2912
Acute disease severity is associated with increased pulmonary perfusion transit times at follow-up in male patients hospitalised with COVID-19.1The University of Sheffield, Sheffield, United Kingdom, 2National Institute for Health Research (NIHR) Sheffield Biomedical Research Centre (BRC), Sheffield Teaching Hospitals, Sheffield, United Kingdom, 3University of Leicester, Leicester, United Kingdom, 4Full group details can be found in Appendix 1 of https://doi.org/10.1016/S2213-2600(21)00383-0, Sheffield, United Kingdom, 5University of Oxford, Oxford, United Kingdom
Synopsis
Keywords: Lung, COVID-19
Motivation: Perfusion disturbances can be observed up to a year after acute COVID-19 infection.
Goal(s): Evaluate the relationship between pulmonary perfusion and sex, age and disease severity in patients hospitalised due to COVID-19.
Approach: 198 patients hospitalised due to COVID-19 were recruited from 13 centres as part of the C-MORE study. 3T dynamic contrast enhanced lung perfusion imaging was acquired at follow-up.
Results: Men previously hospitalised with severe COVID-19 showed increased pulmonary mean transit time (MTT) and more heterogenous pulmonary MTT at follow up compared to men with less severe disease. Disease severity was not associated with increased MTT at follow up in women.
Impact: Dynamic contrast enhanced lung perfusion imaging can identify prolonged pulmonary transit times in patients hospitalised due to COVID-19 and demonstrates that at patient follow-up pulmonary perfusion depends on patient sex, age and, in male patients, acute disease severity.
Introduction
Patients with acute COVID-19 infection typically present with ground glass opacities and consolidation. Various perfusion disturbance patterns have been observed including pulmonary thromboembolism, reduced perfusion in the presence of ground glass opacities, and hyperperfusion in the presence of COVID-19 lesions1-3. Perfusion disturbances have been observed up to and beyond a year after acute COVID-19 infection, including both hypoperfusion and hyperperfusion3-5.A previous study of non-hospitalized patients suggested sex-based differences in pulmonary transit time and confirm that male patients are at a higher risk of severe clinical outcomes5. It has been widely reported that male patients have a higher risk for severe COVID-19, ICU admission and death6.
The recently published C-MORE study of patients hospitalised due to COVID-19 5 months after hospitalisation did not find a significant difference in global pulmonary blood flow, volume and mean transit time between controls and patients7.
In this work, we aim to evaluate the relationship between pulmonary perfusion and sex, age and disease severity in patients who were hospitalised due to COVID-19.
Methods
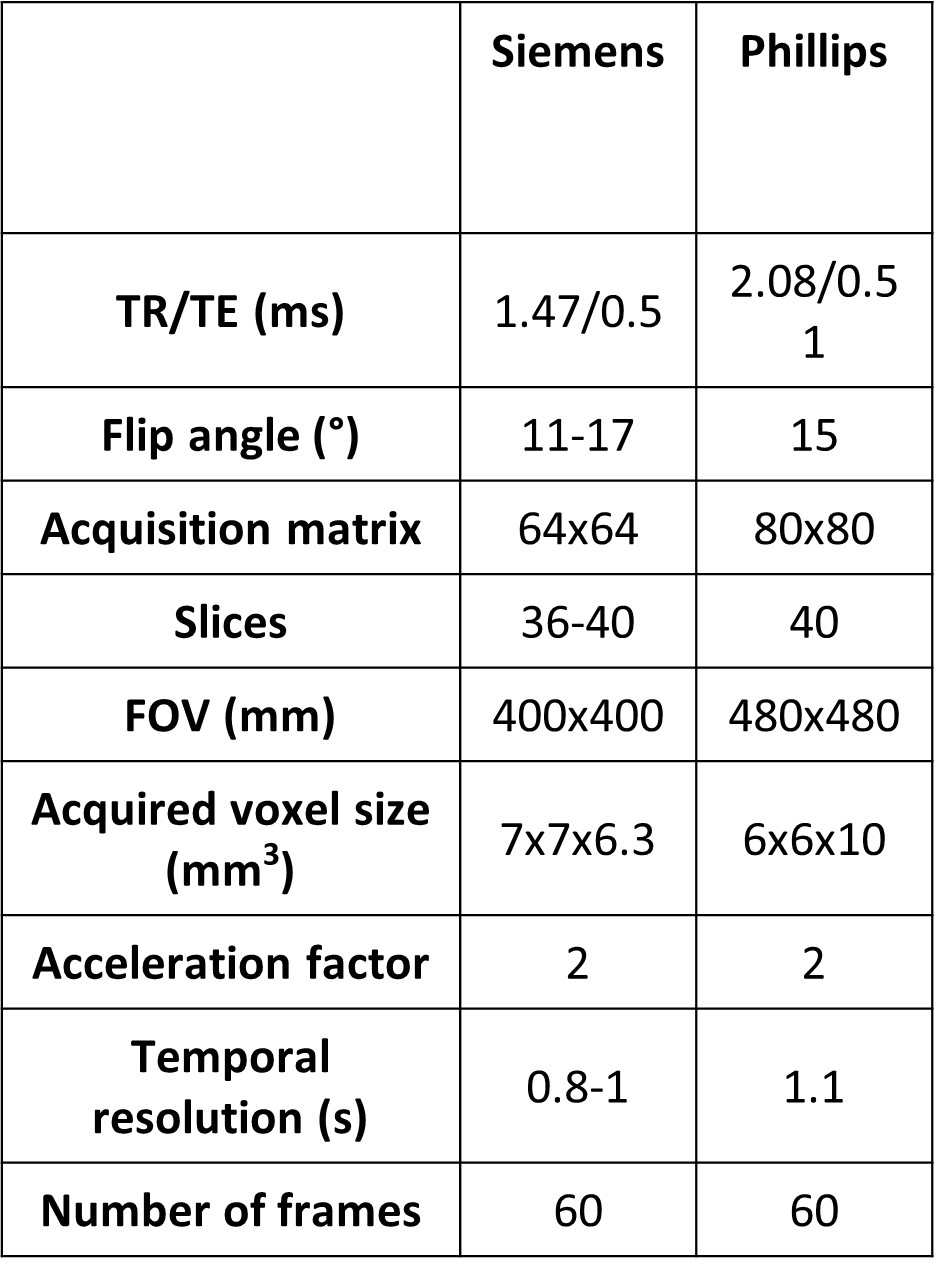
Subjects were recruited from 13 centres as part of the C-MORE study7 and MR imaging was acquired at 3T using the same acquisition protocol (Table 1).Perfusion images were co-registered to correct for patient motion using ANTs software8. Semi-quantitative maps of relative pulmonary blood volume (rPBV), relative pulmonary blood flow (rPBF) and mean transit time were calculated9. Semi-automated segmentations excluding main pulmonary vessels were applied to the maps.
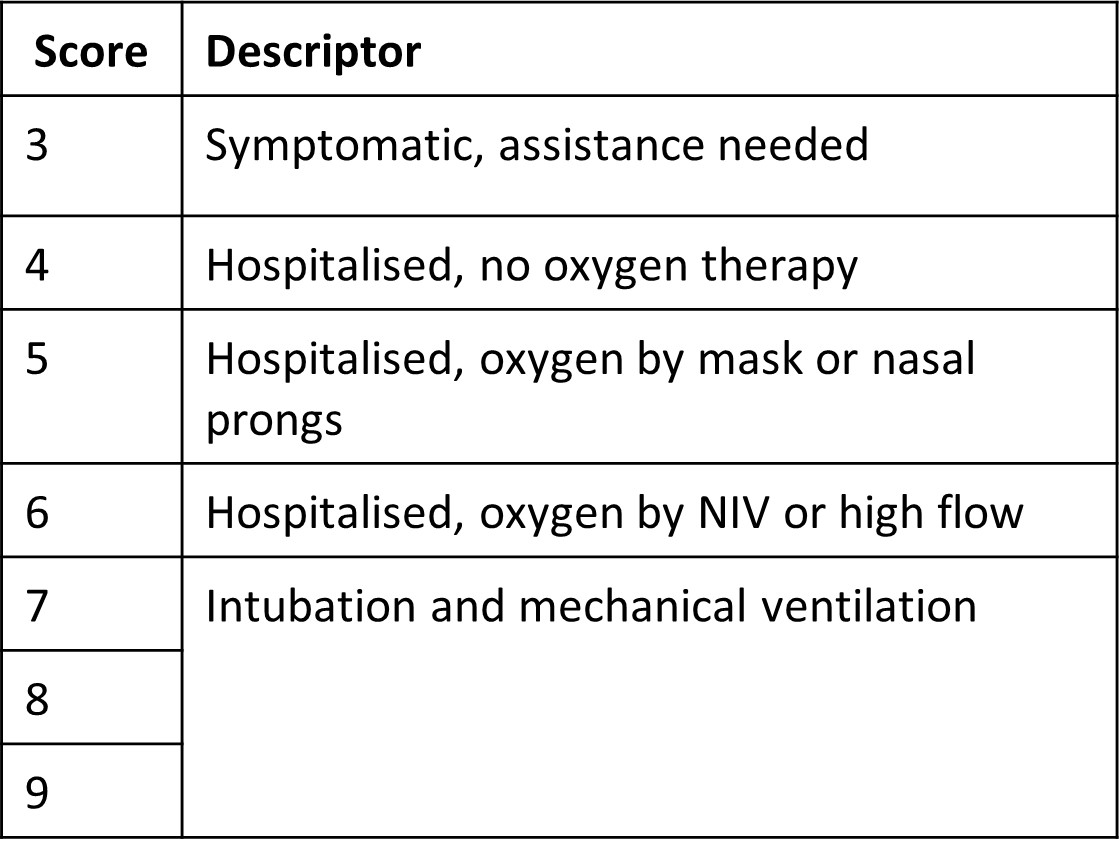
WHO Clinical Progression Scale10 (“WHO score”) and admission duration were used as markers of disease severity (Table 2).
Mann-Whitney U Tests were used to evaluate whether perfusion metrics depended on sex, and for cases with a significant result subsequent analysis was undertaken separately for each sex. Categorical variables were tested for sex differences using a chi-squared test of independence.
Independent-Samples Kruskal-Wallis Tests were used to evaluate whether perfusion metrics varied with WHO score with a Bonferroni correction applied to post-hoc tests. Linear regression modelling with hospitalisation duration and age was used to evaluate the relationship between hospital duration and pulmonary perfusion metrics. Spearmans’ correlation coefficient was used to assess correlations.
Results
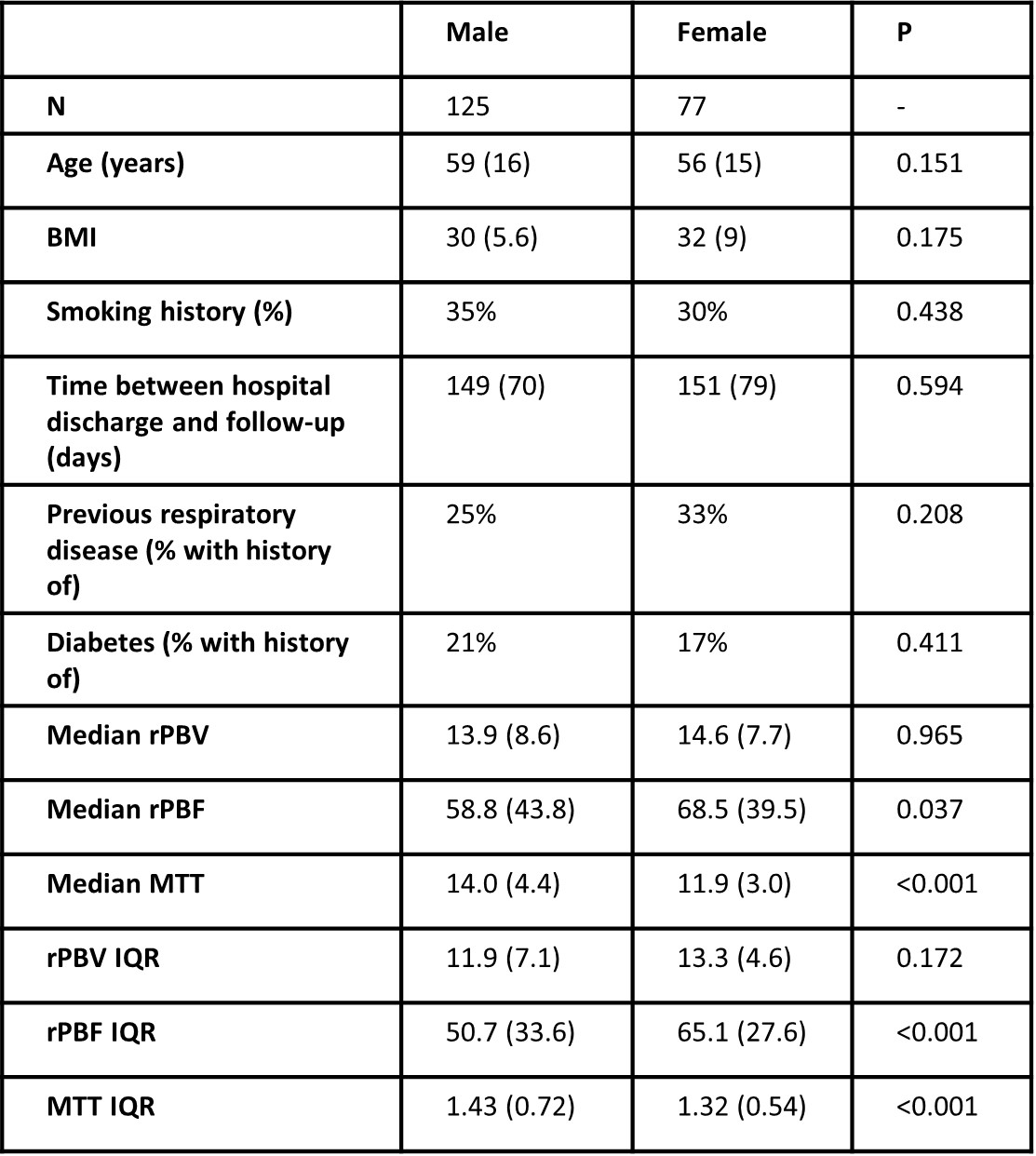
198 patients were identified with successful pulmonary perfusion imaging and analysis (WHO score 3-4: n=36, WHO score 5: n=105; WHO score 6: n=43; WHO score 7-9: n=14). Median hospital duration was 6 days (range 0-157, n=199) and median follow up time was 151 days (range: 81-653).Mean transit time was significantly shorter and pulmonary blood flow was significantly higher in female patients compared to male patients (p<0.001, p=0.037, Table 3).
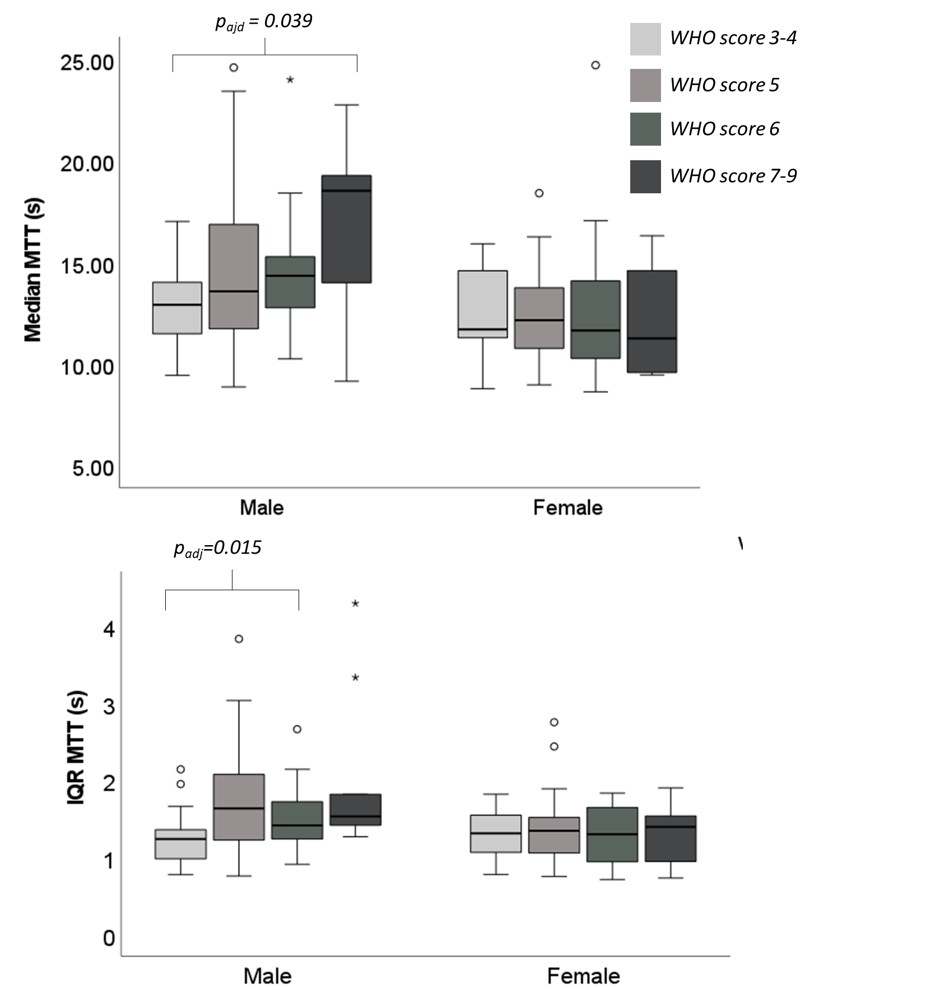
Male patients with WHO score 7-9 had significantly longer MTT than those with WHO score 3-4, see Figure 1. Male patients with WHO score 5 had more heterogeneity in MTT (IQR MTT) than those with WHO score 3-4. No other significant changes with WHO score in perfusion metrics were found.
In male patients, age and admission duration were significant predictors of MTT according to the equation MTT = 10.3 + 0.066*age + 0.053*admission duration (p=0.011, p=0.005). For MTT IQR, rPBV and rPBF age was a significant predictor, but admission duration was not. rPBV IQR and rPBF IQR were not dependent on age or admission duration.
In female patients, neither age nor admission duration were significant predictors of MTT, rPBV, rPBF, rPBV IQR or rPBF IQR. Age was a significant predictor of MTT IQR.
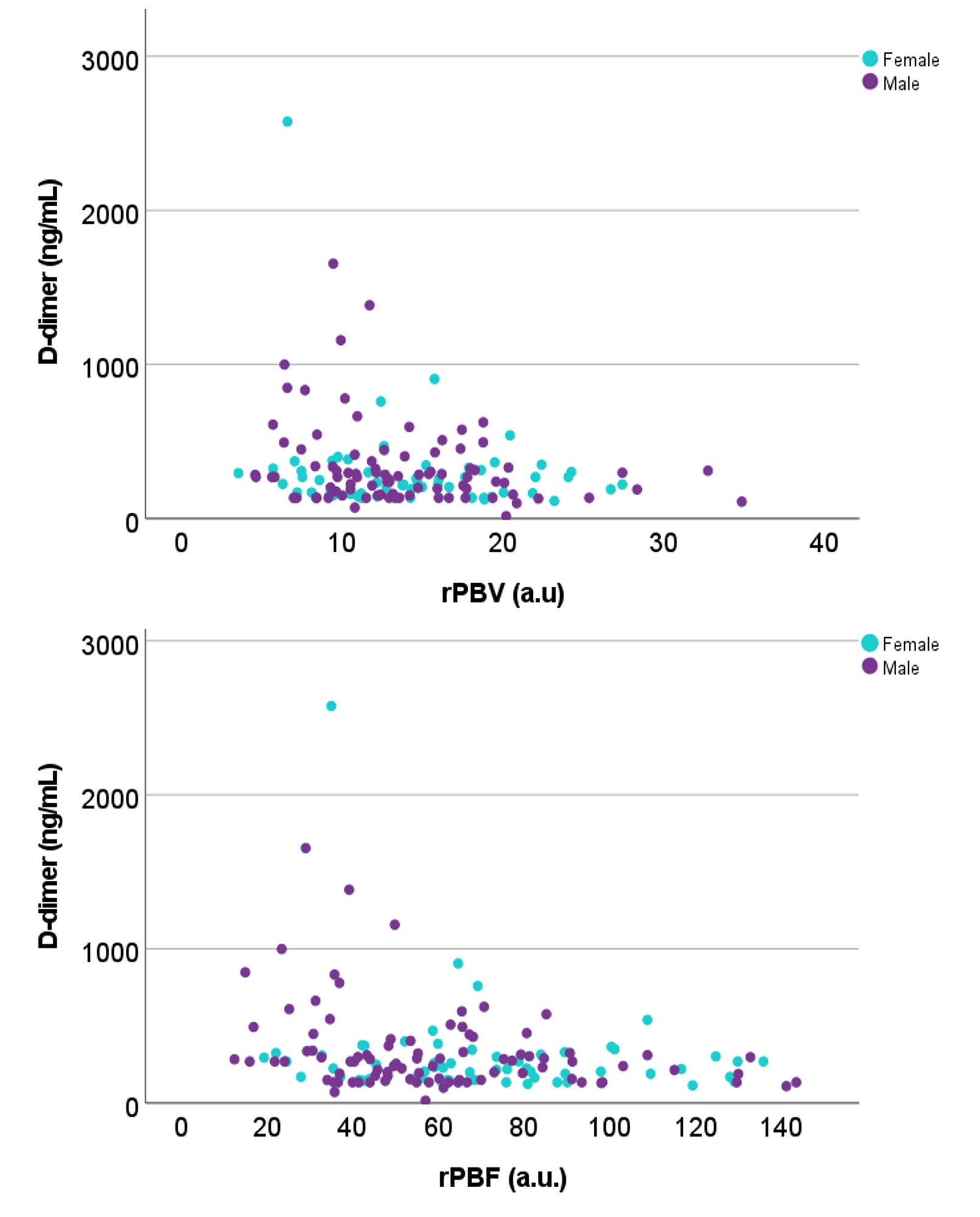
D-dimer measured at follow-up correlated significantly with rPBV (r=-0.188, p=0.022), rPBF (r=-0.255, p=0.006) but not MTT (r=0.150, p=0.069).
Discussion
These results indicate that there may be sex-based differences in pulmonary perfusion measures in patients previously hospitalised with COVID-19. Male patients with more severe disease exhibit increased pulmonary transit times (MTT), even after adjusting for age related changes.This is consistent with previous reports of sex differences in non-hospitalised patients with persistent symptoms after COVID-195. By contrast, women with more severe illness did not show prolonged pulmonary transit times at follow up. While the reasons for this are not clear, possible explanations include differences in hormonal variations, immune response or residual lung abnormality.
Follow-up rPBV or rPBF was not associated with acute disease severity, indicating that perfusion abnormalities in patients with severe COVID-19 are not due to large perfusion defects which would be expected to reduce rPBV and increase rPBV IQR.
Conclusion
Men previously hospitalised with severe COVID-19 showed increased pulmonary MTT and more heterogenous pulmonary MTT at follow up compared to men with less severe disease. Disease severity was not associated with increased MTT at follow up in women.Acknowledgements
National Institute of Health Research (NIHR) (NIHR-RP-R3-12-027), the Medical Research Council (MR/M008894/1) and C-MORE/PHOSP-COVID (MR/V027859/1 and COV0319) for funding. BR is supported by BHF Oxford CRE (RE/18/3/34214). NIHR BRC Im Eng theme. INSIGNEO. This study/research is funded by the National Institute for Health and Care Research (NIHR) Sheffield Biomedical Research Centre (NIHR203321). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care. Radiographic and administration teams at all sites.References
1. Karamian F, Sadeghi R, Askari E. Lung Ventilation-Perfusion Scan in COVID-19: Various Patterns of Perfusion Defects. Clin Nucl Med. May 1 2023;48(5):e239-e243. doi:10.1097/RLU.0000000000004545
2. Lang M, Som A, Mendoza DP, et al. Hypoxaemia related to COVID-19: vascular and perfusion abnormalities on dual-energy CT. Lancet Infect Dis. Dec 2020;20(12):1365-1366. doi:10.1016/S1473-3099(20)30367-4
3. Mohamed I, de Broucker V, Duhamel A, et al. Pulmonary circulation abnormalities in post-acute COVID-19 syndrome: dual-energy CT angiographic findings in 79 patients. Eur Radiol. Jul 2023;33(7):4700-4712. doi:10.1007/s00330-023-09618-9
4. Evbuomwan O, Endres W, Tebeila T, Engelbrecht G. Identification and Follow-up of COVID-19 Related Matching Ventilation and Perfusion Defects on Functional Imaging Using VQ SPECT/CT. Nucl Med Mol Imaging. Feb 2023;57(1):9-15. doi:10.1007/s13139-022-00776-0
5. Yu J, Granberg T, Shams R, et al. Lung Perfusion Disturbances Detected with MRI in Non-Hospitalized Post-COVID-19 Individuals with Dyspnea 3 -13 Months after the Acute Disease. medRxiv. 2022:2022.01.25.22269717. doi:10.1101/2022.01.25.22269717
6. Pijls BG, Jolani S, Atherley A, et al. Temporal trends of sex differences for COVID-19 infection, hospitalisation, severe disease, intensive care unit (ICU) admission and death: a meta-analysis of 229 studies covering over 10M patients. F1000Res. 2022;11:5. doi:10.12688/f1000research.74645.1
7. Group CMP-CC. Multiorgan MRI findings after hospitalisation with COVID-19 in the UK (C-MORE): a prospective, multicentre, observational cohort study. Lancet Respir Med. Sep 22 2023;doi:10.1016/S2213-2600(23)00262-X
8. Avants BB, Tustison NJ, Song G, Cook PA, Klein A, Gee JC. A reproducible evaluation of ANTs similarity metric performance in brain image registration. Neuroimage. Feb 1 2011;54(3):2033-44. doi:10.1016/j.neuroimage.2010.09.025
9. Levin DL, Chen Q, Zhang M, Edelman RR, Hatabu H. Evaluation of regional pulmonary perfusion using ultrafast magnetic resonance imaging. Magn Reson Med. Jul 2001;46(1):166-71. doi:10.1002/mrm.1172
10. Characterisation WHOWGotC, Management of C-i. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect Dis. Aug 2020;20(8):e192-e197. doi:10.1016/S1473-3099(20)30483-7
Figures