2873
Prediction of Pathological Response to Neoadjuvant Chemotherapy in Breast Cancer Using Intravoxel Incoherent Motion Histogram Parameters1Tianjin Medical University Cancer Institute and Hospital, Tianjin, China, 2Tianjin Medical University General Hospital, Tianjin, China, 3GE Healthcare, Beijing, China, Beijing, China
Synopsis
Keywords: IVIM, Breast
Motivation: The motivation behind this study lies in the need for accurate prediction of pathological response to neoadjuvant chemotherapy (NAC) in breast cancer.
Goal(s): Our goal was to assess the potential of IVIM-derived histogram parameters as predictive markers before NAC in breast cancer patients.
Approach: We conducted a comprehensive analysis of 287 breast cancer cases, utilizing IVIM model-based parameters and multivariate logistic regression. The study included voxel-wise analysis.
Results: The prediction model, combining the selected IVIM parameters and PR status, exhibited strong discriminative power. Additionally, we identified the minimum of D, Skewness of D* and D as significant volumetric predictors associated with pCR.
Impact: The impact of this study is significant, as it enhances breast cancer treatment by providing a reliable predictive model for neoadjuvant chemotherapy response, potentially improving patient outcomes and treatment strategies.
Introduction
Neoadjuvant chemotherapy (NAC) has emerged as the preferred treatment strategy for locally advanced breast cancer, offering the potential to reduce tumor burden and facilitate breast-conserving surgery while avoiding axillary lymph node dissection. However, the response to NAC varies widely due to inherent heterogeneity among breast cancer subtypes. Pathological complete response (pCR) rates range from 5% to 60%, with approximately one-third of patients experiencing progression or relapse1,2. Accurate prediction of treatment response is crucial for selecting the most effective therapy. Magnetic resonance imaging (MRI) is a valuable tool for evaluating NAC response in breast cancer. Traditionally, tumor size measured by dynamic contrast-enhanced MRI (DCE-MRI) has been used to predict and monitor response using the Response Evaluation Criteria in Solid Tumors (RECIST 1.1) criteria. However, it is increasingly recognized that changes in intratumoral microstructure precede alterations in morphology. The apparent diffusion coefficient (ADC) obtained from diffusion-weighted imaging (DWI) is a potential biomarker for monitoring response, reflecting changes in tumor cellular density during NAC. Nevertheless, ADC values derived from the monoexponential model may be influenced by capillary perfusion. The intravoxel incoherent motion (IVIM) model, by employing multiple b values, can separate the perfusion component from tissue diffusion, yielding four functional parameters: ADC, D (tissue diffusion coefficient), D* (pseudo-diffusion coefficient), and f (perfusion fraction)3. Preliminary studies have suggested that quantitative parameters from IVIM imaging at various stages of NAC may predict response4. However, the utility of IVIM parameters for pretreatment prediction of NAC response in breast cancer remains unknown. This study aims to evaluate whether pretreatment IVIM histogram-based parameters can predict pathological response following NAC in breast cancer.Methods
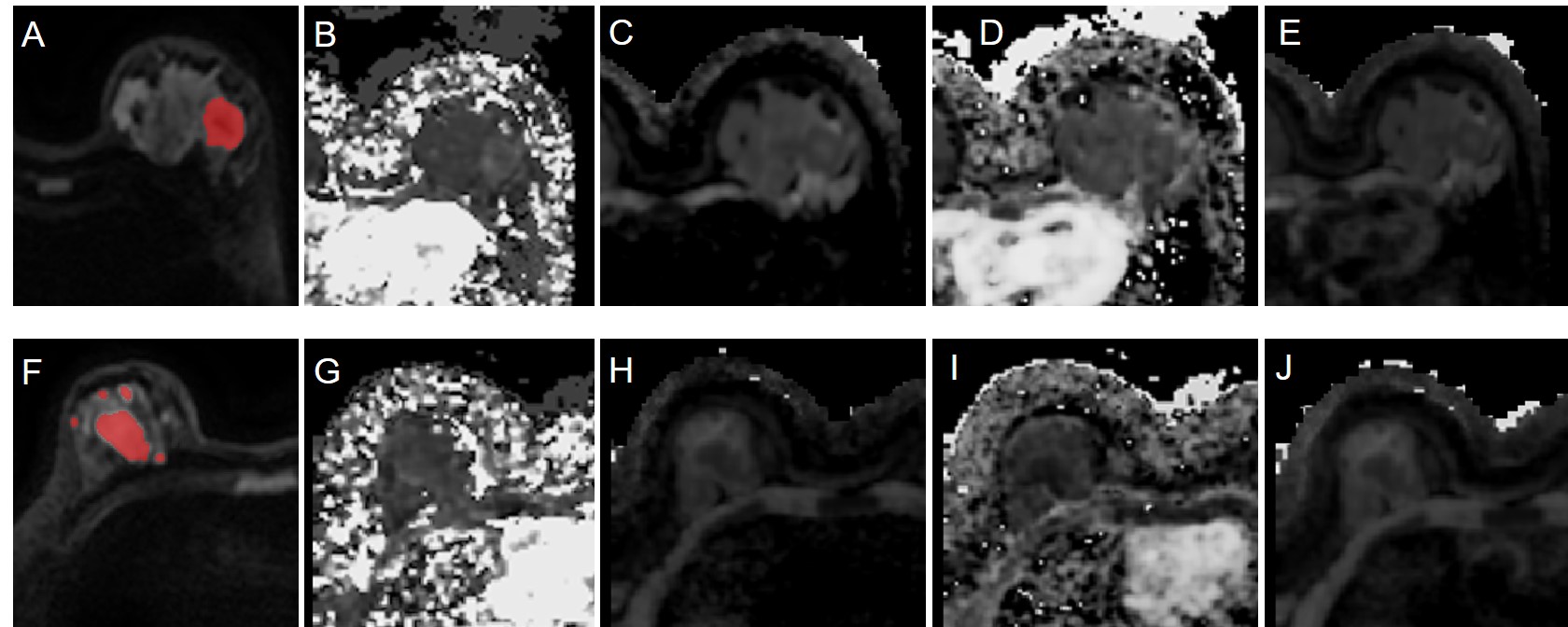
Between December 2010 and December 2022, 287 women diagnosed with breast cancer who underwent breast MRI prior to NAC were enrolled in this study. IVIM model-based maps were generated for apparent diffusion coefficient (ADC), tissue diffusion (D), pseudo-diffusion coefficient (D*), and perfusion fraction (f) using DWI with 10 different b values. Subsequent voxel-wise analysis of tumors allowed for the extraction of histogram features from the four parameter maps. Patients were randomly divided into training and test datasets at a 7:3 ratio. Multivariate logistic regression was employed to select predictors and construct a prediction model. The area under the receiver operating characteristic curve (AUC) and calibration curve were used to evaluate the model's predictive performance in the test dataset.Results
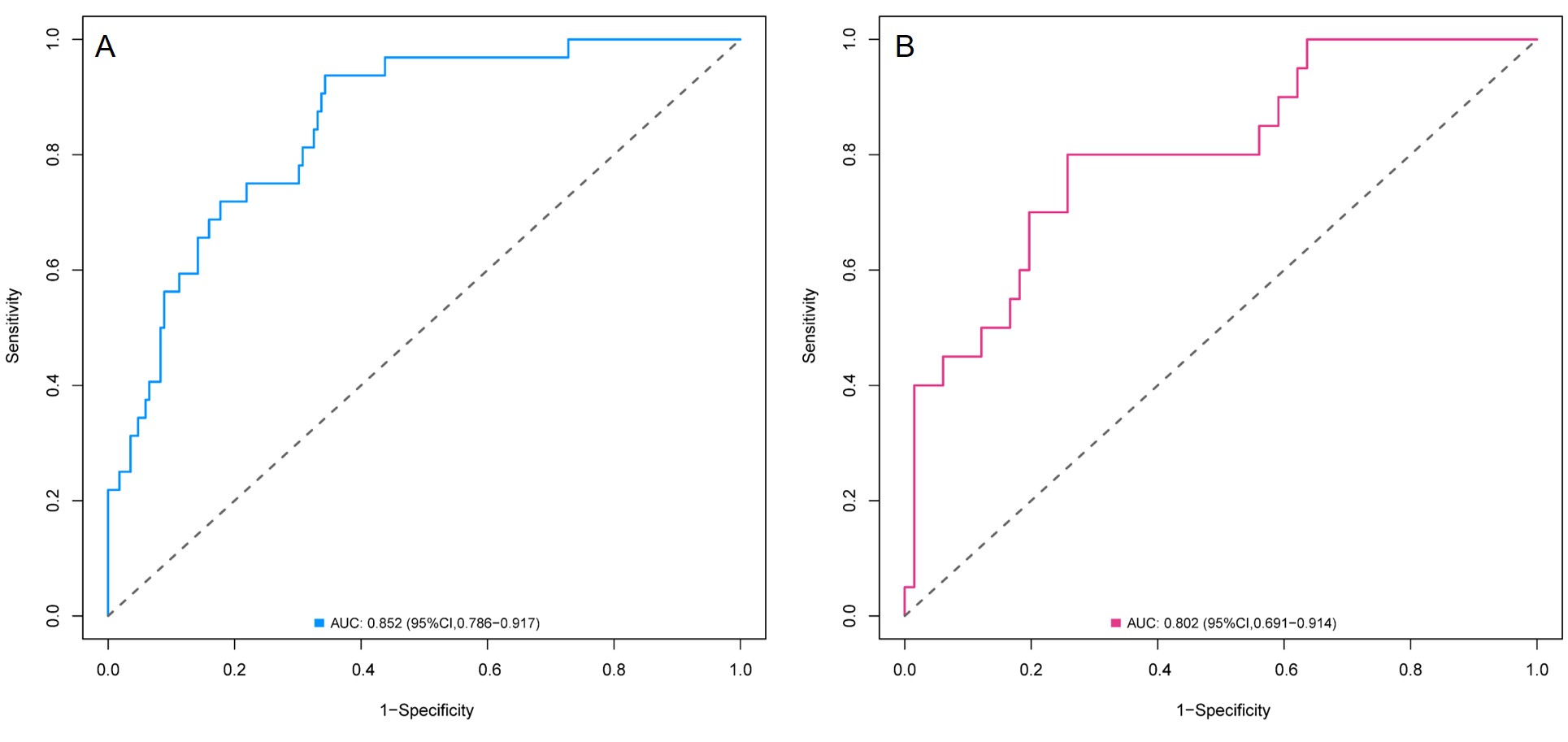
The training dataset included 200 patients (median age: 48 years [IQR, 40–55 years]), while the test dataset comprised 87 patients (median age: 47 years [IQR, 38–54 years]). Patients achieving pCR exhibited lower kurtosis of f and skewness of D* but higher minimum ADC, minimum D, and skewness of D compared to non-pCR patients. The prediction model, which combined skewness of D*, skewness of D, minimum of D, and progesterone receptor (PR) status, demonstrated excellent discriminative performance with AUC values of 0.852 and 0.802 in the training and test datasets, respectively.Discussion
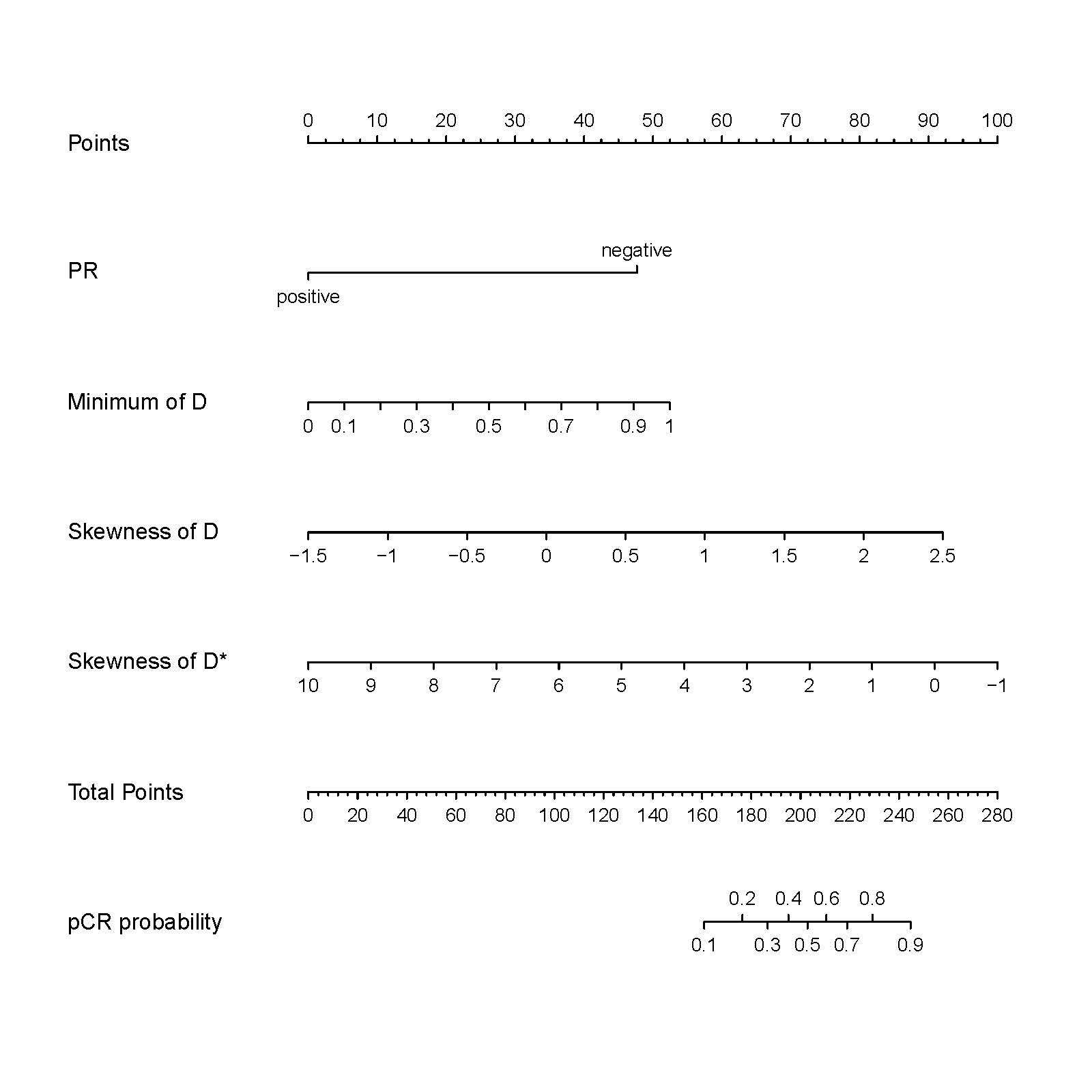
This study successfully developed a prediction model for pCR following NAC, incorporating three quantitative IVIM-derived parameters: skewness of D*, skewness of D, minimum of D, and PR status. The model exhibited strong predictive performance in both the training and test datasets. The International Breast DWI Working Group advocates volume-sampling analysis for assessing treatment response5. Interestingly, we found that the minimum of D before NAC, a volumetric histogram feature, was associated with pCR in breast cancer patients undergoing NAC. This metric reflects the diffusion restriction within the tumor's highest cellular density component, consistent with prior research findings. Skewness, which characterizes the distribution of values, emerged as an independent predictor of pCR in our study. Lower positive skewness of D* in pretreatment breast tumors may favor pCR, possibly due to the asymmetric distribution of the pseudo-diffusion coefficient, linked to capillary network perfusion. Additionally, higher positive skewness of D was associated with pCR, indicating a greater proportion of intratumoral components with high tissue diffusion coefficients.Conclusion
IVIM-derived histogram parameters offer valuable insights into predicting pathological response to NAC in breast cancer. This information can aid clinicians in tailoring treatment strategies more effectively.Acknowledgements
No acknowledgement found.References
1. Ignatiadis M, Sotiriou C. Luminal breast cancer: from biology to treatment. Nat Rev Clin Oncol 2013;10(9):494–506.
2. Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet 2014;384(9938):164–172.
3. Le Bihan D, Breton E, Lallemand D, et al. MR imaging of intravoxel incoherent motions: Application to diffusion and perfusion in neurologic disorders. Radiology 1986; 161(2):401-407.
4. Almutlaq ZM, Wilson DJ, Bacon SE, et al. Evaluation of Monoexponential, Stretched-Exponential and Intravoxel Incoherent Motion MRI Diffusion Models in Early Response Monitoring to Neoadjuvant Chemotherapy in Patients With Breast Cancer-A Preliminary Study. J Magn Reson Imaging. 2022;56(4):1079-1088.
5. Baltzer P, Mann RM, Iima M, et al. Diffusion-weighted imaging of the breast—A consensus and mission statement from the EUSOBI international breast diffusion-weighted imaging working group. Eur Radiol. 2020;30(3):1436-1450.
Figures