2906
Lung MRI Screening protocol at 0.55T: Initial Experience in Healthy Volunteers1Department of Radiology and Biomedical Imaging, Univeristy of California, San Francisco, San Francisco, CA, United States, 2Department of Radiation Oncology, Univeristy of California, San Francisco, San Francisco, CA, United States
Synopsis
Keywords: Lung, Low-Field MRI
Motivation: The current clinical standard for screening lung imaging is chest CT, which is associated with radiation exposure and only provides static, anatomical information of the lung and concurrently imaged heart.
Goal(s): We are exploring an alternative method for lung pathology screening.
Approach: Using a 0.55T MRI scanner and the proposed screening Lung MRI protocol, we conducted lung MRI scans on 10 healthy volunteers.
Results: Initial assessments demonstrate concurrent evaluation of the anatomy, motion, and tissue characteristics of the lung and heart in around 25 minutes.
Impact: We propose a screening Lung MRI protocol as a potential alternative imaging option in screening as well as follow up imaging in particular conditions, with the benefit of eliminating radiation dose and additional respiratory and cardiac motion and tissue information
Introduction
The introduction of a 0.55T scanner with improved lung MR imaging presents an unprecedented opportunity to explore the clinical utility of lung MRI in screening. Unlike traditional lung MRI, which has limited use in initial and follow-up evaluations, such as cystic fibrosis, lung cancer staging, and lung nodule characterization according to the Fleischner Society1,2, this enhanced technology offers advantages over CT by avoiding radiation exposure, providing information on respiratory motion, ventilation, and perfusion, and offering valuable tissue characterization abilities in lesion detection3. Additionally, a screening MRI can include basic cardiac sequences recently proven comparable to 1.5T4 to detect associated heart abnormalities, especially useful in conditions where the lung and heart interact or coexist, such as heart failure, interstitial lung disease, and cancer therapy-induced issues. This study presents preliminary observations from a screening lung MR protocol with basic cardiac sequences.Methods
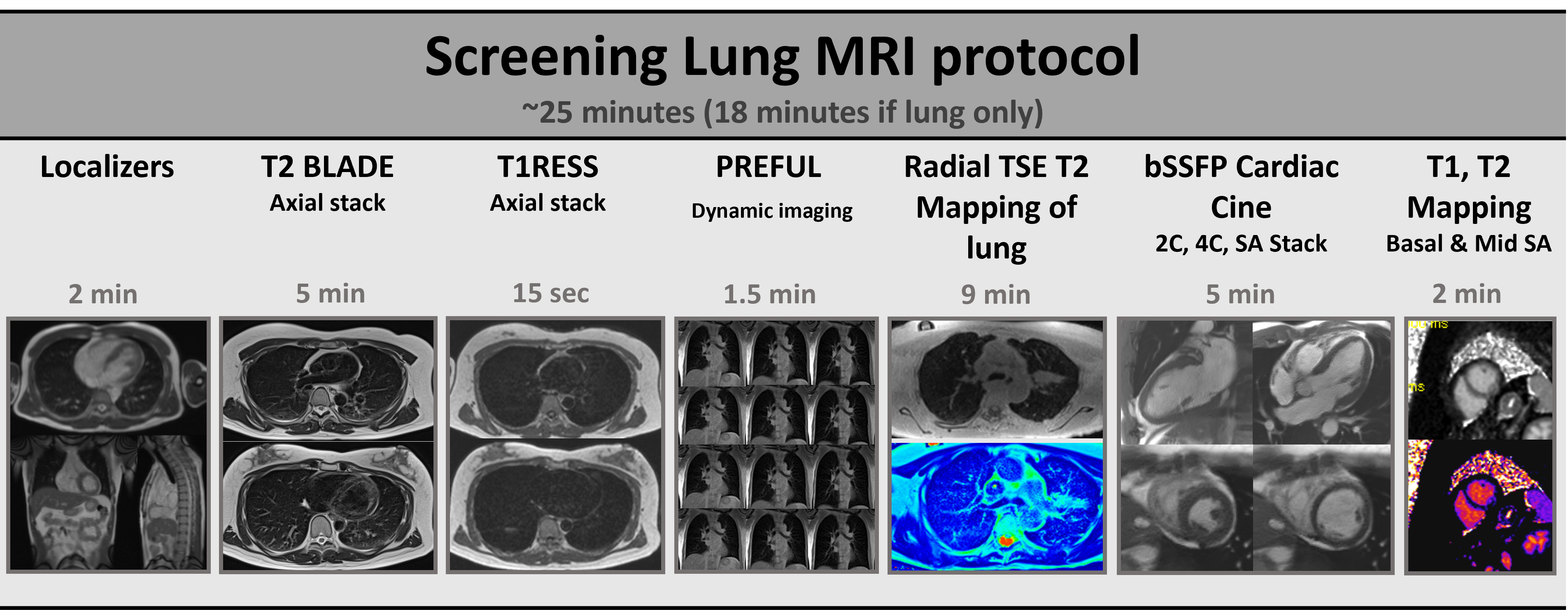
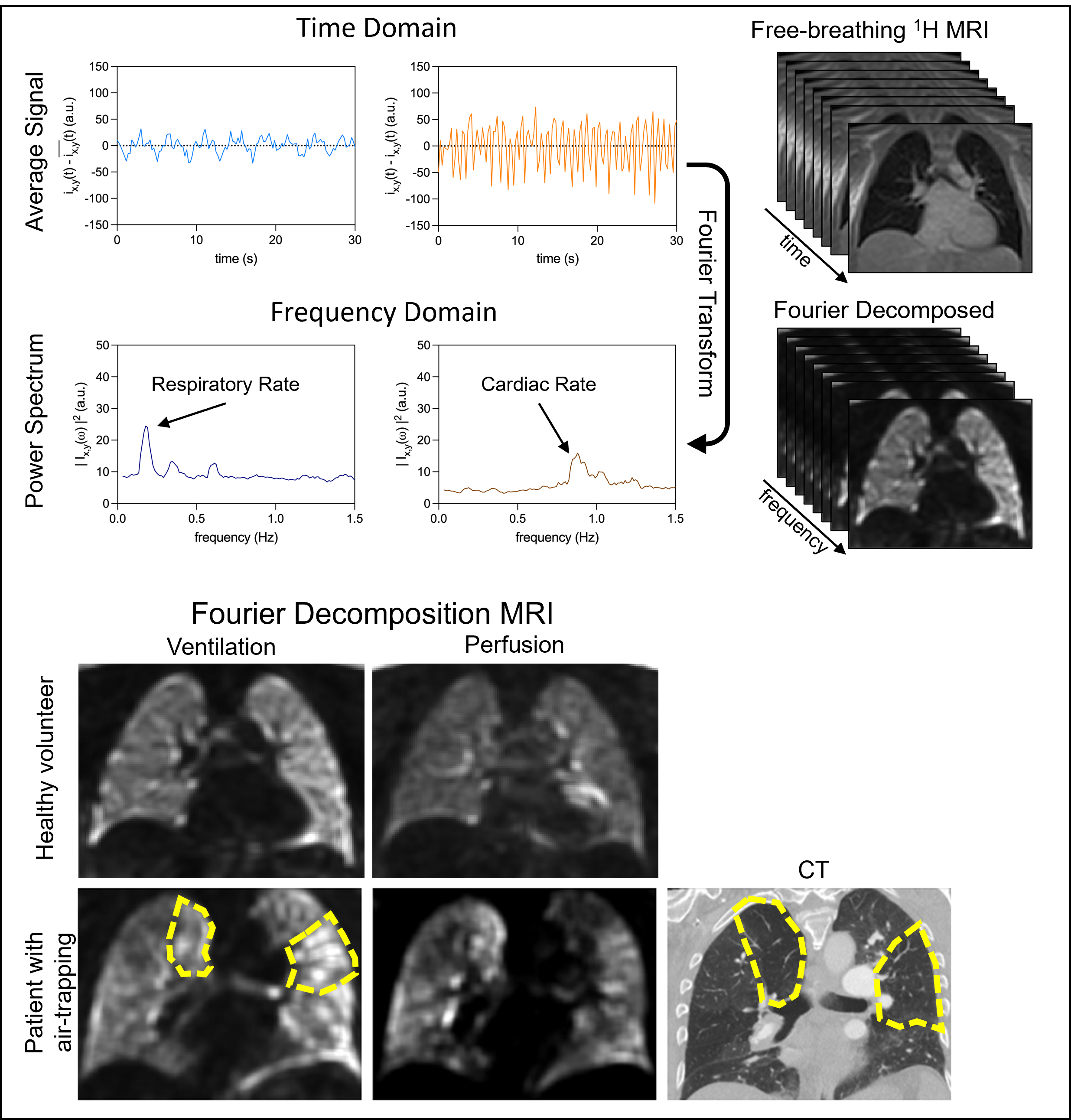
Lung MRIs were obtained on 10 healthy volunteers (5 women, 5 men) with an average age of 43.5 (range 23-64) using a 0.55T Siemens Free.Max scanner. Per protocol, free breathing lung and basic breath-held cardiac sequences were acquired without contrast.Respiratory-navigated T2 BLADE (1.2x1.2mm in-plane spatial resolution, 6mm slice thickness, 40 slices, TE = 94ms, TR = 2.5s.) was acquired for anatomical evaluation of the lung. T1RESS5 (1.3x1.3mm in-plane spatial resolution, 4mm slice thickness, 40 slices, TE = 1.97ms, TR = 553ms) was acquired in a single breath hold. Dynamic Coronal PREFUL/Fourier decomposition (FD) 1H MRI (FDMRI)6 (2x2 mm in-plane resolution after 2 x interpolation, 15mm slice thickness, TE=1.33ms, TR=231.3ms with 272 phases) was acquired during multiple respiratory cycles, which was grossly evaluated for the motion of the diaphragm. Ventilation and perfusion images were also generated using computational methods to extract functional information from the observed parenchymal signal intensity changes. Respiratory-navigated Axial Radial TSE T2 mapping7 (1.3x1.3 mm, 6mm slice thickness, 36 slices, starting TE=10ms, with the turbo factor of 32 and echo spacing of 10.1ms, TR = 2.33s) was acquired, which was then measured within the right mid lung parenchyma.
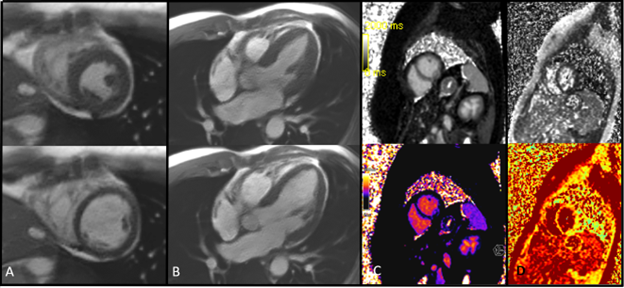
For the Cardiac cine imaging, a retrospectively gated balanced SSFP was employed (1.4x1.4x8 mm with a temporal resolution of 35ms). Additionally, we included the MOLLI 5-3-3 T1 mapping (1.9x1.9x8 mm) and T2 mapping with T2 preparation time of 0, 25, and 55ms (1.9x1.9x8mm). Both native T1 and T2 values were recorded. Chamber size and morphology were evaluated from the cine imaging. The left ventricular ejection fraction (LVEF) was calculated from the short axis cine using Medis QMass Software. Image quality was assessed by two board-certified radiologists, using a 5-point Likert scale (1: poor, 5: fully diagnostic) for visual evaluations.
Results
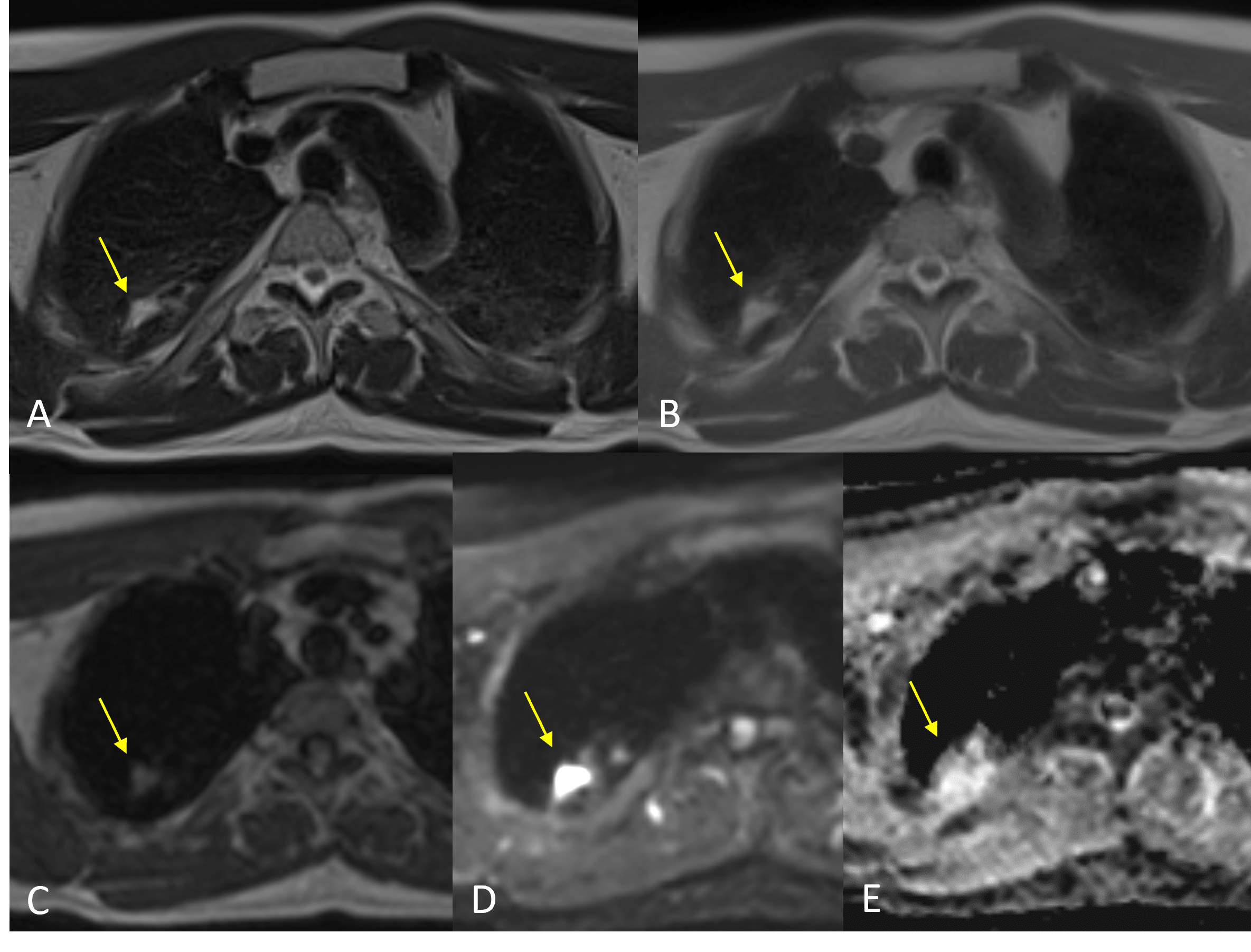
We obtained 10 scans without any complications. There were 2 incidentally revealed lung nodules, leading to further evaluation with chest CT in accordance with current guidelines. The total scan time was around 25 minutes as detailed in Figure 1. Image quality scores averaged 4.2±0.4 for T2 BLADE, 3.5±0.4 for T1RESS, 3.4±0.2 for FDMRI, 3.7±0.4 for Cardiac Cine imaging, 2.9±0.4 and 3.1±0.4 for Cardiac T1 and T2 mapping.T2 mapping value of the lung parenchyma averaged at 81.6 ± 3.5 ms. Ventilation defect percent and perfusion defect percent were 2.0±1.0% and 3.4±1.0%, aligning with data for 1.5 and 3T scanners6. Respiratory motion of the bilateral diaphragms was grossly normal in all scans.
The native T1 and T2 mapping of the myocardium averaged 652.9±54.9ms and 62.5±6.9ms. The cardiac chambers were normal in morphology and function in all scans with the left ventricular ejection fraction of 63.6±3.4%.
Discussion
T2 BLADE received the highest grade among the lung sequences, consistent with our experience. We found that the FDMRI ventilation and perfusion results aligned with the data from 1.5T and 3T scans, and they were also useful for assessing respiratory diaphragmatic motion. Cardiac cine imaging quality was sufficient in extracting ejection fraction and assessing chamber size and morphology. Mapping data from the lung and heart will be further assessed and collected, as no reliable reference values are currently reported.Conclusion
The initial observations of screening lung 0.55T MRI indicate a potential for broader utility in specific medical conditions, within 25 minutes. While its resolution may not equal that of CT scans, the absence of radiation exposure supports its use in screening and for conditions requiring frequent follow-up. Additionally, the included cardiac information could be invaluable in conditions where the lung and heart interact or coexist. This research also suggests future opportunities for selecting and developing lung sequences for specific purposes.Acknowledgements
This project was supported by the University of California San Francisco Department of Radiology and Biomedical Imaging Startup Grant.References
1.Adrienne E. Campbell-Washburn, Anthony F. Suffredini, and Marcus Y. Chen. High-Performance 0.55-T Lung MRI in Patient with COVID-19 Infection. Radiology 2021 299:2, E246-E247.
2.Azour L, Condos R, Keerthivasan MB, Bruno M, Pandit Sood T, Landini N, Silverglate Q, Babb J, Chandarana H, Moore WH. Low-field 0.55 T MRI for assessment of pulmonary groundglass and fibrosis-like opacities: Inter-reader and inter-modality concordance. Eur J Radiol. 2022 Sep 8;156:110515.
3. Usuda, K.; Ishikawa, M.; Iwai, S.; Yamagata, A.; Iijima, Y.; Motono, N.; Matoba, M.; Doai, M.; Hirata, K.; Uramoto, H. Pulmonary Nodule and Mass: Superiority of MRI of Diffusion-Weighted Imaging and T2-Weighted Imaging to FDG-PET/CT. Cancers 2021, 13, 5166.
4. Bandettini WP, Shanbhag SM, Mancini C, McGuirt DR, Kellman P, Xue H et al (2020) A comparison of cine CMR imaging at 0.55 T and 1.5 T. J Cardiovasc Magn Reson 22(1):37.
5. Edelman R, Leloudas N, Pang J, Bailes J, Merrell R, Koktzoglou I. Twofold improved tumor-to-brain contrast using a novel T1 relaxation-enhanced steady-state (T1RESS) MRI technique. Sci Adv. 2020 Oct 28;6(44):eabd1635.
6. Glandorf J, Klimes F, Voskrebenzev A, Gutberlet M, Behrendt L, Crisosto C, et al. (2020) Comparison of phase-resolved functional lung (PREFUL) MRI derived perfusion and ventilation parameters at 1.5T and 3T in healthy volunteers. PLoS ONE 15(12): e0244638.
7. Li, B, Lee, NG, Cui, SX, Nayak, KS. Lung parenchyma transverse relaxation rates at 0.55 T. Magn Reson Med. 2023; 89: 1522-1530.
Figures