2896
Differential diagnosis of renal tumors using dual echo time diffusion weighted imaging (dual TE-DWI)1Radiology, Kawasaki Medical School, Kurashiki, Japan, 2Philips Japan, Tokio, Japan, 3Kawasaki Medical School, Kurashiki, Japan, 4Urology, Kawasaki Medical School, Kurashiki, Japan
Synopsis
Keywords: Urogenital, Kidney
Motivation: In renal tumors, it is often difficult to differentiate between benign and malignant tumors, which could reduce unnecessary biopsies and surgeries.
Goal(s): To differentiate between angiomyolipoma (AML) and renal cell carcinoma (RCC).
Approach: Imaging with two types of diffusion-weighted images (DWI) with different Echo times (TE) and comparing T2 signals in AML and RCC at DWI (b=0) and DWI (b=1200).
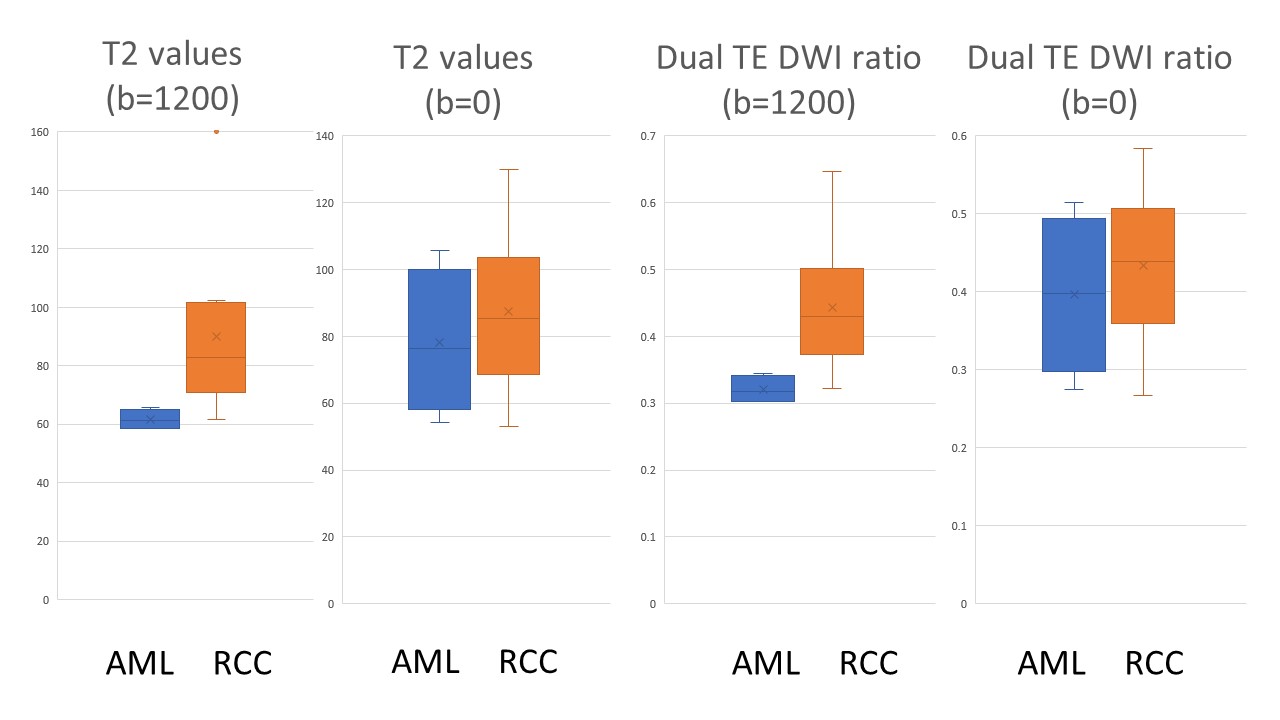
Results: T2 signals at high diffusion restriction DWI (b=1200) were significantly lower in AML compared to RCC.
Impact: There is potential to preoperatively differentiate AML non-invasively, which previously due to the difficulty in differentiation, led to invasive diagnostic methods such as biopsies and unnecessary surgeries.
Introduction
Differentiating between the common benign tumor angiomyolipoma (AML) and the malignant renal cell carcinoma (RCC) is often challenging in small renal tumors under 4 cm in diameter. Therefore, biopsies are sometimes performed, which are invasive and carry the risk of bleeding and infection. Unnecessary surgeries are also not uncommon when malignancy cannot be ruled out. The aim of this study was to distinguish angiomyolipoma from RCC of the kidney.Methods
This study included 14 patients with AML (n=4) and renal cell carcinoma (n=10) (8 clear cell RCC and 2 chromophobe RCC) diagnosed pathologically. Renal masses larger than 4 cm in diameter and cases that could be diagnosed on preoperative MRI as AML (massive fatty component) or RCC (high signal on T2WI) were excluded. All patients underwent MRI using a 3-Tesla MRI machine including dual TE-DWI. Dual TE-DWI (b values=0 and 1200 s/mm2) were acquired with combinations of TE=70 and 140 msec. Size (long diameter), T2 signal intensity ratio (SIR) (SI of tumor/SI of muscle), T2 values on DWI (b=0 and 1200) and SIR (SI of tumor/SI of muscle) on DWI (b=0 and 1200) for each TE (TE=70 and 140) and ADC values (b=1200) were measured in all tumors. These parameters were compared between AML and RCC.Results
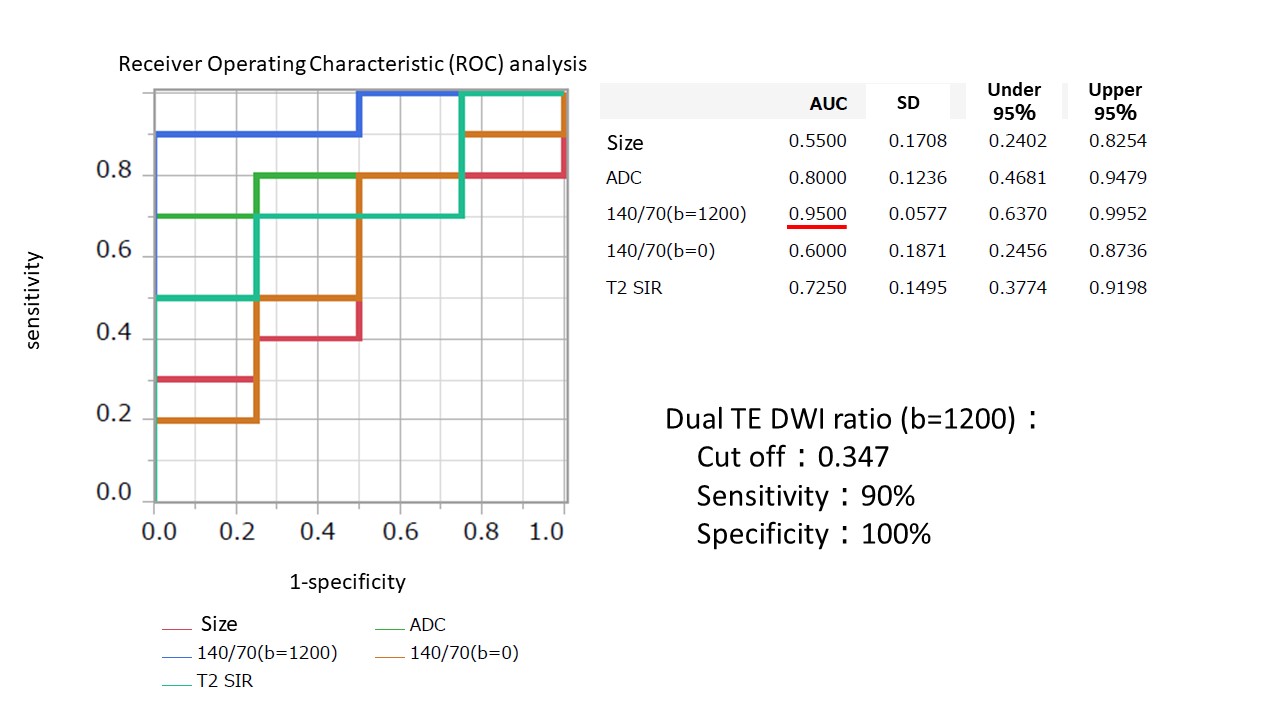
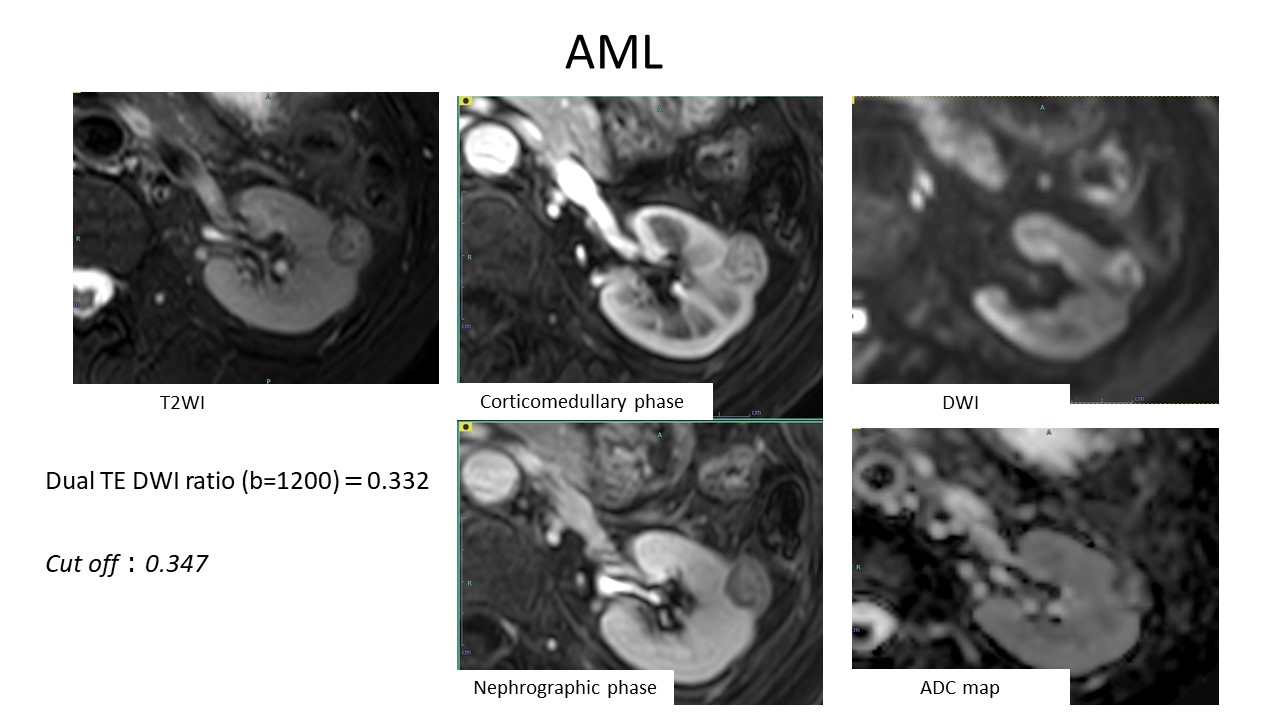
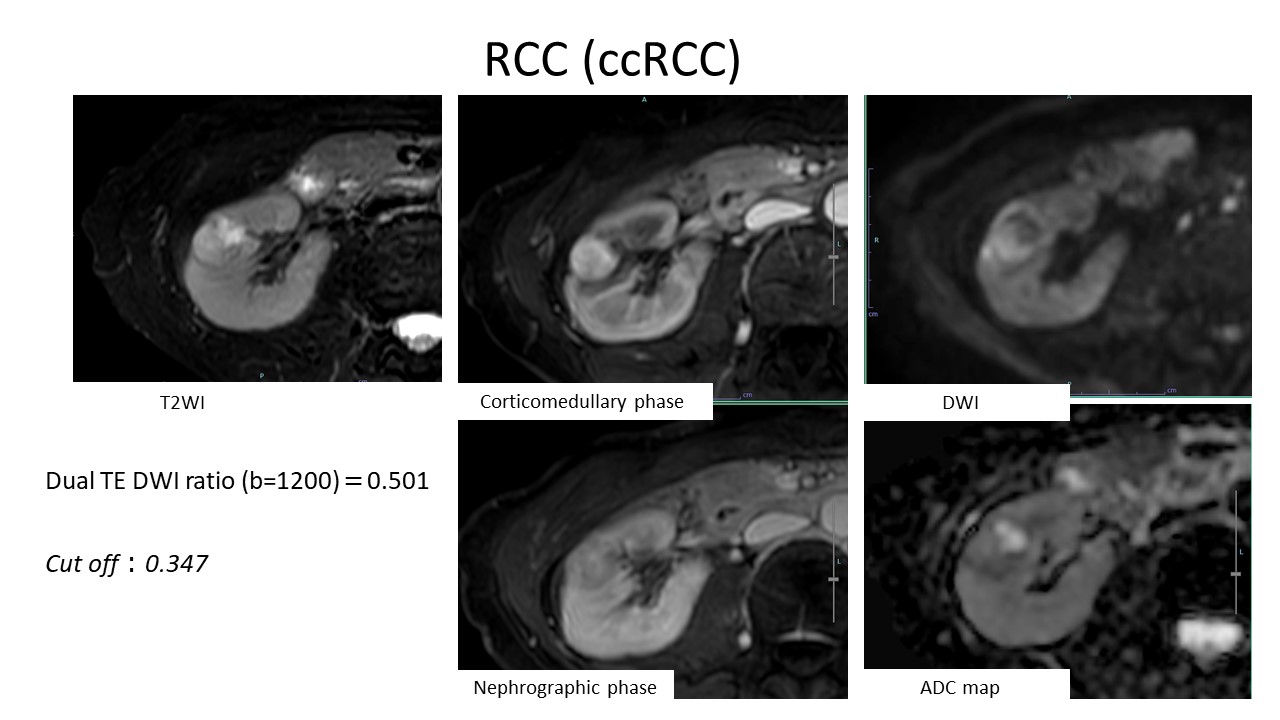
A significant difference was seen between AML and RCC in T2 values on DWI (b=1200) (mean ± SD: 78.12±21.75 vs 87.34±24.28msec; p=0.008) and SI ratio of dual TE-DWI (b=1200) (mean ± SD: 0.32±0.02 vs 0.44±0.10; p=0.008). No significant difference was seen in size, T2 SIR, T2 values on DWI (b=0), SI ratio of dual TE-DWI (b=0) and ADC values. ROC analysis showed that the area under the curve (AUC) for the SI ratio of dual TE-DWI (b=1200) was high at 0.9500, and with a cutoff of 0.347, the sensitivity was 90% and specificity was 100%.Discussion
The T2 values in DWI (b=1200) may reflect a focus on tumor cells by suppressing the signal of free water, such as in cystic degeneration or necrosis. Additionally, the SI ratio of dual TE-DWI (b=1200) could be focusing more on tumor cells by calculating the ratio of SIR at short TE (=70), which minimizes the effect of T2 relaxation, and at long TE (=140), which is strongly influenced by T2 relaxation. The results indicate that in small renal tumors with low T2WI signals, where it is difficult to differentiate AML from RCC, AML has lower T2 values in the tumor cells themselves compared to RCC.Conclusion
Dual TE-DWI might be useful to distinguish AML from RCC of the kidney. This technique may allow us to avoid invasive tests such as biopsies and unnecessary surgical resection of AML.Acknowledgements
No acknowledgment found.References
1.Tom DeRoche et al. Pathologic characteristics of solitary small renal masses: can they be predicted by preoperative clinical parameters?: Am J Clin Pathol. 2008 Oct;130(4):560-4
2. Thiravit S, et al. The different faces of renal angiomyolipomas on radiologic imaging: a pictorial review. Br J Radiol. 2018 Apr;91
3. Lopes Vendrami C, et al. Differentiation of Solid Renal Tumors with Multiparametric MR Imaging. Radiographics. 2017 Nov-Dec;37(7):2026-2042
Figures