2904
Predictors of 0.55T Respiratory Navigated Lung MRI Degradation1College of Medicine, University of South Alabama, Mobile, AL, United States, 2School of Medicine, University of California San Francisco, San Francisco, CA, United States, 3Siemens Medical Solutions USA, Inc., Malvern, PA, United States, 4Department of Radiology & Biomedical Imaging, University of California San Francisco, San Francisco, CA, United States
Synopsis
Keywords: Lung, Low-Field MRI
Motivation: The image quality generated using respiratory triggered sequences on low-field scanners is sometimes degraded, and it is currently not well known what causes this. This degradation can lead to image misinterpretation.
Goal(s): Our goal was to determine possible predictors of image quality degradation in low-field lung MRI.
Approach: Six radiologists graded anatomic 0.55T MRI images, and then analysis of patient clinical history, demographics, and respiratory navigation was conducted to determine any patterns.
Results: We found that clinical conditions including fibrotic interstitial lung disease and pulmonary artery pathologies, as well as descriptors such as increased body mass index can predict image quality degradation.
Impact: Our observation of degradative predictors serves as the foundation for research into altering of 0.55T MRI parameters to limit the degree of degradation, so that at-risk patients can still be scanned on these low-field machines with optimal image quality.
Introduction
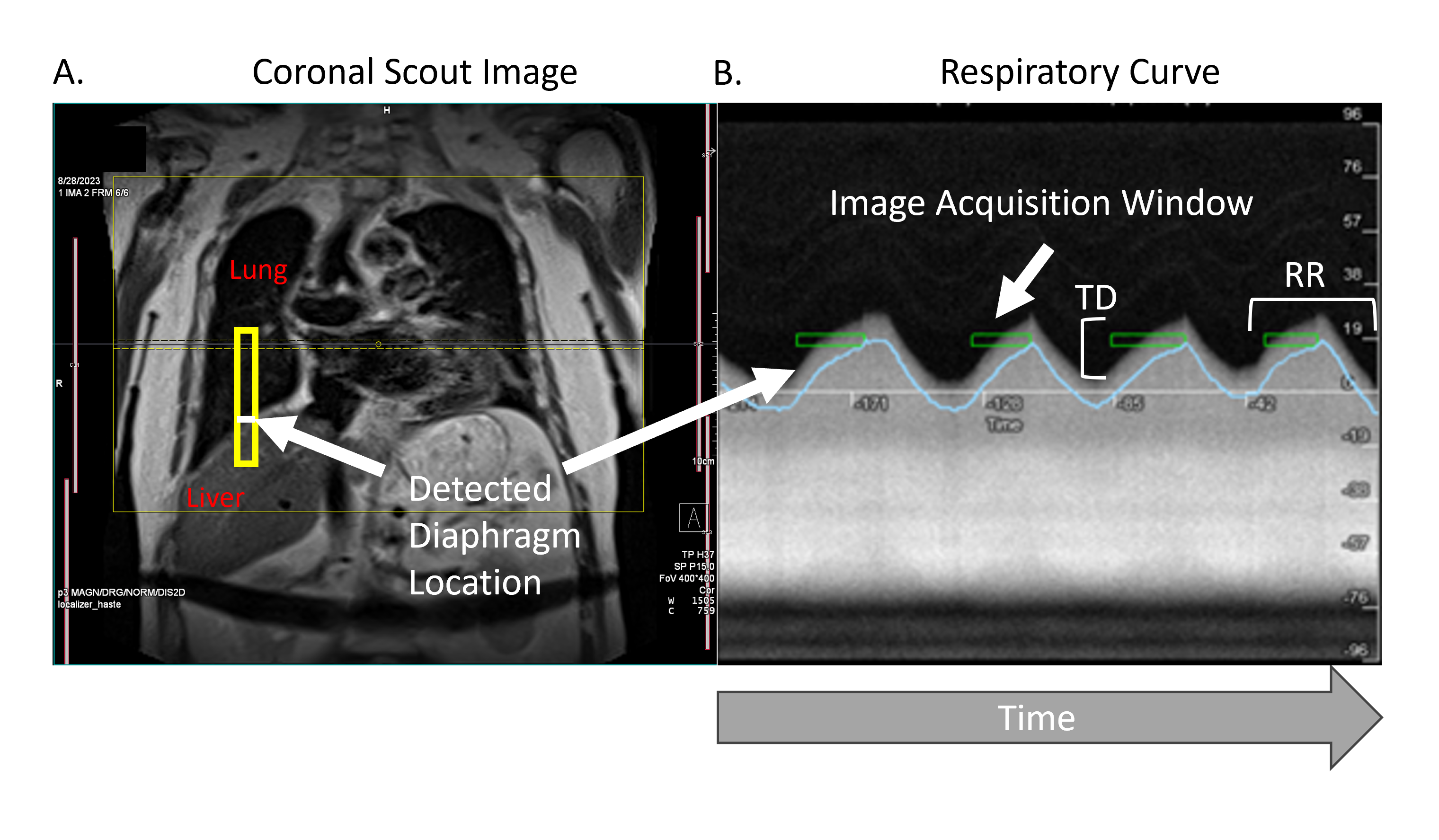
Image quality of lung MRI can be variable and depend on several factors including motion and respiratory navigation1. Recent developments in MRI technology regarding respiratory navigated sequences have allowed for the mitigation of certain degraders. However, in certain patient populations, even with this technology, the quality of imaging is still being degraded. There has been a paucity of studies trying to identify predictors of anatomic image degradation when using respiratory navigated sequences on a low-field scanner.Methods
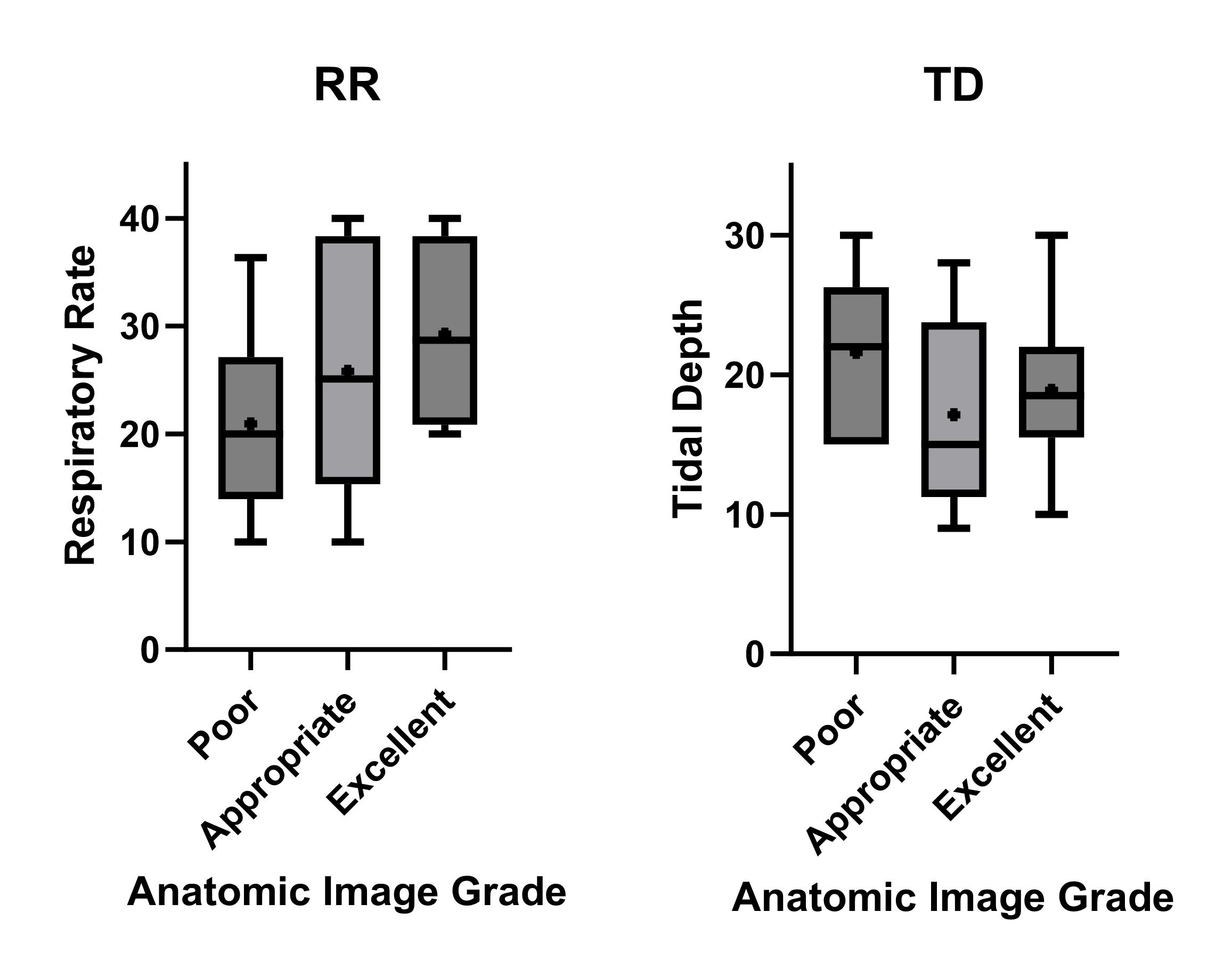
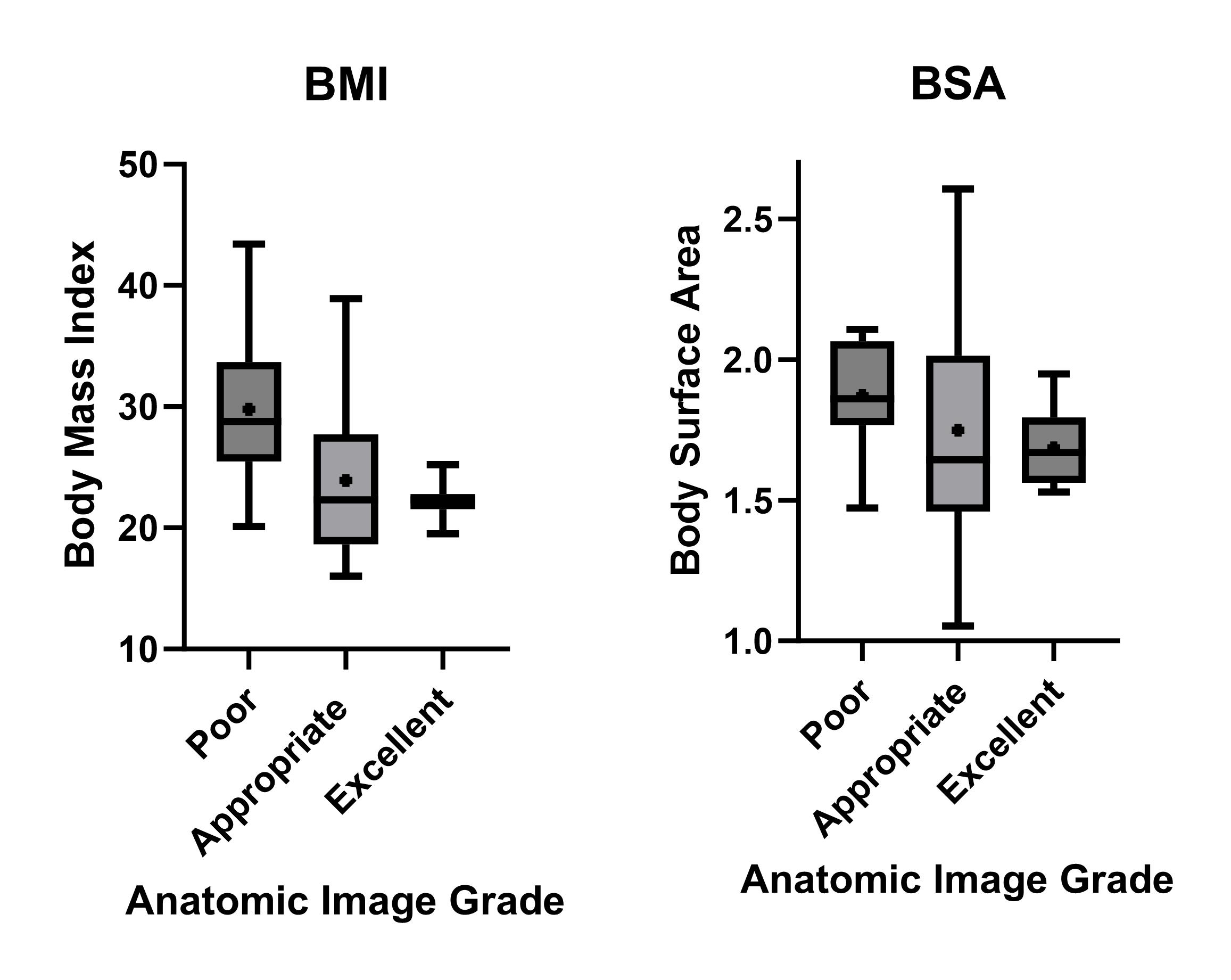
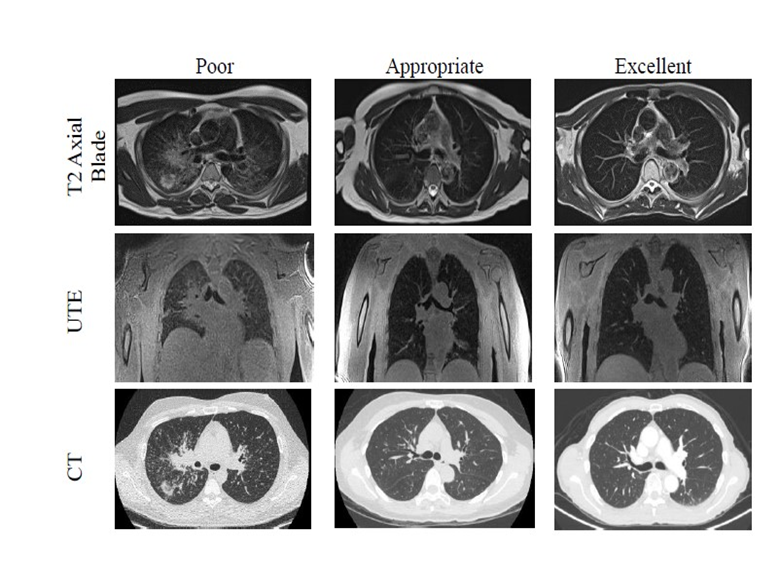
This prospective study scanned patients from January of 2023 to August of 2023 that had significant pulmonary pathologies such as lung nodules, fibrotic interstitial lung disease, and adenocarcinoma. Once T2 axial blade and ultrashort echo time sequences were acquired on the 0.55T scanner, grades were assigned based on image quality by six radiologists. Analysis of clinical correlates in and between grade tertiles was performed. Body surface area and BMI were also calculated to determine if patient height and weight had any impact on image quality. A one-way ANOVA was performed to compare the effect of respiratory rate, tidal volume, BMI, and body surface area on image quality.Results
28 patients (mean age, 59 years +/- 19; 17 women) were evaluated. Among the anatomic images that received poor grades, pulmonary artery pathology and fibrotic interstitial lung disease were the most common clinical correlates that appeared to degrade image quality. Increased body mass index (p<.05) was found to contribute to image degradation (Figure 3). Tidal volume, respiratory rate, and body surface area did not have a statistically significant effect on image quality.Discussion
Fibrotic interstitial lung disease was found to be one of the most common clinical correlates in images that received poor grades. The fibrotic nature of the condition, with a corresponding decrease in compliance, may have led to difficulty in distension during respiration. This could raise the amount of work necessary to breathe regularly. Additionally, it is possible that gas exchange is impaired in these patients due to interstitial scarring. These reductions in pulmonary function can result in an irregular respiratory rate to maintain adequate oxygenation. The triggered sequences are gated to end-expiration, therefore an increased respiratory rate would decrease the amount of time in end-expiration, which could increase the sequence time and allow for susceptibility to factors such as motion artifacts.Another predictor of image quality degradation was found to be body mass index. The effects of this covariate may have derived from both technical and physiological causes. Technologically, it is often necessary to increase the field of view in patients with a larger body habitus. This change in parameters allows for an increased viewing area, but does so at the expense of a lower resulting image resolution due to the voxels becoming larger. If the voxel size is held the same, using a larger field of view also requires longer image acquisition time. This increases the risk of motion artifacts and the potential for the patient’s respiratory rate to become irregular over that extended time period, even further exacerbating image degradation. Anatomically, larger body habitus in the form of accumulation of fat in the mediastinum or abdominal cavities of patients can have restrictive effects on lung physiology in a similar manner as fibrotic interstitial lung disease.
Conclusion
Factors including pulmonary artery pathology, fibrotic interstitial lung disease, and increased BMI can put patients at risk of MRI quality degradation on a 0.55T Siemens MAGNETOM Free.Max scanner. Being able to predict patient populations at risk of MRI degradation has a number of important clinical and research applications.From a clinical perspective, this information can be used to guide clinicians on the most appropriate use of the low-field scan in practice. Our findings suggest that the images of patients with fibrotic interstitial lung disease could be degraded. The inherent value added with this knowledge of degradative predictors lies in the potential ability to alter 0.55T MRI parameters before the start of scanning to try and limit the degree of degradation, so that at-risk patients could still be scanned on these machines with optimal image quality instead of having to opt to use another imaging modality such as CT.
It is our hope that these predictors can also be useful as a foundation for future research work to improve MRI of the lungs by generating hypotheses and discussion into why it is that the images of patients in these specific populations are being degraded. Additionally, this information could help in determining how best to improve the navigation technology to overcome the degradative impact of these predictors in the future.
Acknowledgements
This project was supported by the University of California, San Francisco’s Research Initiative to Promote Diversity in Radiology, and the University of California, San Francisco Department of Radiology and Biomedical Imaging Startup Grant. Special thanks to every member of the Sohn Laboratory, and the MRI technologists and imaging scientists at China Basin for their generous support. The preview figure was created with BioRender.com.References
- Campbell-Washburn AE, Malayeri AA, Jones EC, et al. T2-weighted Lung Imaging Using a 0.55-T MRI System. Radiology: Cardiothoracic Imaging. 2021;3:e200611 doi: 10.1148/ryct.2021200611.
Figures