2917
Using a Shinnar LeRoux Pulse for 3D Multi Ultra-short TE Look-locker Inversion Recovery for T1-Mapping in the human lungs1Diagnostic and Interventional Radiology, University Hospital Heidelberg, Heidelberg, Germany, 2Translational Lung Research Center Heidelberg, Member of the German Center for Lung Research, Heidelberg, Germany
Synopsis
Keywords: Lung, Lung
Motivation: Lung T1(TE) quantification using 2D UTE was demonstrated as an interesting tool but needs expansion to 3D UTE for better comparability and coverage. However, streaking artefacts originating from the edges of the Field of View are particularly problematic in Lung T1(TE) maps.
Goal(s): To reduce streakings in T1(TE) maps caused by B0 inhomogeneities.
Approach: A Shinnar LeRoux (SLR) minimum phase pulse was used to limit excitation to a 320mm slab in the Multi Ultra-short TE Look-Locker Inversion Recovery sequence.
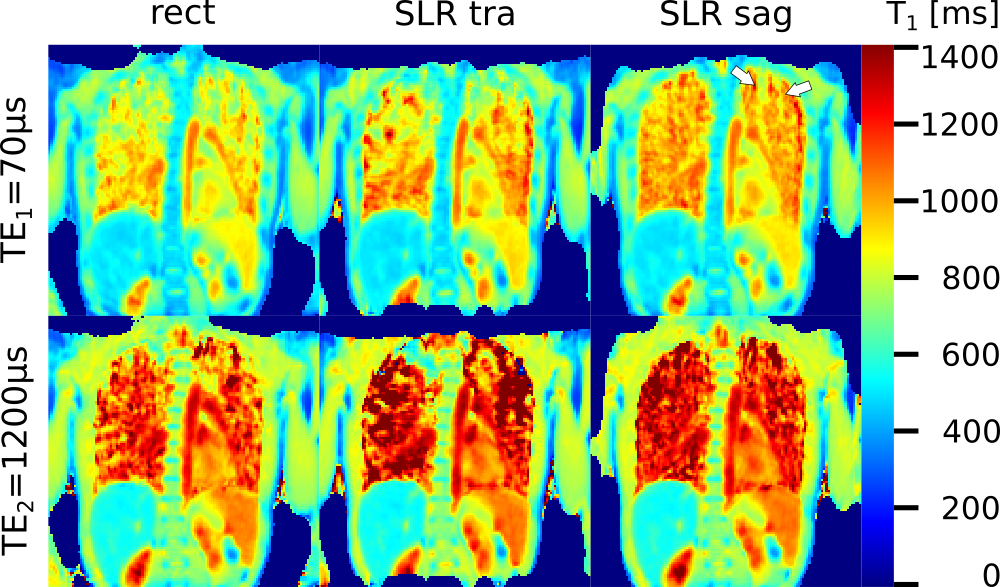
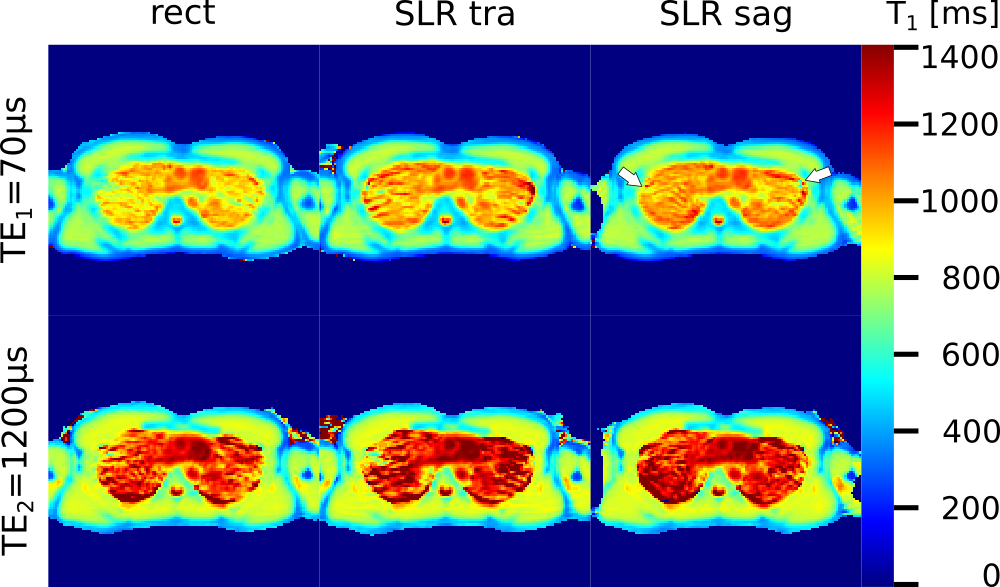
Results: T1(TE) maps produced using sagittal SLR excitation showed less streakings than using transverse SLR excitation and rectangular pulses, but still had residual streaking.
Impact: Inhomogeneity streakings in 3D UTE lung T1(TE) maps were greatly reduced by employing a SLR pulse. With additional efforts during reconstruction, it may be possible to remove the remaining artefacts and quickly acquire parameter maps of the entire lungs.
Introduction
The quantification of echo-time dependent T1 (T1(TE)) in the lungs has been shown to provide potentially useful information both in patients with cystic fibrosis (CF) and chronic obstructive pulmonary disease (COPD) [1,2,3]. T1 not only depends strongly on local perfusion because of the long T1 of blood protons, intra- and inter-patient correlations between T1 and contrast-agent based perfusion MRI have been shown to depend on TE [4]. Perfusion in the lungs is particularly interesting since the mechanism of hypoxic pulmonary vasoconstriction directly links perfusion to ventilation, which can thus be used to depict functional impairment in obstructive lung diseases. However, correlations of T1 with measures of parenchymal abnormalities showed different TE-dependence than with perfusion [2,3]. So far, T1(TE) mapping has been demonstrated using a 2D UTE approach limited to individual slices, while contrast-agent based 4D perfusion measurements cover the entire lungs in 3D acquisitions (while requiring breath-holds). Free breathing 3D lung T1 mapping using a radial approach has been shown, based on cylindrical encoding, which thus could not provide ultra-short TE, which is of particular interest in the further investigation of the TE-dependence of lung T1, in addition of potentially providing additional signal in the lungs [5]. This work aims to further 3D UTE T1-mapping specifically in the lungs. Initially, 3D UTE utilized non-selective excitation using rectangular pulses. However, a primary problem are streaking artefacts from the edges of the Field of View, caused by the field inhomogeneities in the outer areas of the magnet bore. Normally, these would not be relevant, but since the proton density in the lungs is so low, they can easily distort T1. To reduce this, the use of Shinnar LeRoux (SLR) pulses has been suggested for morphological 3D UTE in the lungs [6].Methods
All measurements were performed on healthy volunteers on a 1.5T scanner (Avanto, Siemens Healthineers, Erlangen, Germany). All participants provided written informed consent, and the study was approved by the institutional ethics committee. Three excitation schemes were used: A 300μs duration SLR minimum phase-pulse with 4% ripple in both pass- and stopband was used to limit the excitation to a 320mm thick slab, separately in sagittal and in transverse orientation and a 60μs rectangular pulse was used for a non-selective excitation. A ‘cooshball’ encoding scheme with 3D center-out radial trajectories using ramp-sampling was employed. In all cases, a 2-dimensional golden angle increment adapted to the inversion recovery was used [7]. The measurement was divided into blocks with a global inversion pulse followed by 1000 radial projections, separated by 3s delays. To avoid subjects synchronizing their breathing cycle to the measurement, gradients were continued during the delay. Further acquisition parameters were TR=3ms; TE1,2=70μs,1200μs; α=6°; total projections 54000. Images were reconstructed using a non-uniform Fourier Transform and a sliding window 4181 projections wide with 2584 step-width. The resolution was 1283 points at 4503 mm3 FoV. This gave an effective time-resolution of 117ms and 5min 24s acquisition time. T1 was fitted from the inversion recovery to yield 3D T1 maps.Results
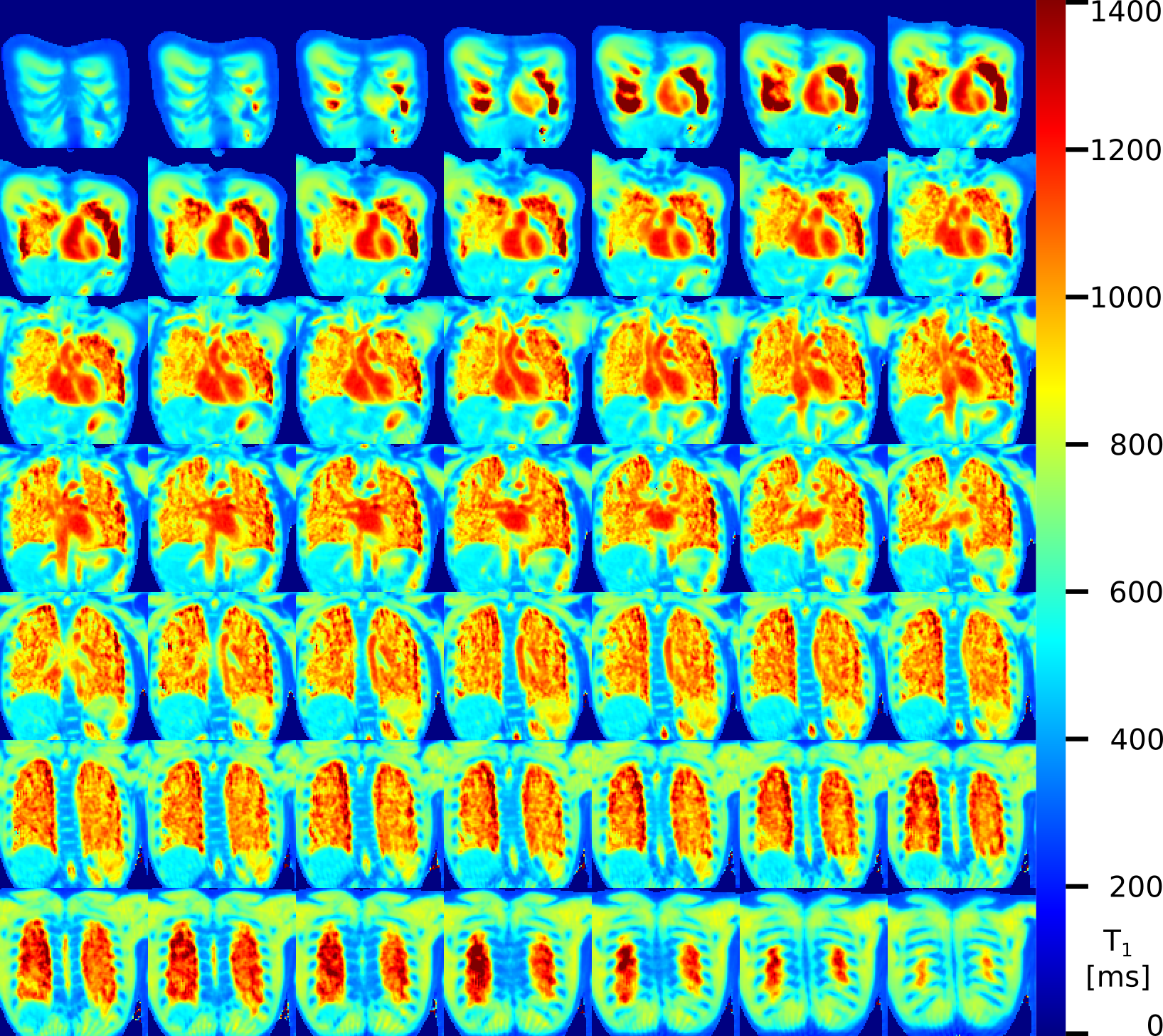
Figure 1 shows representative coronal slices of 3D T1 maps at both TEs from one volunteer for different excitation schemes, figure 2 equivalent transverse slices and figure 3 all coronal lung slices acquired in the lungs of a second volunteer. Streaking artefacts were greatly reduced in the maps produced with SLR slice-excitation and worse with transverse SLR excitation compared to sagittal. However, residual streakings were still visible in the sagittal maps (arrows in figure 1 & 2).Discussion
It has been shown previously that in healthy subjects, lung T1 is generally homogenous. Thus, residual image artefacts that distort T1 maps are still recognizable in healthy subjects, where lung T1 should be homogenous. However, to discern pathological abnormalities on parameter maps, a very low amount of localized artefacts is desirable. As shown here, using an SLR pulse with a sagittal slab excitation greatly reduces the artefacts visible in T1 maps when compared to the non-selective excitation with a rectangular pulse and the same SLR pulse but using a transverse slab. However, as seen in figure 1, residual streaking artefacts were still visible when using the SLR to excite a sagittal slab. Accordingly, further research will be required to make 3D T1(TE) quantification in the lungs at UTE practical. Techniques that suppress inhomogeneity streakings during reconstruction or coil combination could further improve parameter map quality [8,9].Acknowledgements
No acknowledgement found.References
1. Triphan SMF, Jobst BJ, Breuer FA, Wielpütz MO, Kauczor H-U, Biederer J, Jakob PM. Echo time dependence of observed T1 in the human lung. Journal of Magnetic Resonance Imaging 2015:42:610–616.
2. Triphan, S.M.F., Stahl, M., Jobst, B.J., Sommerburg, O., Kauczor, H.-U., Schenk, J.-P., Alrajab, A., Eichinger, M., Mall, M.A. and Wielpütz, M.O. (2020), Echo Time-Dependence of Observed Lung T1 in Patients With Cystic Fibrosis and Correlation With Clinical Metrics. J Magn Reson Imaging, 52: 1645-1654. https://doi.org/10.1002/jmri.27271
3. Triphan, S.M.F., Weinheimer, O., Gutberlet, M., Heußel, C.P., Vogel-Claussen, J., Herth, F., Vogelmeier, C.F., Jörres, R.A., Kauczor, H.-U., Wielpütz, M.O., Biederer, J., Jobst, B.J. and (2021), Echo Time-Dependent Observed Lung T1 in Patients With Chronic Obstructive Pulmonary Disease in Correlation With Quantitative Imaging and Clinical Indices. J Magn Reson Imaging, 54: 1562-1571. https://doi.org/10.1002/jmri.27746
4. Triphan, S.M.F, Konietzke, M., Biederer, J., Kauczor, H.-U., Heussel, C., Wielpütz, M. (2023), Local correlation of echo-time dependent observed lung T1 and quantitative perfusion in patients with chronic obstructive pulmonary disease. Proceedings of the ISMRM, #4665
5. Triphan, S.M.F., Wielpütz, M., Kauczor, H.-U., Jobst, B. (2018), 3D T1 mapping in the lungs during free breathing using asymmetrical cylindrical encoding. Proceedings of the ISMRM, #4356
6. Johnson, K.M., Fain, S.B., Schiebler, M.L. and Nagle, S. (2013), Optimized 3D ultrashort echo time pulmonary MRI. Magn. Reson. Med., 70: 1241-1250. https://doi.org/10.1002/mrm.24570
7. Chan, R.W., Ramsay, E.A., Cunningham, C.H. and Plewes, D.B. (2009), Temporal stability of adaptive 3D radial MRI using multidimensional golden means. Magn. Reson. Med., 61: 354-363. https://doi.org/10.1002/mrm.21837
8. Mandava, S, Keerthivasan, MB, Martin, DR, Altbach, MI, Bilgin, A. Radial streak artifact reduction using phased array beamforming. Magn Reson Med. 2019; 81: 3915–3923. https://doi.org/10.1002/mrm.27689
9. Fu, Z, Johnson, K, Altbach, MI, Bilgin, A. Cancellation of streak artifacts in radial abdominal imaging using interference null space projection. Magn Reson Med. 2022; 88(3): 1355-1369. doi:10.1002/mrm.29285
Figures