2901
Clinical feasibility of mpMRI in determining bladder-sparing strategy after initial systemic therapy for muscle-invasive bladder cancer1West China Hospital, Sichuan University, Chengdu, China, ChengDu, China, 2Department of Clinical, Philips Healthcare, China, Chengdu, China, 3West China Hospital, Sichuan University, Chengdu, China, Chengdu, China
Synopsis
Keywords: Pelvis, Bladder, cancer
Motivation: NacVI-RADS based on mpMRI, was exclusively constructed to evaluate the response to systemic therapy and provided a reference for further treatment for patients with muscle-invasive bladder cancer (MIBC).
Goal(s): To examine the feasibility of the nacVI-RADS criteria in driving the therapeutic decision.
Approach: Patients received bladder sparing treatment were retrospectively retrieved. Pre-treatment and follow-up MRI were independently reviewed by two readers using the nacVI-RADS. We observed the pathological results from salvage RC and oncological outcomes for patients continuing systemic treatment with different nacVI-RADS category.
Results: We confirmed the consistency between the nacVI-RADS score and outcomes to initial treatment both pathologically and oncologically.
Impact: We preliminarily verified the feasibility of mpMRI in determining continuing or quitting bladder-sparing strategy after initial systemic therapy for MIBC. Besides, we modified nacVI-RADS, which showed a significantly improved performance in predicting the oncological outcomes after undergoing bladder sparing strategy.
Introduction
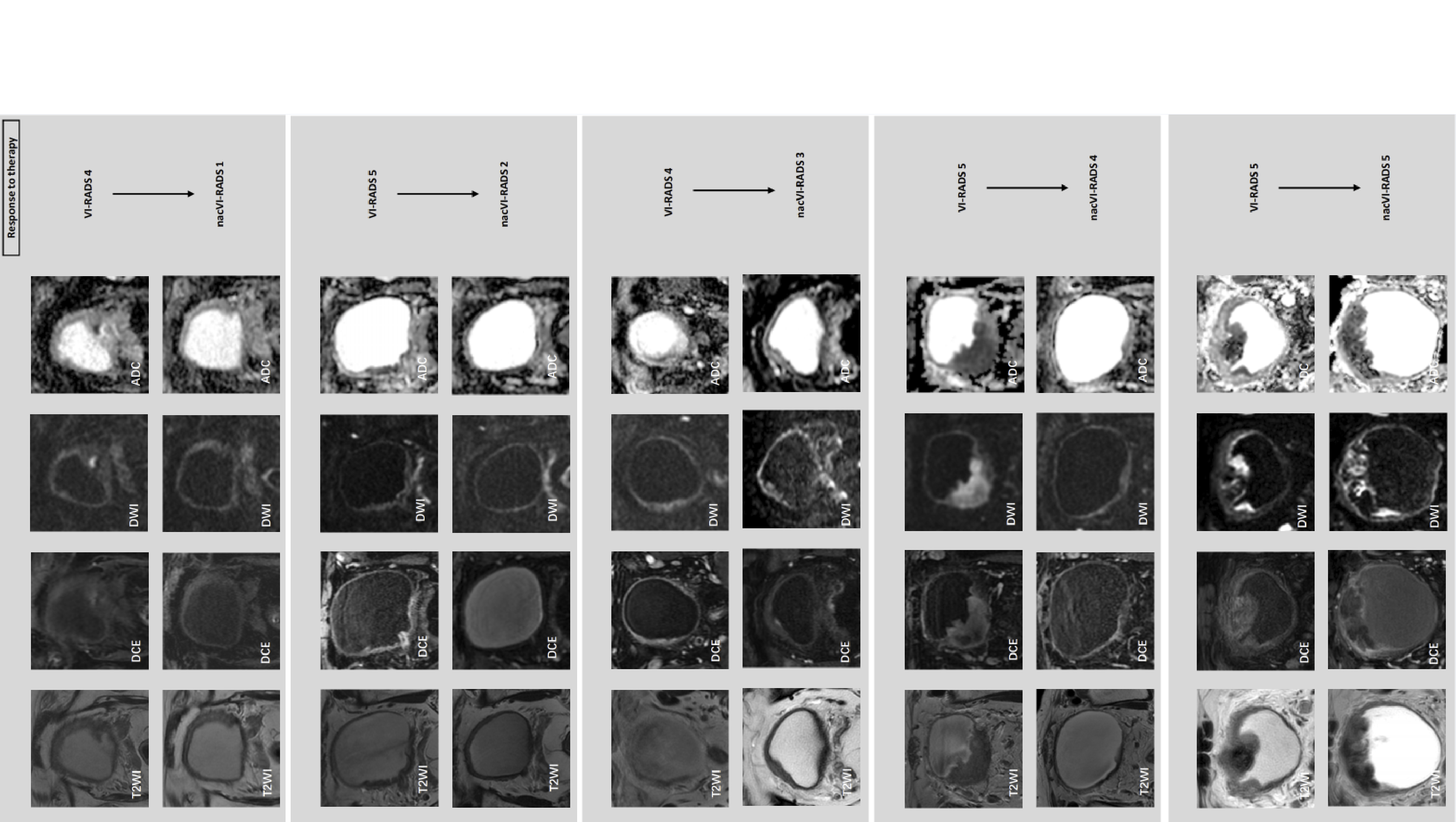
Muscle-invasive bladder cancer (MIBC) represents about 25% of all bladder cancer (BCa) cases and is defined as T2 or greater disease.[1] Although neoadjuvant chemotherapy before radical cystectomy (RC) has improved patient prognosis, most MIBC patients still suffer from a poor quality of life after RC.[1] Recently, tri-modal therapy (TMT) was proposed as a bladder-sparing approach comprising maximal transurethral resection of bladder tumor (TURBT), radiation, and chemotherapy. [2,3] However, about 20% of MIBC patients need a salvage cystectomy because TMT fails.[4,5] Because the salvage cystectomy should be performed as early as possible, it is essential to evaluate whether TMT should be continued during bladder-preserving therapy. Multiparametric magnetic resonance imaging (mpMRI) has played a significant role in pre-treatment staging and risk stratification for BCa.[6] Pecoraro et al. developed a novel algorithm based on pre-treatment and follow-up MRI after the last neoadjuvant cycle (Figure 1). This algorithm was exclusively constructed to evaluate the response to systemic therapy and provided a reference for further treatment, including active surveillance, a bladder sparing strategy, and standard RC defined as neoadjuvant chemotherapy VI-RADS (nacVI-RADS).[7] However, this preliminary study only included ten patients and failed to examine the feasibility of nacVI-RADS categories for guiding therapeutic decisions because all patients underwent RC after four RC cycles. Therefore, the primary aim of this retrospective study was to validate the accuracy of the nacVI-RADS criteria for the pathological response to therapy assessment. The second objective of this study was to examine the feasibility of the nacVI-RADS criteria in driving the therapeutic decision.Methods
This retrospective, observational study was approved by the Institutional Review Board and Ethical Committee of our hospital, and patient informed consent was waived. Patients diagnosed with local advanced MIBC from June 2019 to May 2021 who underwent systemic treatment were retrospectively collected. Two sets of MR images (pre-and post-treatment) were obtained before staging TURBT and after induction treatment. Both sets of MR scanning were compliant with the VI-RADS and performed on a 3T MR scanner (Elition, Philips), including T2-weighted imaging (T2WI), diffusion-weighted imaging (DWI), and dynamic contrast enhanced (DCE) sequences. [6]These two sets of images were evaluated independently by two experienced radiologists with 5 and 8 years assessing bladder tumors, respectively, who were blinded to the pathological results and follow-up outcomes. We observed the pathological results from salvage RC and oncological outcomes for patients continuing systemic treatment with different nacVI-RADS category. Receiver operating characteristic curve (ROC) analysis was used for assessing predictive performance to predict good response.Results
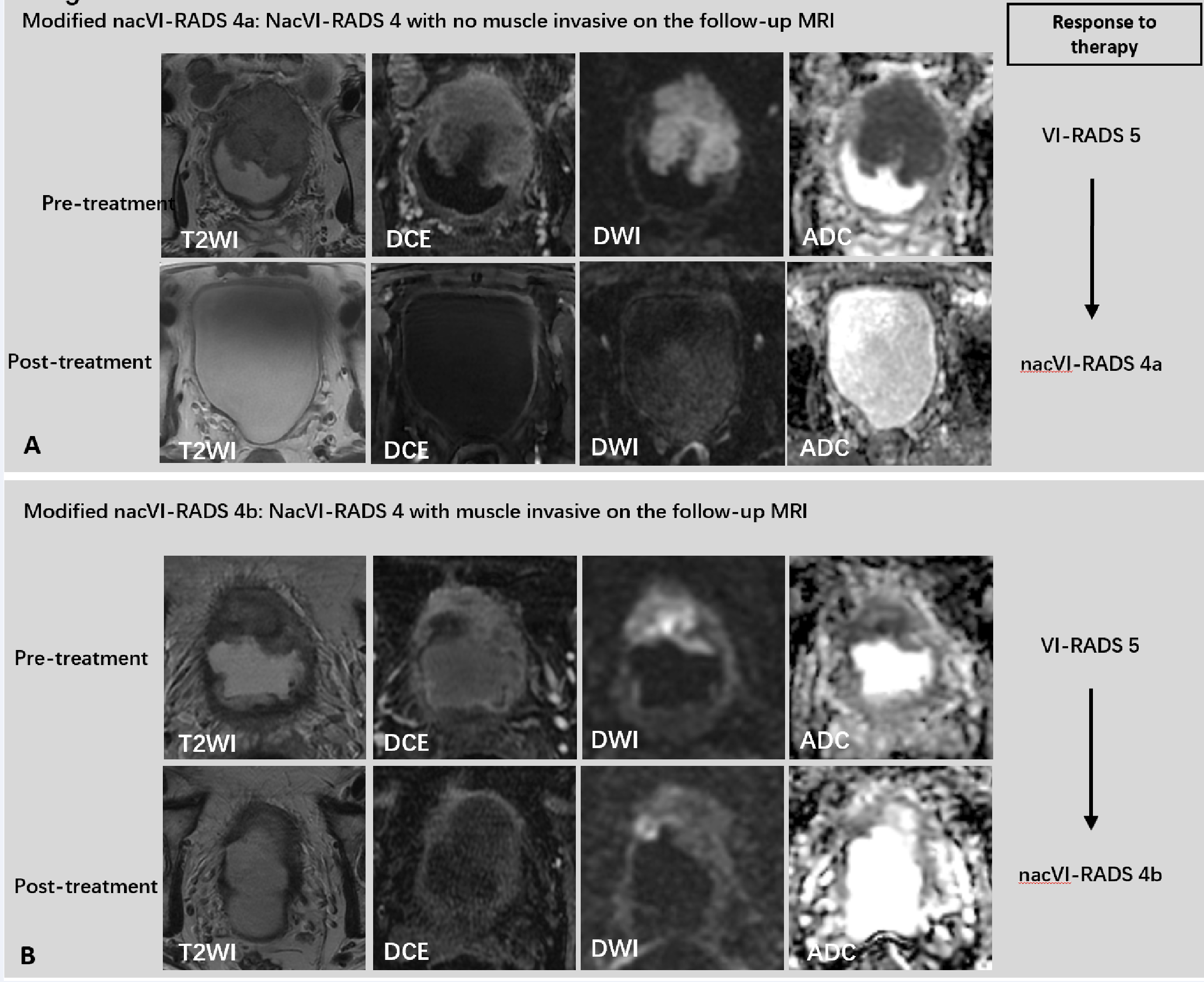
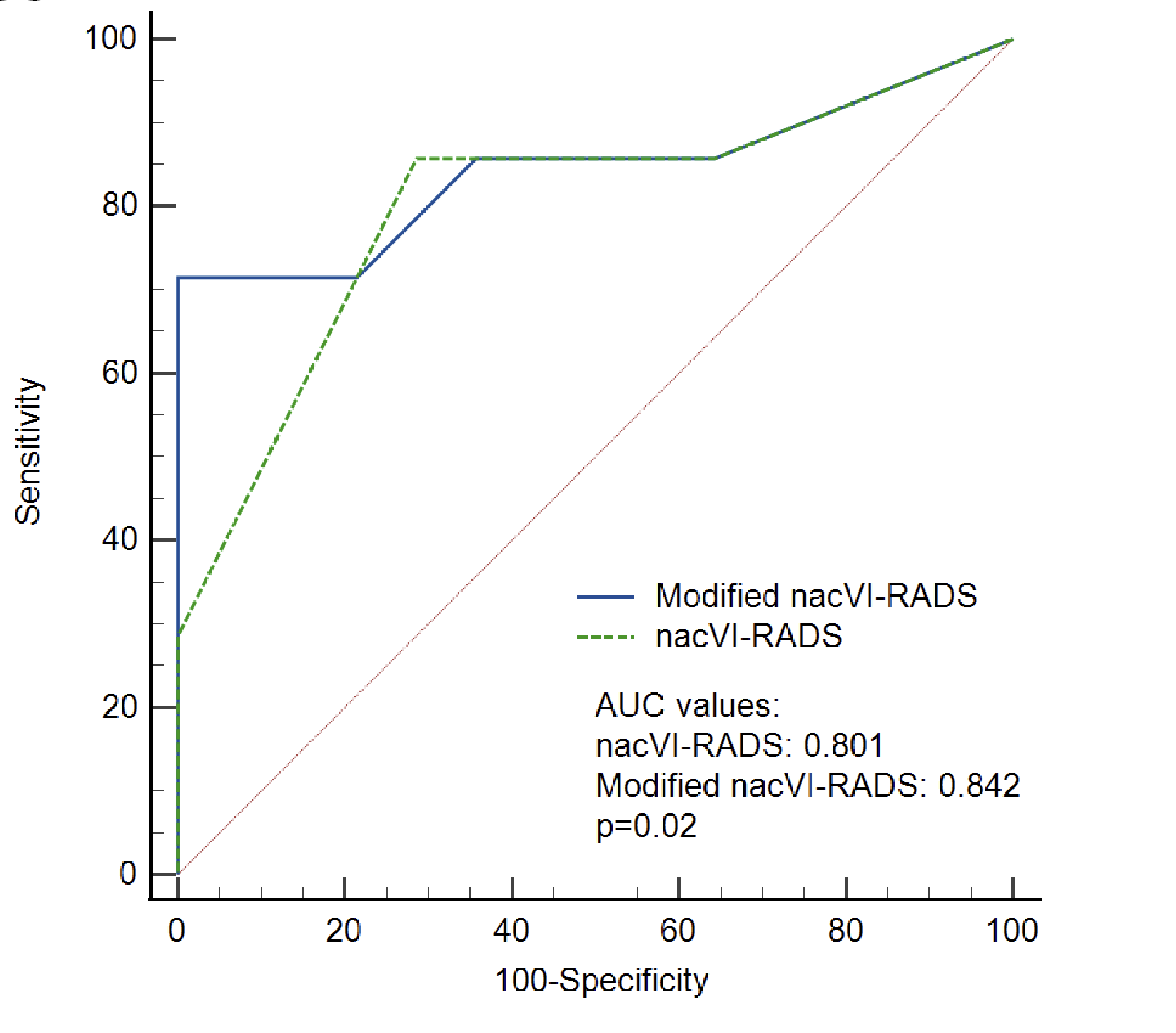
Among the 33 patients, 12 underwent RC, and 21 received sequential systemic treatment. The nacVI-RADS matched the final pathological results from RC. For patients receiving sequential systemic therapy, ROC analysis showed that the optimal criterion was nacVI-RADS ≥ 3 with area under the curve (AUC) value of 0.801, while patients with nacVI-RADS 4 had indeterminate responses to the bladder sparing treatment. Therefore, we proposed modified nacVI-RADS by further subdividing nacVI-RADS 4 into nacVI-RADS 4a and 4b (Figure 2), according to the status of muscle-invasiveness in follow-up MRI. The AUC value of the modified nacVI-RADS was 0.842, significantly higher than that of nacVI-RADS (Figure 3, p=0.02).Discussion
This study was the first to evaluate the association between mpMRI changes before and after systemic treatment and treatment outcomes among patients undergoing bladder-preserving strategy. Among patients who chose the bladder preservation strategy, we found that patients with nacVI-RADS scores of 3 or less had a significant likelihood of complete or partial response during follow-up, patients with score of 5 had SD and might benefit from salvage RC, whereas patients with scores of 4 had indeterminate responses to the bladder sparing treatment. Thus, we proposed to modify nacVI-RADS by subdividing patients with nacVI-RADS score of 4, according to the status of muscle-invasiveness assessed by follow-up MRI. For patients with nacVI-RADS 4a, whom have no involvement of the muscularis propria in the follow-up MRI, might have better response for continuing the bladder-sparing strategy, than those nacVI-RADS 4b remaining muscle-invasive diseases. Our results differed from the preliminary study of nacVI-RADS, which showed that patients with scores of 4 were less likely to be partial responders.[7] Therefore, our results provided complementary assessment to nacVI-RADS, and might positively influence the applicability of nacVI-RADS among patients planning bladder preservation.Conclusions
This small-size study confirmed the consistency between the nacVI-RADS score and pathological response to initial treatment, and indicated that early assessment using modified nacVI-RADS might be a predictive factor for the prognostic outcome after continuing systemic outcome.Acknowledgements
NoneReferences
1. Flaig, T.W.; Spiess, P.E.; Agarwal, N.; Bangs, R.; Boorjian, S.A.; Buyyounouski, M.K.; Chang, S.; Downs, T.M.; Efstathiou, J.A.; Friedlander, T.; et al. Bladder Cancer, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 2020, 18, 329–354, doi:10.6004/jnccn.2020.0011.
2. Chang, S.S.; Bochner, B.H.; Chou, R.; Dreicer, R.; Kamat, A.M.; Lerner, S.P.; Lotan, Y.; Meeks, J.J.; Michalski, J.M.; Morgan, T.M.; et al. Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline. J Urol 2017, 198, 552–559, doi:10.1016/j.juro.2017.04.086.
3. Büchser, D.; Zapatero, A.; Rogado, J.; Talaya, M.; Martín de Vidales, C.; Arellano, R.; Bocardo, G.; Cruz Conde, A.; Pérez, L.; Murillo, M.T. Long-Term Outcomes and Patterns of Failure Following Trimodality Treatment With Bladder Preservation for Invasive Bladder Cancer. Urology 2019, 124, 183–190, doi:10.1016/j.urology.2018.07.058.
4. Efstathiou, J.A.; Spiegel, D.Y.; Shipley, W.U.; Heney, N.M.; Kaufman, D.S.; Niemierko, A.; Coen, J.J.; Skowronski, R.Y.; Paly, J.J.; McGovern, F.J.; et al. Long-Term Outcomes of Selective Bladder Preservation by Combined-Modality Therapy for Invasive Bladder Cancer: The MGH Experience. Eur Urol 2012, 61, 705–711, doi:10.1016/j.eururo.2011.11.010.
5. Giacalone, N.J.; Shipley, W.U.; Clayman, R.H.; Niemierko, A.; Drumm, M.; Heney, N.M.; Michaelson, M.D.; Lee, R.J.; Saylor, P.J.; Wszolek, M.F.; et al. Long-Term Outcomes After Bladder-Preserving Tri-Modality Therapy for Patients with Muscle-Invasive Bladder Cancer: An Updated Analysis of the Massachusetts General Hospital Experience. Eur Urol 2017, 71, 952–960, doi:10.1016/j.eururo.2016.12.020.
6. Panebianco, V.; Narumi, Y.; Altun, E.; Bochner, B.H.; Efstathiou, J.A.; Hafeez, S.; Huddart, R.; Kennish, S.; Lerner, S.; Montironi, R.; et al. Multiparametric Magnetic Resonance Imaging for Bladder Cancer: Development of VI-RADS (Vesical Imaging-Reporting And Data System). Eur Urol 2018, 74, 294–306, doi:10.1016/j.eururo.2018.04.029.
7. Pecoraro, M.; Del Giudice, F.; Magliocca, F.; Simone, G.; Flammia, S.; Leonardo, C.; Messina, E.; De Berardinis, E.; Cortesi, E.; Panebianco, V. Vesical Imaging-Reporting and Data System (VI-RADS) for Assessment of Response to Systemic Therapy for Bladder Cancer: Preliminary Report. Abdom Radiol (NY) 2021, doi:10.1007/s00261-021-03365-5.
Figures