2914
Phase-Resolved Functional Lung MRI Reveals Perfusion Abnormalities in Postacute COVID-19 Syndrome1Department of Radiology, Beijing Chaoyang Hospital, Capital Medical University, Beijing 100020, China, Beijing, China, 2Institute for Diagnostic and Interventional Radiology, Hannover Medical School, Hannover, Germany, Hannover, Germany, 3MR Research Collaboration, Siemens Healthineers, Beijing, China, Beijing, China
Synopsis
Keywords: Visualization, Lung
Motivation: The Pulmonary perfusion defects were unknown in post-acute COVID-19 syndrome (PACS).
Goal(s): To investigate the utility of phase-resolved functional lung (PREFUL) MRI in detecting pulmonary perfusion disturbances inPACS.
Approach: Participants diagnosed with PACS were recruited, along with healthy (NCT05933317). The quantified parameter QDP derived from PREFUL MRI represents abnormal pulmonary blood flow.
Results: 44 participants with PACS, and 43 healthy were assessed. QDP significantly exceeded healthy controls in PACS (39.81% ± 15.0% vs 8.2% ± 3.3%) and was notably higher in inpatients (46.8% ± 17.0% vs 34.5% ± 10.8%). Moreover, males exhibited higher QDP than females (43.9% ± 16.8% vs 34.4% ± 10.2%).
Impact: PREFUL MRI demonstrates notable perfusion defects in participants with PACS.
Introduction
Postacute COVID-19 syndrome (PACS) refers to persistent symptoms lasting beyond four weeks after SARS-CoV-2 infection1. Studies have confirmed the existence of persistent ventilatory impairment in PACS patients, but pulmonary perfusion injury in these patients has rarely been studied. Ventilation-perfusion single-photon emission computed tomography (V/Q–SPECT) is an important method for calculating lung perfusion, but it involves patient radiation exposure. Contrast-enhanced methods like dynamic contrast-enhanced MRI (DCE-MRI) also require contrast agents3. Phase-resolved functional lung MRI (PREFUL-MRI) is a radiation-free alternative that captures dynamic perfusion and ventilation parameters without contrast agents4. This study aims to assess lung function changes in PACS usingMethods
In the prospective study (ClinicalTrials.gov: NCT05933317), participants diagnosed with PACS were included. Meanwhile, healthy volunteers who had never been infected with COVID-19 were recruited. Pulmonary inflammation severity was quantified using a CT scoring system based on the extent of parenchymal involvement in each of the 5 lobes, with scores ranging from 0 (no involvement) to 5 (greater than 75% involvement), and the cumulative CT score ranged from 0 to 25. Free-breathing lung MRI was performed on a 3T MRI scanner (MAGNETOM Prisma; Siemens Healthcare, Erlangen, Germany) with specific parameters as described by Julian et al.5 The processed functional parameters perfusion defect percentage (QDP), ventilation defect percentage (VDP) and ventilation-perfusion non-defect match (VQM) were derived from PREFUL MRI (MATLAB, Hannover Medical School)6.Results
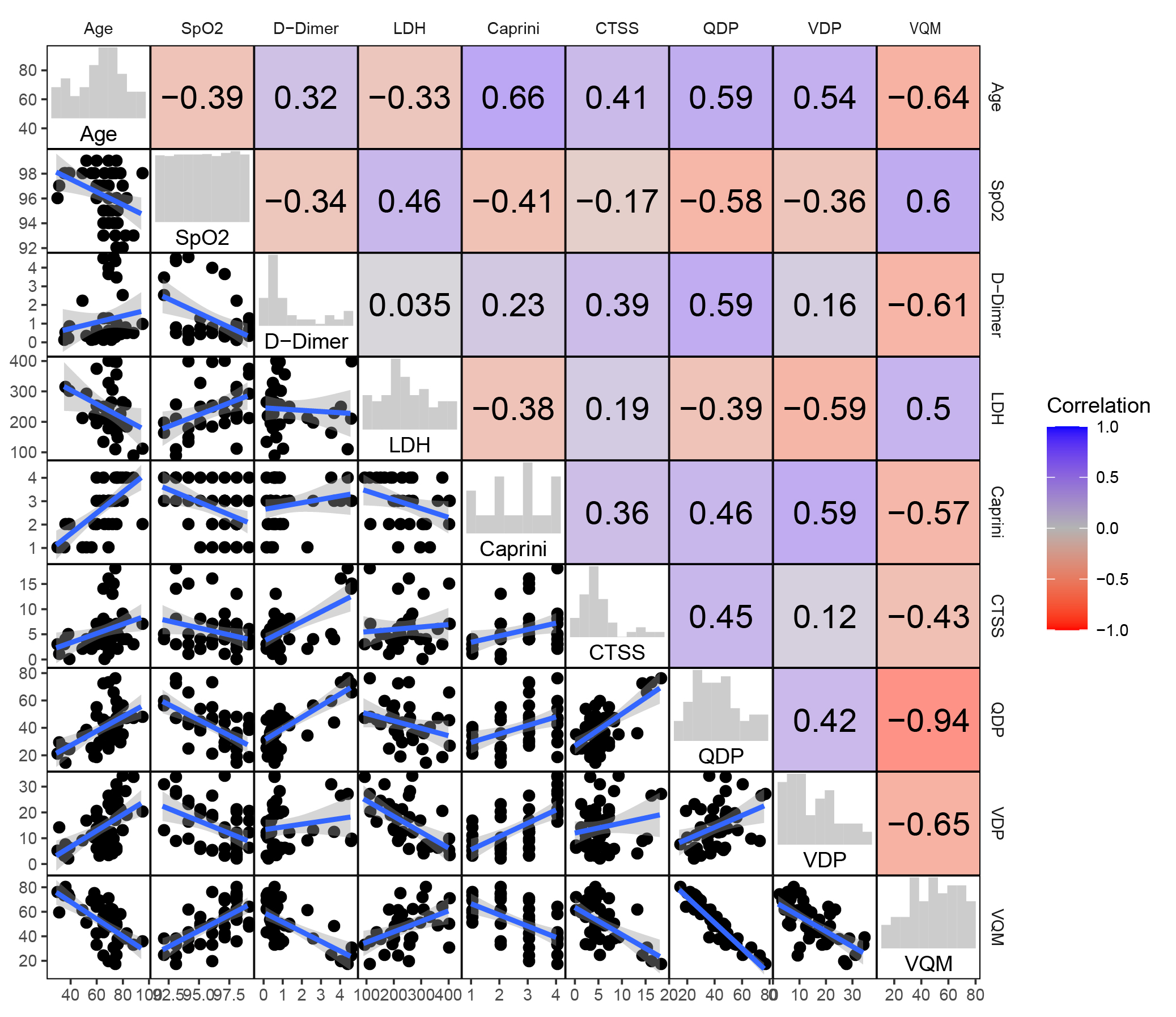
Finally, 44 participants with PACS, and a control group of 43 healthy volunteers were included. The mean interval between positive RT-PCR and MRI scans was 42.6 ± 6.3 days. Participants' mean age was 64.1 ± 15.1 years, with 43.2% females. 47.7% of participants received 3 doses of the COVID-19 vaccine, while 27.3% received no vaccine (Table 1). Lung parenchymal perfusion defects were significantly higher in participants with PACS (39.8% ± 15.0%) (Fig 1 and Fig 2). Comparison between PACS and healthy controls revealed that PACS patients had markedly higher perfusion defect percentages (39.81% ± 15.0% vs 8.2% ± 3.3%) and lower ventilation-perfusion match (VQM) (51.2% ± 16.6% vs 81.7% ± 4.9%) (Fig 3). Inpatients had higher perfusion defects (46.8% ± 17.0% vs 34.5% ± 10.8%) but lower VQM (44.8% ± 16.7% vs 54.1% ± 15.1%) compared to outpatients (Fig 3). A subgroup analysis based on sex showed that males had higher C-reactive protein (CRP) levels, CT severity scores, and perfusion defect percentages (QDP), but lower VQM compared to females (Fig 4). Participants with dyspnea (26 out of 44) were older, had lower oxygen saturation levels, higher D-dimer levels, higher QDP (44.8% ± 15.8% vs 32.6% ± 10.3%), and lower VQM (45.9% ± 17.2% vs 58.8% ± 12.6%) than those without dyspnea (Fig 4). Correlations were observed between PREFUL MRI-derived parameters and various clinical factors. QDP positively correlated with age, CT score, D-dimer level, and Caprini score but negatively correlated with oxygen saturation (SpO2) and lactate dehydrogenase (LDH) levels. Ventilation defect percentage (VDP) positively correlated with age and Caprini score but negatively correlated with SpO2 and LDH levels. VQM negatively correlated with age, CT score, D-dimer level, and Caprini score but positively correlated with SpO2 and LDH levels (Fig 5).Discussion
PREFUL MRI, a contrast-free technique, has been effective in detecting lung pathology. Previous studies also highlighted its utility in assessing impaired lung function post-COVID-19 infection7. The study's findings aligned with these, indicating vascular or structural abnormalities in PACS participants, particularly with significantly higher perfusion defects than healthy individuals. Gender disparities in COVID-19 pathology were observed, with males displaying higher perfusion defects possibly due to increased vasoconstriction in male patients. Dyspnea, a prevalent symptom during and after COVID-19, was associated with more pronounced perfusion defects, suggesting microcirculation and alveolar membrane impact in post-COVID patients with respiratory distress. The study also correlated perfusion defects with clinical markers such as D-dimer levels, Caprini score, and oxygen saturation, supporting microvascular thrombosis/injury and inflammation as underlying mechanisms.Conclusions
This study highlighted the presence of persistent pulmonary dysfunction, specifically perfusion defects, in individuals with PACS, as demonstrated by PREFUL MRI. Additionally, our findings suggest notable pathophysiological differences in lung perfusion among participants of different sexes and those with or without dyspnea. Future longitudinal studies will seek to determine the temporal progression of pulmonary vascular abnormalities and their potential as prognostic indicators for the long-term outcomes of COVID-19 patients.Summary of Main Findings
PREFUL MRI demonstrates notable pulmonary perfusion defects in participants with postacute COVID-19 syndrome. Furthermore, perfusion impairments are more pronounced in males, inpatients, and dyspneic participants.Acknowledgements
NAReferences
1. Nalbandian A, Sehgal K, Gupta A, et al. Post-acute COVID-19 syndrome. Nat Med 2021; 27(4): 601-15. 2. Chopra V, Flanders SA, O'Malley M, Malani AN, Prescott HC. Sixty-Day Outcomes Among Patients Hospitalized With COVID-19. Annals of internal medicine 2021; 174(4): 576-8. 3. Yu JZ, Granberg T, Shams R, et al. Lung perfusion disturbances in nonhospitalized post-COVID with dyspnea-A magnetic resonance imaging feasibility study. Journal of internal medicine 2022; 292(6): 941-56. 4. Voskrebenzev A, Gutberlet M, Klimeš F, et al. Feasibility of quantitative regional ventilation and perfusion mapping with phase-resolved functional lung (PREFUL) MRI in healthy volunteers and COPD, CTEPH, and CF patients. Magnetic resonance in medicine 2018; 79(4): 2306-14. 5. Glandorf J, Klimeš F, Voskrebenzev A, et al. Comparison of phase-resolved functional lung (PREFUL) MRI derived perfusion and ventilation parameters at 1.5T and 3T in healthy volunteers. PloS one 2020; 15(12): e0244638. 6. Pöhler GH, Klimeš F, Behrendt L, et al. Repeatability of Phase-Resolved Functional Lung (PREFUL)-MRI Ventilation and Perfusion Parameters in Healthy Subjects and COPD Patients. Journal of magnetic resonance imaging : JMRI 2021; 53(3): 915-27. 7. Levy S, Heiss R, Grimm R, et al. Free-Breathing Low-Field MRI of the Lungs Detects Functional Alterations Associated With Persistent Symptoms After COVID-19 Infection. Investigative radiology 2022; 57(11): 742-51.Figures