2910
Adaptation of lung mechanics during constrained breathing using 3D MRI spirometry1Université Paris-Saclay, CEA, CNRS, Inserm, BioMaps, Zoteux, France, 2Université Paris-Saclay, CEA, CNRS, Inserm, BioMaps, Orsay, France, 3Hôpital Bicêtre, APHP, Le Kremlin-Bicêtre, France, 4GE Healthcare, Buc, France
Synopsis
Keywords: Lung, Lung, Spirometry, biomarkers, biomechanical
Motivation: New mechanical biomarkers to characterize lung pathophysiology using 3D MR spirometry.
Goal(s): To investigate the dynamics of lung elongations along the three anatomical directions when the lungs are constrained during breathing.
Approach: 3D MR spirometry was performed in 25 healthy volunteers spontaneously breathing and in a healthy volunteer for three types of breathing (spontaneous, thoracic, diaphragmatic).
Results: The main respiratory driving force is produced by the diaphragm as it is assessed here with a dominant superior-inferior normal strain in basal pulmonary regions. In spontaneous breathing, it is supplemented mainly by the anterior-posterior normal strain in the apical regions.
Impact: Dynamic normal strains are original mechanical biomarkers that provide new insight on the regional anisotropic behaviour of the lungs.
Introduction
Three-dimensional MR spirometry produces local flow-volume loops across an average respiratory cycle integrated over a 12 min dynamic lung MRI acquisition [1]. Lung function can then be regionally characterized along the lines of standard spirometry, which is routinely performed but only limited to a global measurement at the subject’s mouth in forced respiration. Additional markers can further be extracted from 3D MR spirometry to track the dynamic biomechanical behaviour of the lung. The Green-Lagrange strain tensor was evaluated between the 32 processed respiratory phases. It diagonally contains the directional dilatations, which allows us to calculate deformation in all three directions.Methods
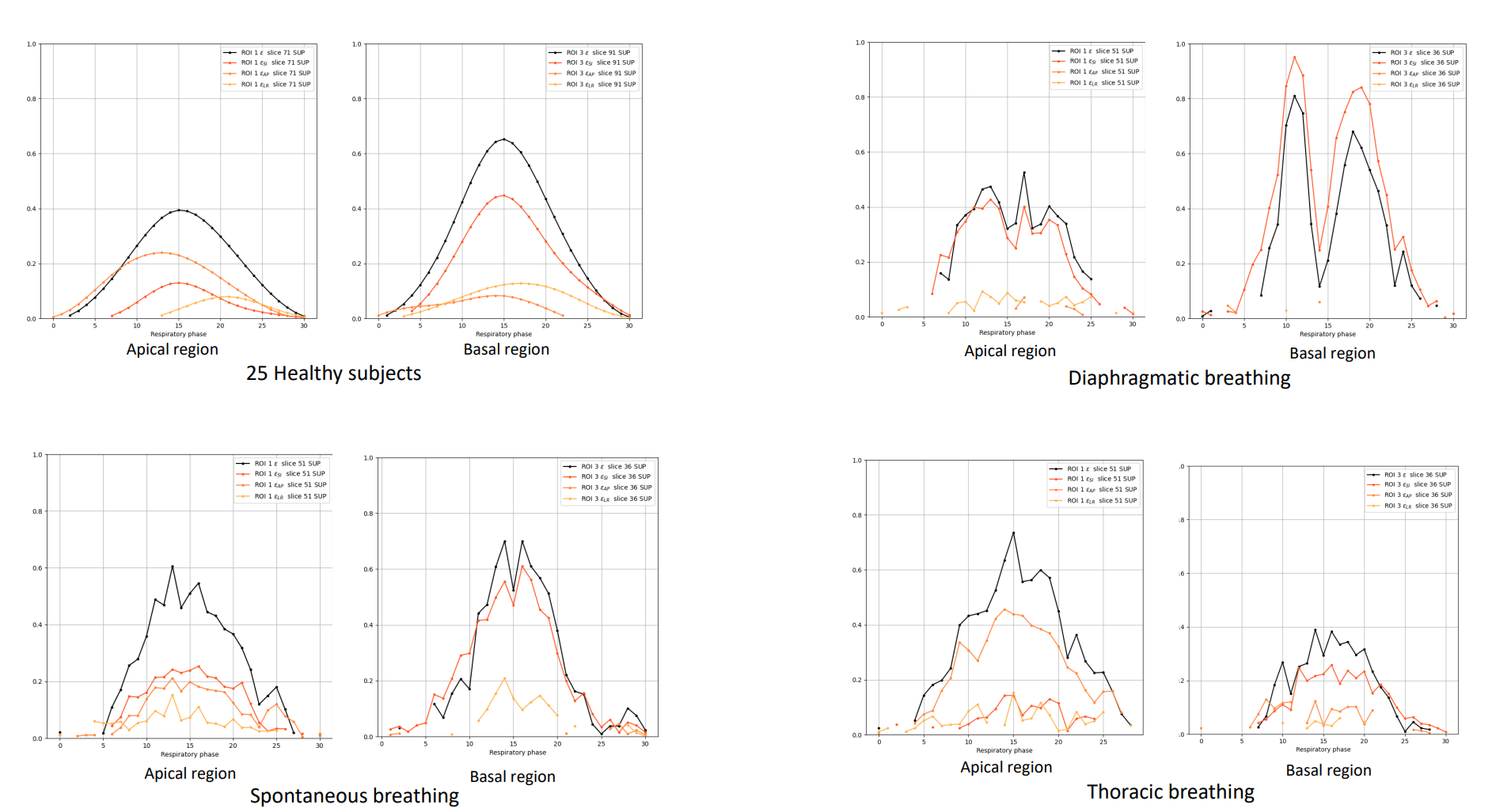
MR acquisitions were carried on a cohort of 25 subjects freely-breathing in supine position in a GE Signa PET/MR at 3 T using a 3D UTE sequence with AZTEK [2] and a 30-channel thoracic coil array. Acquisitions were also performed on a healthy subject for three modes of breathing (spontaneous, diaphragmatic and thoracic) governed by a sound metronome set at 20 beats/min. The centre of the acquired k-space was used as a surrogate respiratory signal to retrospectively rephase MR data to reconstruct 32 3D lung dynamic images over the acquisition-integrated respiratory cycle. The dynamic Green-Lagrange strain tensor was inferred at each respiratory phase from the deformation fields after elastic registration to the beginning of inspiration reference phase. The maps of the compressive strain tensor diagonal elements (or normal strains) along the three anatomical directions (superior-inferior, SI, anterior-posterior, AP, and left-right, LR) were then morphology- and histogram-based normalized before computing mean maps over the volunteers across the 32 respiratory phases for analysis. ROIs of (5×5×5) voxels were selected throughout the lung to probe the evolution of the normal strains and the sum, ɛ, over the respiratory cycle. Data consistancy was checked between the cadenced and free breathing acquisitions.Results
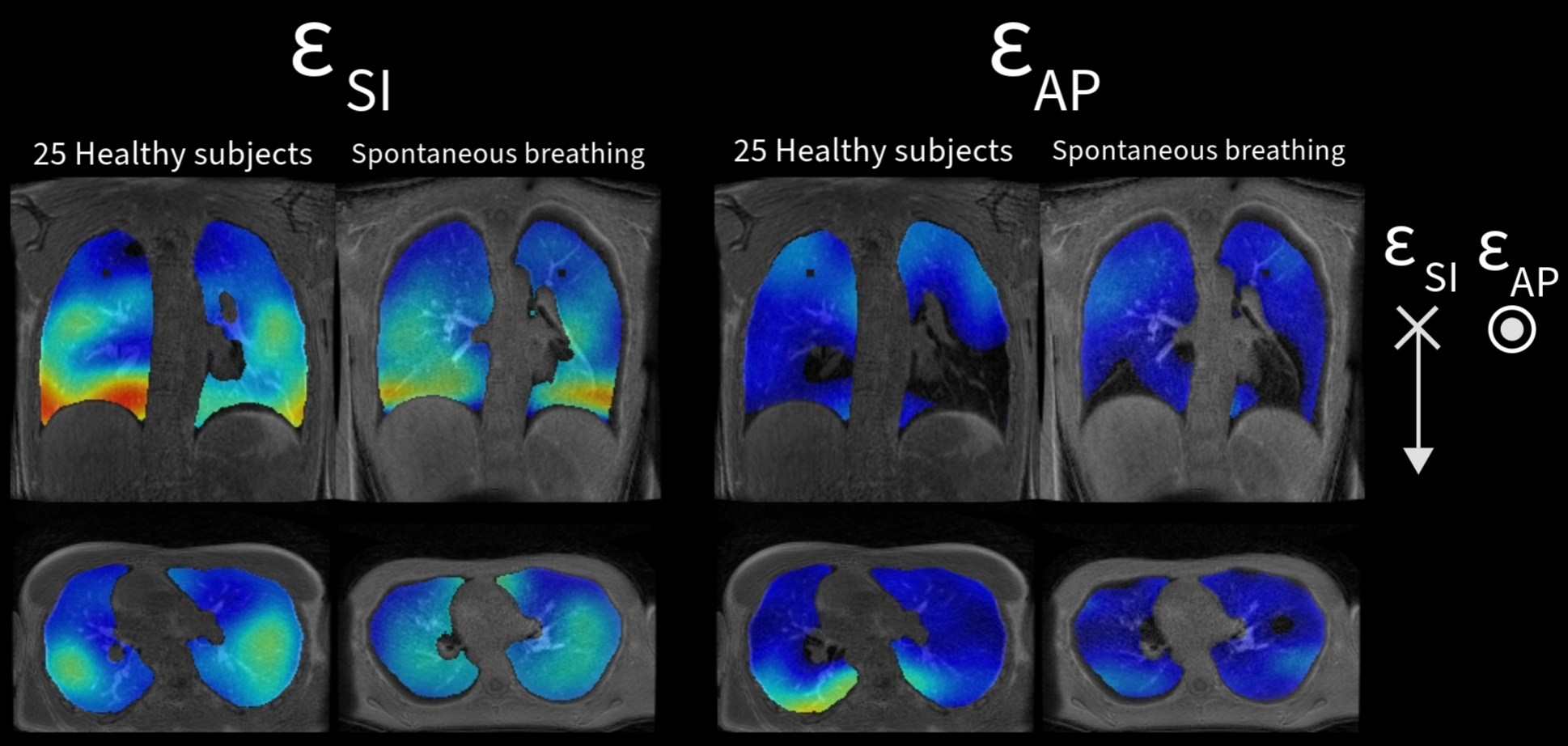
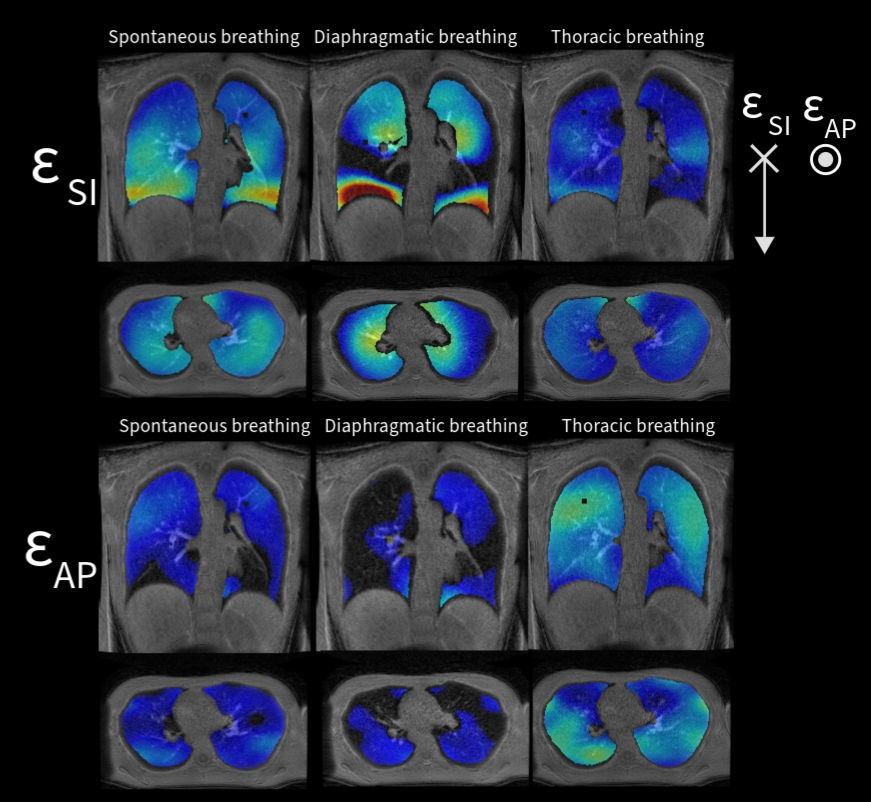
3D Maps of normal strains are shown in Figure 1 for SI. Mean values and standard deviations were <ɛSI>25 =(0.128±0.050), <ɛSI>cad=(0.105±0.050) and <ɛAP>25=(0.049±0.033) and < ɛAP >cad=(0.058±0.029). In the SI direction, lung deformation mainly takes place in the basal regions, close to the diaphragm. In the AP direction, deformation takes place in the posterior apical regions. Diaphragmatic breathing involves almost two-third as much deformation as spontaneous breathing does in the SI direction. In the AP direction, thoracic breathing involves twice as much deformation as thoracic breathing does. Over a respiratory cycle, the SI component reaches its maximal value before the AP component in most of the lungs but it is reverse in the apical regions.Discussion
In supine position, the subject is free to move the thorax. Yet, the diaphragm remains the driving force in spontaneous breathing: lung elongation mainly occurs along SI but in the apical regions. For cadenced acquisitions, breathing is slightly forced and therefore less spontaneous.Conclusion
Numerous parametric maps can be extracted from 3D MR spirometry. The normal strains provide rich spatial and temporal information on the biomechanical function of the lung. They are comprehensive and sensitive parameters which characterize the respiratory function and its adaptation to conditions. They might also explicit the lung dysfunction when muscles are impaired or more generally in most respiratory pathology when the lung function is altered and the volume changes are modified at the regional level. A temporal approach to these mechanical biomarkers could make it possible to diagnose pathologies at the voxel level and to know at what point in the breathing process the disease manifests itself.Acknowledgements
No acknowledgement found.References
[1] Boucneau T, Fernandez B, Larson P, Darrasse L, Maître X. 3D Magnetic Resonance Spirometry. Scientific Reports. 2020;10(1):9649. doi:10.1038/s41598-020-66202-7
[2] Boucneau T, Fernandez B, Besson FL, Menini A, Wiesinger F, Durand E, Caramella C, Darrasse L, Maître X. AZTEK: Adaptive zero TE k-space trajectories. Magnetic Resonance in Medicine. 2021;85(2):926-935. doi:https://doi.org/10.1002/mrm.28483
[3] Yang X, Sun H, Deng M, Chen Y, Li C, Yu P, Zhang R, Liu M, Dai H, Wang C. Characteristics of Diaphragmatic and Chest Wall Motion in People with Normal Pulmonary Function: A Study with FreeBreathing Dynamic MRI. Journal of Clinical Medicine. 2022;11(24):7276. doi:10.3390/jcm11247276
Figures