forced expiratory volume (FEV1), FEV1/FVC ratio, peak expiratory flow (PEF), maximum mid-expiratory flow (MMEF), diffusion capacity of carbon monoxide (DLCO), residual volume (RV), and total lung capacity (TLC) were recorded. Lung MRI examinations were performed on a 3.0 T MRI scanner (SIGNATM Premier; GE Healthcare, Milwaukee, WI) equipped with a 21-channel AIRTM flexible coil. End-inspiration and end-expiration breath-hold UTE images were acquired with following parameters: FOV = 400 x 400 mm, matrix = 200 x 200, slice thickness = 12 mm, TR/TE = 4.5/0.032 ms, flip angle = 8°. The data analysis was conducted using a custom MATLAB code, following the procedures reported by the previous study12 (Figure 1). Specifically, we performed automatic lung parenchyma segmentation on end-expiration UTE images by graph-based segmentation approach with predefined seeds, then employed active contour method based on the Chan-Vese algorithm. Subsequently, nonrigid image registration between end-expiration and end-inspiration UTE images was performed. Finally, fractional ventilation (FV) can be calculated by: (SIend-inspiration-SIend-expiration)/ SIend-inspiration. To assess the homogeneity of regional ventilation, the interquartile range (IQR) of the normalized FV was further calculated. One-way ANOVA and post-hoc tests were performed to compare group differences of FV and IQR values. Spearman correlation coefficient was obtained to assess correlation between FV and IQR values with PFT parameters.Results
Figure 2 displays the FV maps of 3 representative patients from each group. A progressive reduction in FV values from patients in group1 to group3 can been found by visual inspection.Figure 3 demonstrates the comparison of FV and IQR values among groups. The whole lung FV and IQR were 0.23±0.02 and 0.61±0.10 in group1, 0.21±0.01 and 0.68±0.11 in group2, 0.19±0.03 and 0.68±0.05 in group1, respectively. One-way ANOVA indicated that whole lung FV (p = 0.019) and left lung FV (0.040) were significantly different among 3 groups, and post-hoc tests denoted that goup1 was significantly higher than group3 in these two parameters (p < 0.05). No difference was found in IQR value among groups. Figure 4 shows the correlation analysis results. We observed that there were significant positive correlations between whole lung FV with FEV1 (r = 0.600, p = 0.008), FEV1/FVC ratio (r = 0.598, p = 0.010), and MMEF (r = 0.717, p = 0.001) values.
Discussion
This study has demonstrated the feasibility of single breath-hold UTE MRI for pulmonary functional imaging in patients with obstructive lung disease. Specifically, we found that FV values can be used to differentiate the disease severity, and were positive correlated with varies PFT parameters. By providing regional functional information, UTE MRI might be a useful tool in lung disease management.Acknowledgements
NoReferences
1. Smyth AR, Bell SC, Bojcin S, et al. European Cystic Fibrosis Society Standards of Care: Best Practice guidelines. J Cyst Fibros. 2014; 13(Suppl 1)S23-42.
2. Wild JM, Marshall H, Bock M, et al. MRI of the lung (1/3): Methods. Insights Imaging. 2012; 3:345-353.
3. Yu J, Xue Y, Song HK. Comparison of lung T2* during free-breathing at 1.5 T and 3.0 T with ultrashort echo time imaging. Magn Reson Med. 2011; 66:248-254.
4. Theilmann RJ, Arai TJ, Samiee A, et al. Quantitative MRI measurement of lung density must account for the change in T with lung inflation. J Magn Reson Imaging. 2009; 30:527-534.
5. Johnson KM, Fain SB, Schiebler ML, Nagle S. Optimized 3D ultrashort echo time pulmonary MRI. Magn Reson Med. 2013; 70:1241-1250.
6. Bae K, Jeon KN, Hwang MJ, et al. Comparison of lung imaging using three-dimensional ultrashort echo time and zero echo time sequences: Preliminary study. Eur Radiol. 2019; 29:2253-2262.
7. Lederlin M, Crémillieux Y. Three-dimensional assessment of lung tissue density using a clinical ultrashort echo time at 3 Tesla: A feasibility study in healthy subjects. J Magn Reson Imaging. 2014; 40:839-847.
8. Veldhoen S, Weng AM, Knapp J, et al. Self-gated non–contrast enhanced functional lung MR imaging for quantitative ventilation assessment in patients with cystic fibrosis. Radiology. 2016; 283:242-251.
9. Bauman G, Puderbach M, Deimling M, et al. Non-contrast-enhanced perfusion and ventilation assessment of the human lung by means of Fourier decomposition in proton MRI. Magn Reson Med. 2009; 62:656-664.
10. Fischer A, Weick S, Ritter CO, et al. Self-gated non-contrast-enhanced functional lung imaging (SENCEFUL) using a quasi-random fast low angle shot (FLASH) sequence and proton MRI. NMR Biomed. 2014; 27:907-917.
11. Mendes Pereira L, Wech T, Weng AM, et al. UTE-SENCEFUL: First results for 3D high-resolution lung ventilation imaging. Magn Reson Med. 2019; 81:2464-2473.
12. Balasch A, Metze P, Stumpf K, et al. 2D Ultrashort echo-time functional lung imaging. J Magn Reson Imaging. 2020; 52(6):1637-1644.
Figures
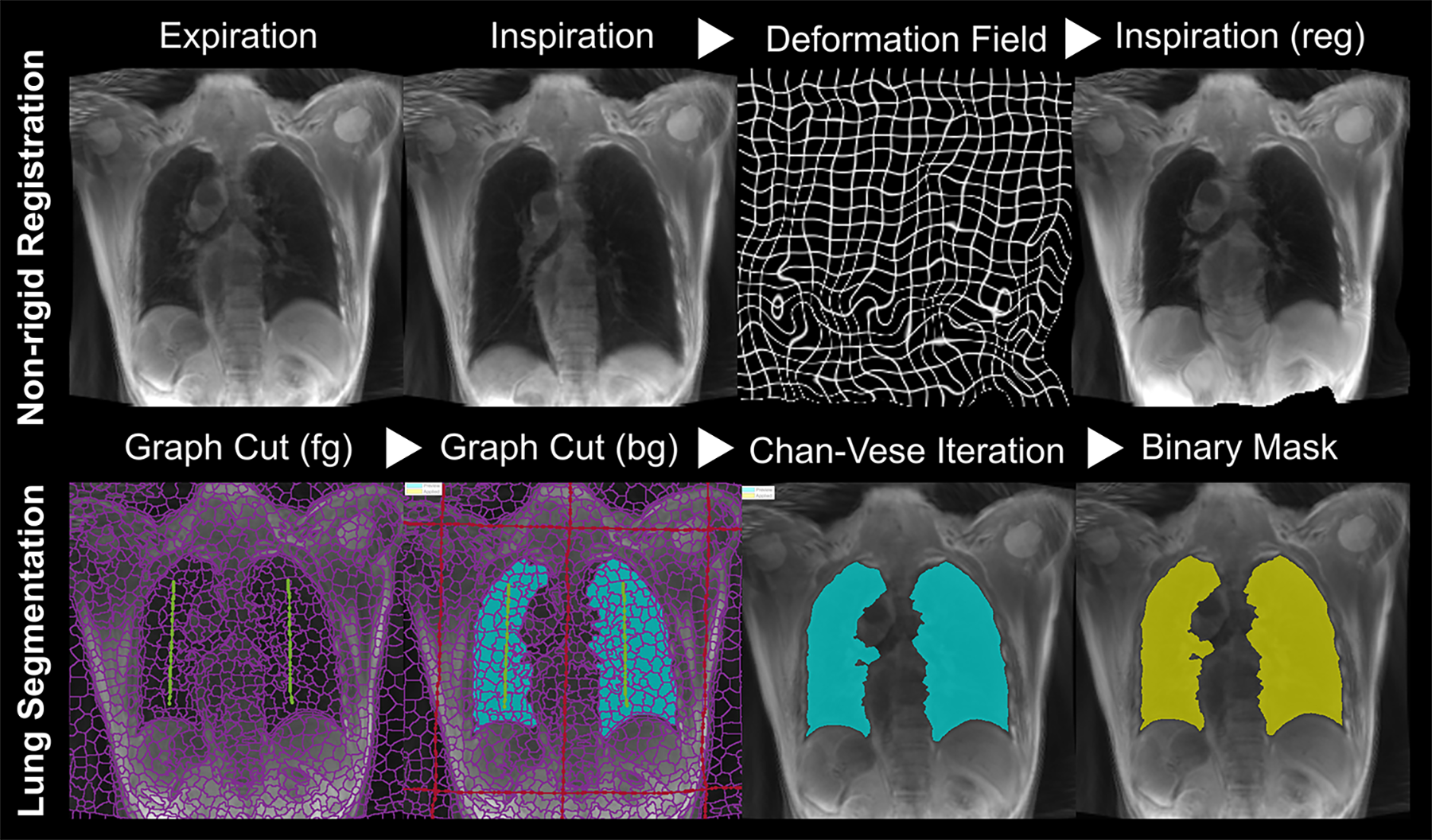
Figure 1. Automatic segmentation of lung parenchyma and non-rigid image alignment between end-expiratory and end-inspiratory UTE images.
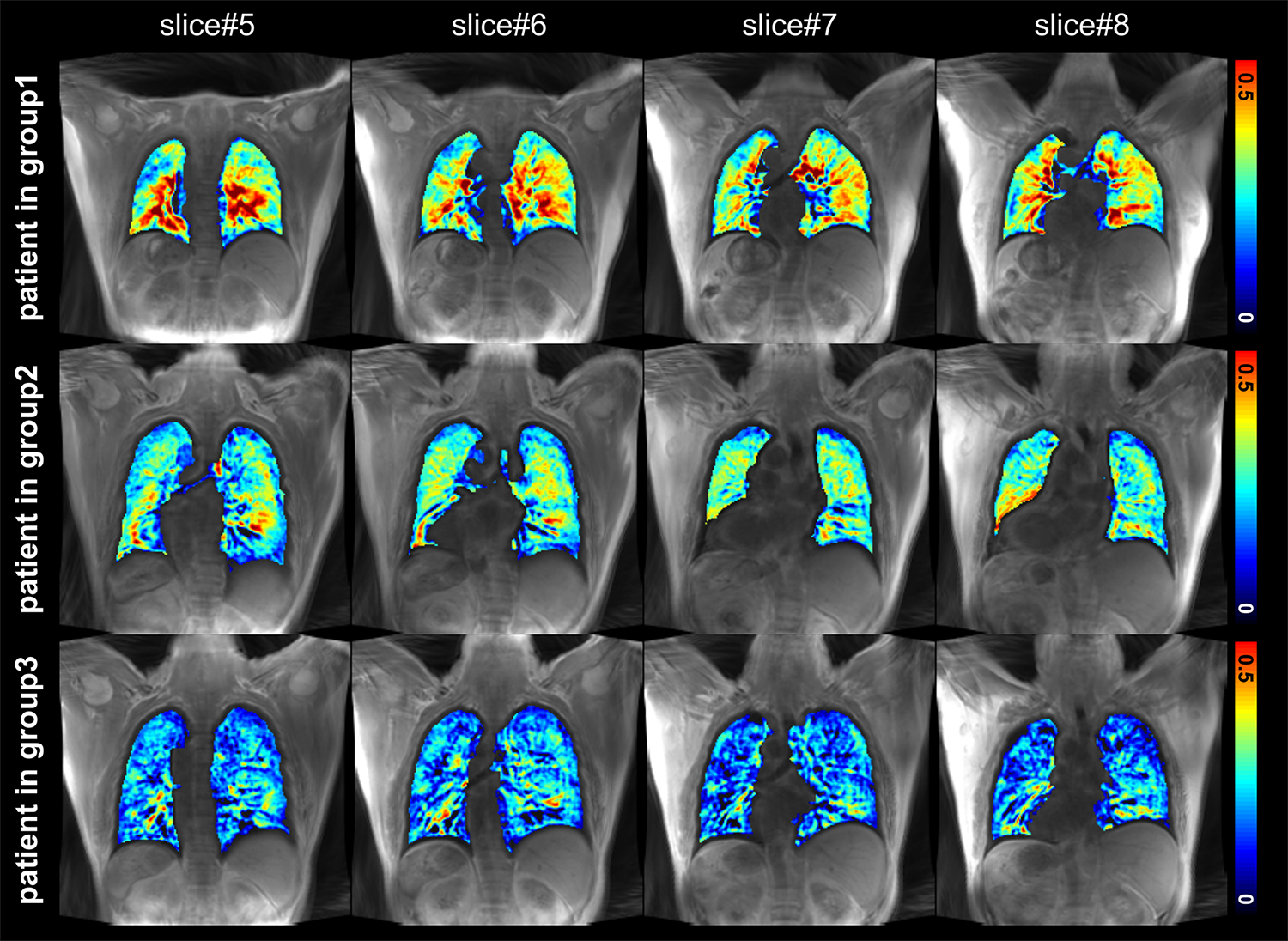
Figure 2. The FV maps of 3 representative patients from each group.
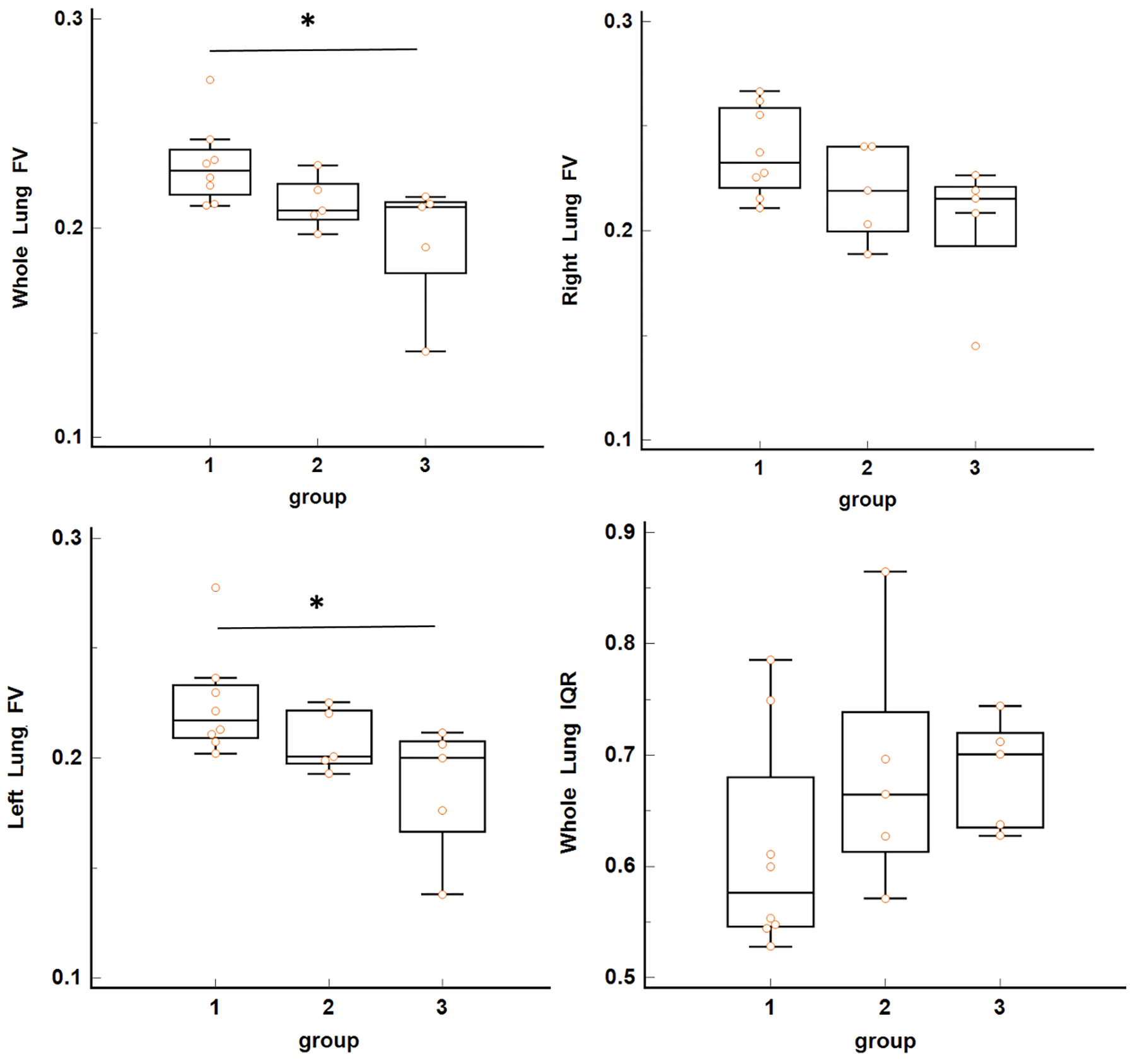
Figure 3. Comparison of FV and IQR values among groups.
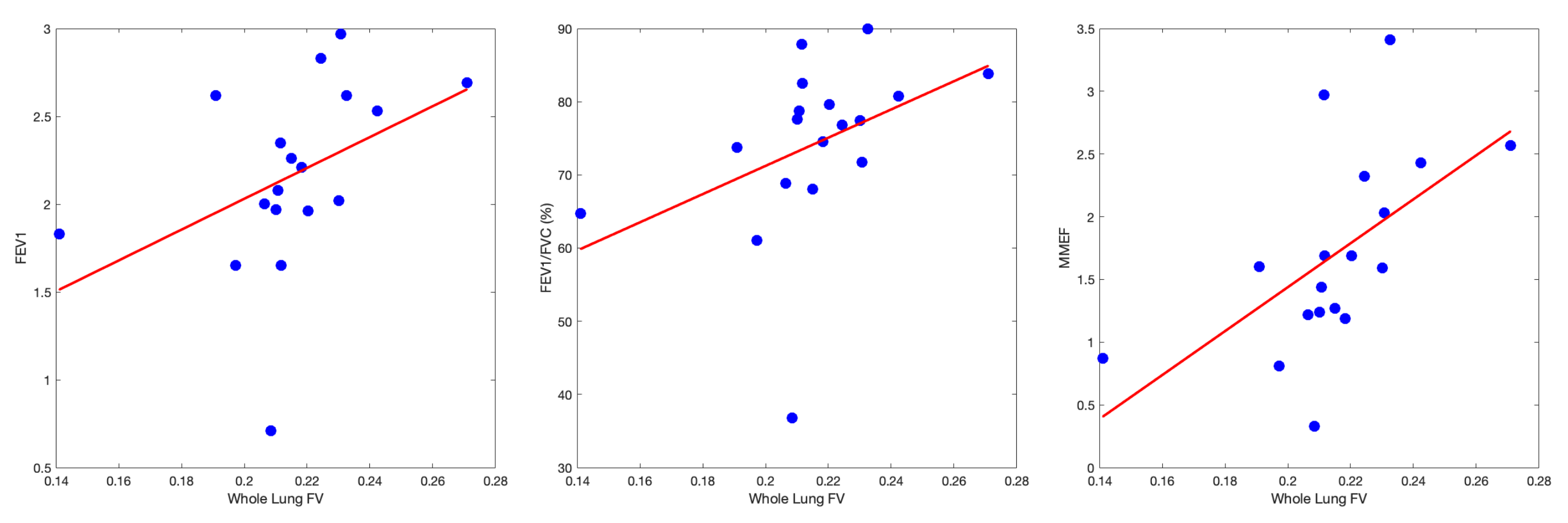
Figure 4. The results of FV and PFT correlation analysis.