2899
Clinical PC VIPR Implementation for Abdominal Hemodynamics Assessment in Patients with Renal Cell Carcinoma Tumor Thrombus1Radiology, University of Wisconsin, Madison, WI, United States, 2Mechanical Engineering, University of Wisconsin, Madison, WI, United States, 3Medical Physics, University of Wisconsin, Madison, WI, United States, 4Urology, University of Wisconsin, Madison, WI, United States
Synopsis
Keywords: Kidney, Kidney
Motivation: 4D flow MRI provides volumetric time-resolved blood flow measurements in short scan times. Nevertheless, 4D Flow MRI techniques have not been clinically applied to abdominal neoplasms invading into the vasculature, altering blood flow and posing unique surgical problems.
Goal(s): Describe the clinical implementation of 4D Flow MRI for treatment planning of RCC patients with venous tumor thrombus undergoing nephrectomy and thrombectomy.
Approach: Our institution has established a 4D flow MRI workflow for blood flow assessment based on multidisciplinary collaboration and several other factors.
Results: Clinical 4D flow for treatment planning of RCC patients has been successfully implemented at our institution.
Impact: 4D flow MRI allows for comprehensive non-invasive assessment of the abdominal circulation in the clinical setting. The methodology presented here has provided unvaluable input to the care team of patients with complicated cases of advanced RCC during treatment planning.
Introduction
4D flow MRI provides volumetric time-resolved blood flow measurements in short scan times. Most applications of 4D flow imaging to date are cardiovascular. However, recent efforts have also demonstrated utility in abdominal blood flow1,2. Hoffman et al.3 measured renal artery blood flow in kidney cancer patients, finding flow asymmetry. Motoyama et al.4 measured blood velocity in transplant recipient renal arteries and compared results with Doppler ultrasound flow. Several studies have verified 4D flow measurement validity5 by comparing to 2D flow and analyzing internal consistency6. Nevertheless, 4D flow techniques have not been clinically applied to abdominal neoplasms invading into the vasculature, altering blood flow and posing unique surgical problems.Advanced renal cell carcinoma (RCC) may invade into the renal vein and inferior vena cava (IVC), resulting in tumor thrombus. Occlusive thrombus changes local hemodynamics, including flow reversal. Moreover, chronic occlusion leads to venous collateralization, which is vital to recognize pre-operatively given increased surgical complexity, patient morbidity and mortality from bleeding risk. Detailed 4D flow MRI blood flow assessment of the renal veins, IVC, and venous collaterals, aids in surgical decision making. Therefore, it has been incorporated into routine imaging protocols at our institution for treatment of patients with advanced RCC with tumor thrombus. The purpose of this abstract is to describe the clinical implementation of 4D Flow MRI for treatment planning of RCC patients with venous tumor thrombus undergoing nephrectomy and thrombectomy.
Methods
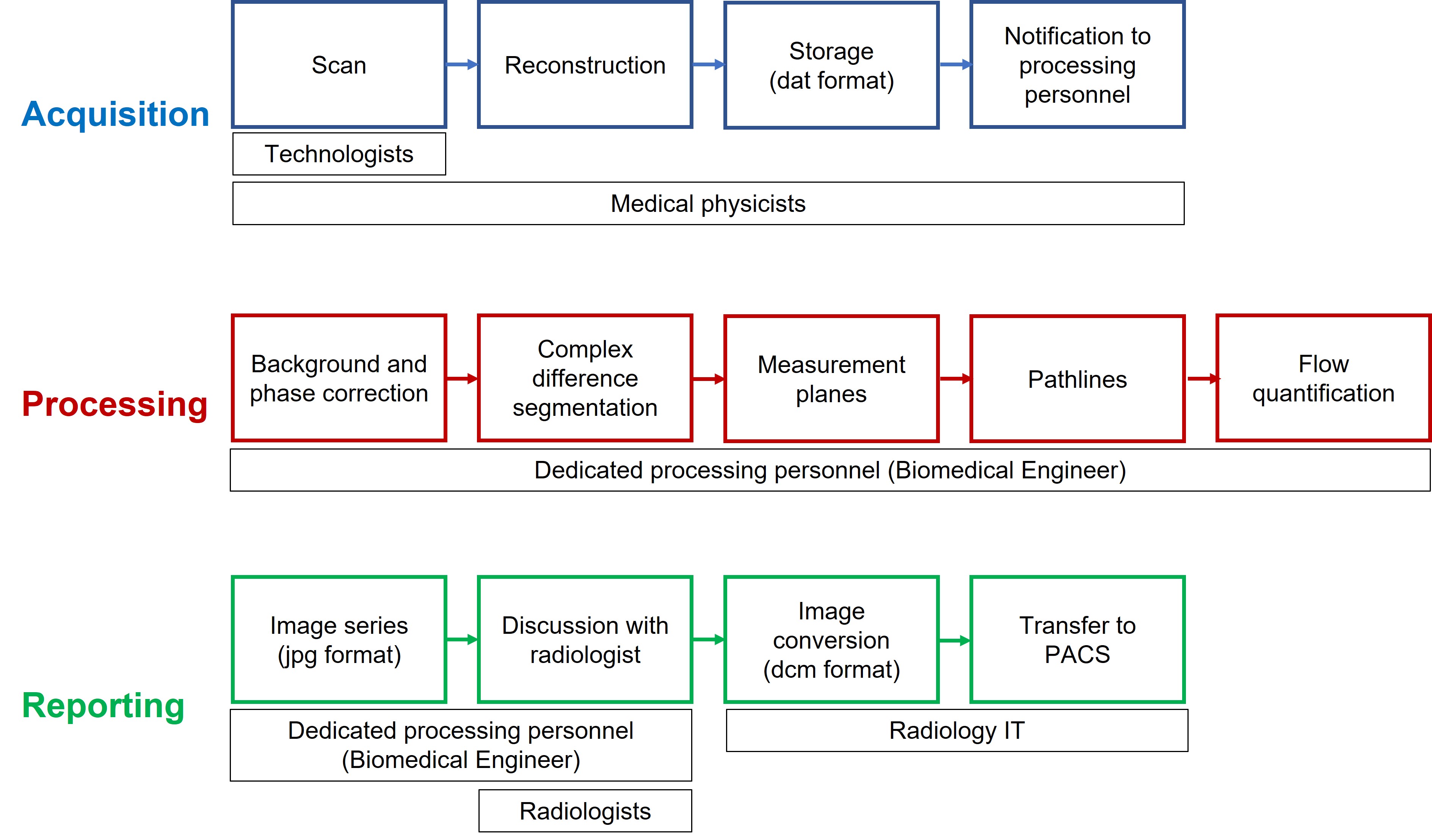
4D Flow MRI blood flow assessment is performed by an imaging analysis research support laboratory. Diagnostic assessment with 4D flow MRI has been recently added to clinical imaging protocols involving RCC cases (Figure 1).The PC-VIPR 4D flow sequence has been optimized for abdominal cases with parameters: venc = 60 cm/s, isotropic resolution 1.25 mm, and flip angle 12° or 8° for contrast-enhanced scans and non contrast-enhanced scans, respectively. Scan data reconstruction (20 frames/ cardiac cycle) is performed automatically and stored in a dedicated network folder while notifications are sent to processing personnel.
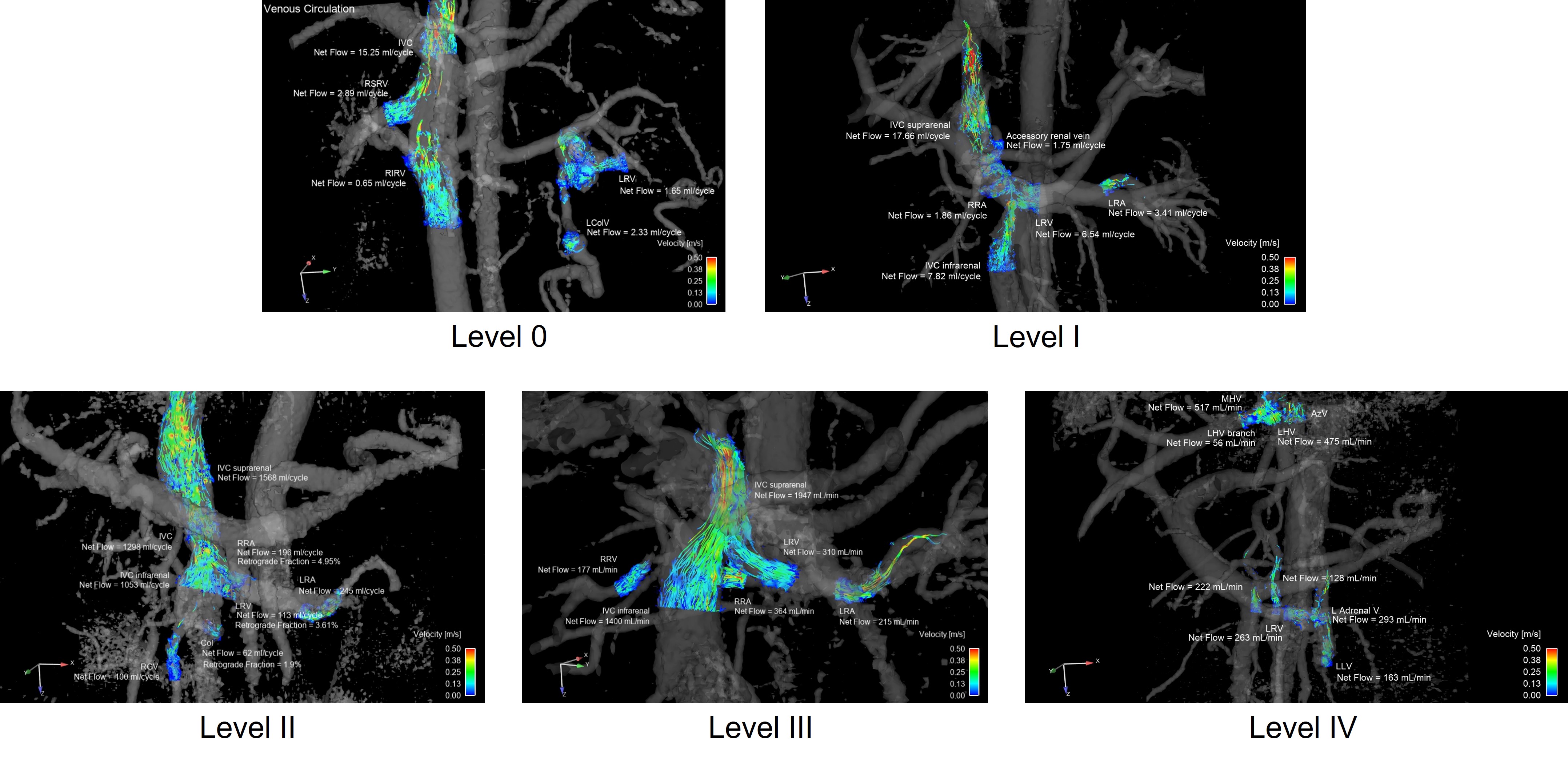
Custom-developed tools are used for background and phase correction, as well as macros for subsequent processing (EnSight). Anatomical segmentation is performed based on complex difference (phase contrast angiogram) data, where a threshold allowing vessel visualization is defined. Planes are perpendicularly placed at various sites, including renal arteries, renal veins, IVC, and venous collaterals. Pathlines are generated with traces originating from each plane, where quantitative analysis is performed obtaining net flow and retrograde fraction. A video containing color-coded velocity pathlines and flow is created by generating an image (jpg) per time frame (Figure 2). Results are discussed with the reading radiologist, with possible iterations in the processing workflow until approval. Custom-developed algorithms convert the EnSight image series to dicom format with subsequent transfer to PACS. The turnaround time for processing one case is in average one day, but no more than one week depending on the clinical needs of the referring urologist.
Results
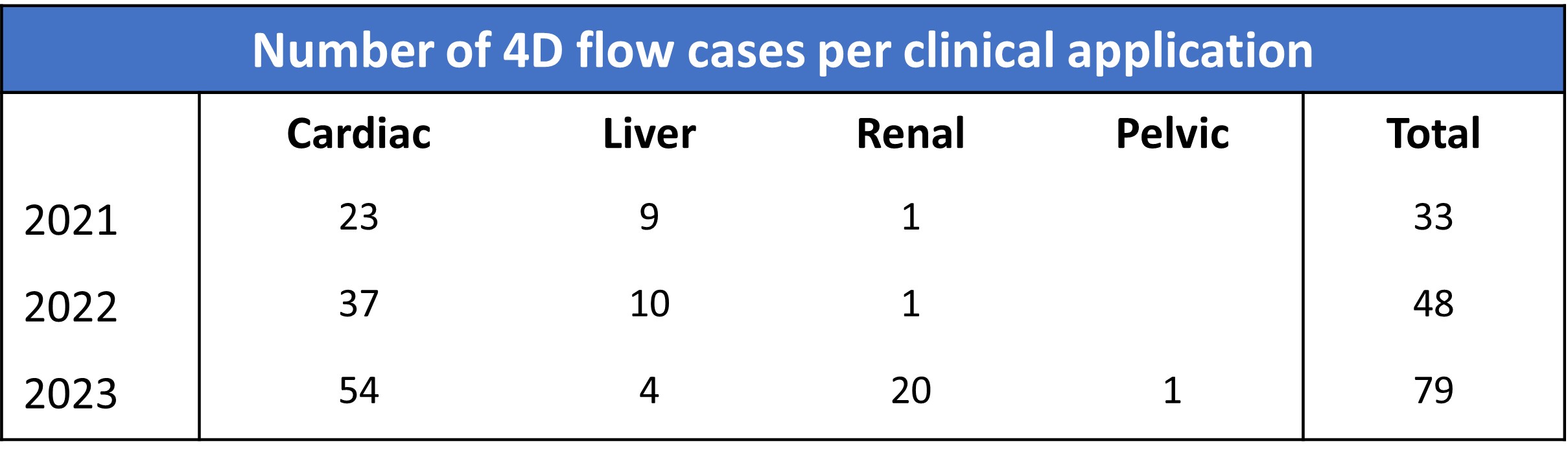
Clinical 4D flow processing has been successfully implemented at our institution. The total number of 4D flow cases, including cardiac, liver, pelvic and renal applications, has steadily grown (Figure 3). From 2021 to 2022, the total number of cases increased by 45%; from 2022 to 2023, totals increased by 65%. Renal cases represented 3% of the total 4D flow cases in 2021, 2% in 2022 and 25% in 2023, up to date.Blood flow assessment for RCC cases has spanned all thrombus levels as defined by standard classification (Figure 2, Video 1).
Discussion and Conclusion
Results from 4D flow MRI are helpful in identifying collateral circulation that may be sufficient for venous return, thus resecting the IVC without the need for replacement. In cases with partial IVC occlusion, blood flow information is helpful in surgical planning including creating appropriate multidisciplinary surgical teams (e.g. cardiothoracic surgeons, perfusionists, vascular surgeons) and determining the IVC reconstruction extent.Our institution has established a 4D flow MRI workflow for blood flow assessment. Multidisciplinary collaboration and several other factors have facilitated clinical implementation: 1) development of algorithms to automatically reconstruct scan data, store resulting files, and notify key personnel; 2) standard processing workflow with simple segmentation; 3) dedicated data processing personnel; 4) experienced team of reading radiologists, familiar with results interpretation; and 5) the capability of preparing and transferring data to PACS. Recognition of 4D flow MRI clinical value by our physicians has been key--growing its demand and motivating important support by our institution’s administration.
Future work is focused on increasing workflow efficiency and standard processing methods, disseminating its utility among radiologists and medical trainees, and implementing internal quality assurance protocols.
Acknowledgements
We are grateful to UW Departments of Radiology and Medical Physics, as well as to Daryn Belden for his IT support regarding PACS reporting. GE Healthcare provides research support to UW Madison.
References
1. Wieben O, Roberts G, Corrado P, et al. Four-dimensional flow MR imaging: technique and advances. Magn Reson Imaging Clin N Am. 2023;31:433-449.
2. Takayama T, Takehara Y, Sugiyama M, et al. use of three-dimensional time-resolved phase-contrast magnetic resonance imaging with vastly undersampled isotropic projection reconstruction to assess renal blood flow in a renal cell carcinoma patient treated with sunitinib: a case report. BMC Research Notes. 2014;7:527.
3. Hoffman C, García-Rodríguez S, Roldán-Alzate R, et al. 4D flow analysis of renal flow changes due to kidney cancer. SMRA Conference, Chicago, 2016.
4. Motoyama D, Ishii Y, Takehara Y, et al. Four-dimensional phase-contract vastly undersampled isotropic projection reconstruction (4D PC-VIPR) MR evaluation of the renal arteries in transplant recipients: preliminary results. J Magn Reso Imaging. 2017;46:595-603.
5. Rutkowski D, Medero R, Garcia F, et al. MRI-based modeling of spleno-mesenteric confluence flow. J Biomech. 2019;88:95-103.
6. Wentland A, Grist T, Wieben O. Repeatability and internal consistency of abdominal 2D and 4D phase contrast MR flow measurements. Acad Radiol 2013;20:699-704.
Figures