2866
Evaluation of Microstructural Brain Abnormalities and Cognitive Impairment of OSAHS patients with axial and radial kurtosis from DKI1The Sixth Hospital of Shanxi Medical University(General Hospital of TISCO), Taiyuan, China, 2GE Healthcare, Beijing, China
Synopsis
Keywords: DWI/DTI/DKI, Nervous system, Obstructive sleep apnea-hypopnea syndrome; cognitive function
Motivation: Microstructural brain changes resulted from obstructive sleep apnea hypopnea syndrome(OSAHS)related cognitive impairment can help to understand the potential neuropathological mechanism.
Goal(s): To assess the brain microstructural alteration in patients with OSAHS using DKI imaging.
Approach: 33 OSAHS patients and 33 healthy controls were performed DKI/3D-T1WI MRI imaging. The AK and RK in different brain regions were extracted.
Results: Significant differences were found in AK and RK values in various brain regions for OSAHS group compared to HC group. Abnormal changes in some crucial brain regions were found to be correlated with MoCA score and sleep parameters.
Impact: Altered AK and RK in brain regions associated with the microstructural change in OSAHS, such as demyelination and axonal destruction. The correlation of respiratory parameters and scoring indicators is conducive to more objective assessment for cognitive level of patients.
INTRODUCTION
Obstructive sleep apnea hypopnea syndrome (OSAHS) is a sleep disorder characterized by excessive snoring, repeated apnea and nocturnal awakening, often accompanied by intermittent hypoxemia, sleep fragmentation1. There has been more evidence that OSAHS can cause neurocognitive impairment, resulting in a decline in work efficiency and life quality2,3. Now there are few studies on the microstructural changes of OSAHS brain based on non-Gaussian diffusion model. We have analyzed MK values in different brain regions and their correlation with clinical scores in last year. This study aims to analyze the axial kurtosis (AK) and radial kurtosis (RK) to explore the changes in different brain regions for patients with OSAHS.METHODS
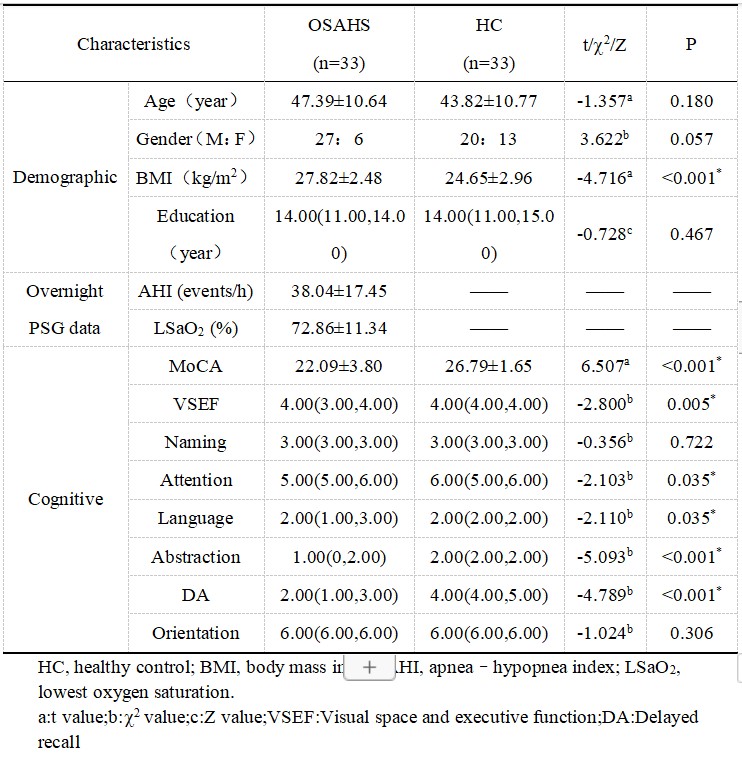
A total of 33 patients with moderate and severe OSAHS diagnosed by overnight polysomnography (PSG) and 33 healthy controls (HC) matched with age, sex and education were collected. All subjects were assessed by Montreal Cognition scale(MoCA) and performed DKI and 3D T1-weighted imaging (T1WI) in a 3T MRI (SIGNA Pioneer, GE Healthcare),with the following acquisition parameters: (1) DKI: TR/TE=12000/88.7ms, b value = 0, 1000, 2000mm2/s, 25 diffusion coding directions for each non-zero b value, FOV =240mm×240mm; (2) 3D T1WI: TR/TE=2384/2.5ms, TI=1000ms, FOV= 240mm×240mm, flip angle = 8°, matrix=224×224, slice thickness = 1.1 mm . The DKI images were post-processed to generate AK and RK maps in iQuant software (GE Healthcare, Beijing, China). Then the maps were registered to the 3D T1WI and transformed to the MNI (Montreal Neurological Institute) space to extract the quantification in each brain region with customized automated anatomical labeling atlas in house-built software (SPM12, Matlab R2015b).The demographic features, PSG and MoCA score as well as the AK/RK quantification were compared between patient and HC group.The partial correlation analysis done in SPSS (v26) was used to analyze the correlation of AK/RK with respiratory sleep parameters or cognitive scores after controlling the potential confounding effects (age, BMI, years of education), p < 0.05 indicated significant difference.RESULTS
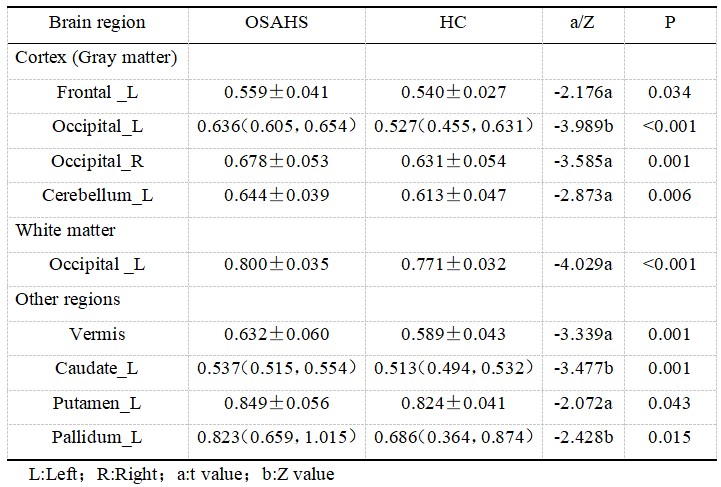
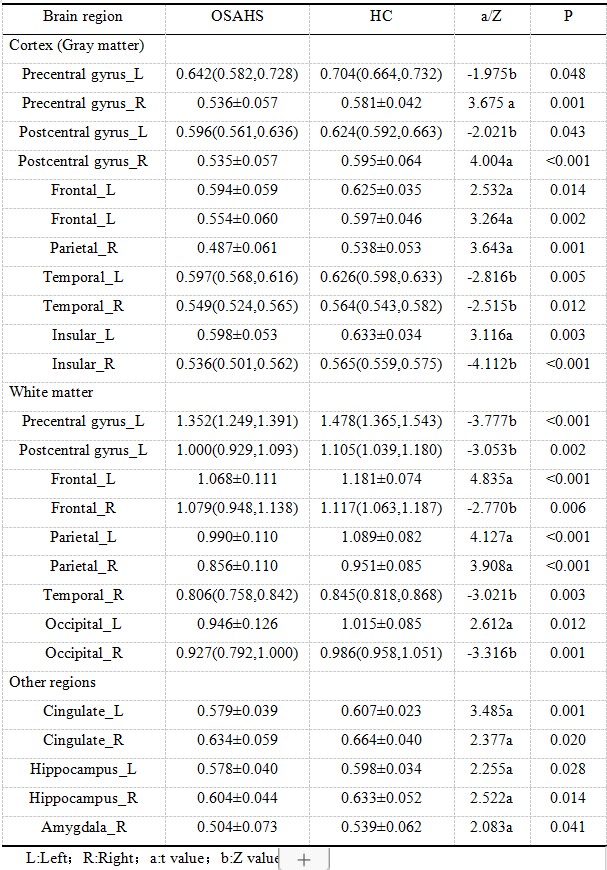
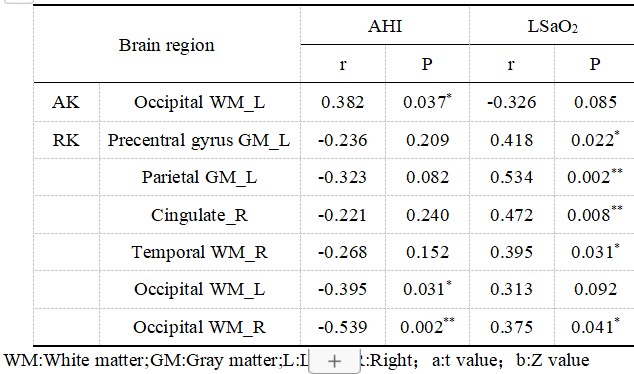
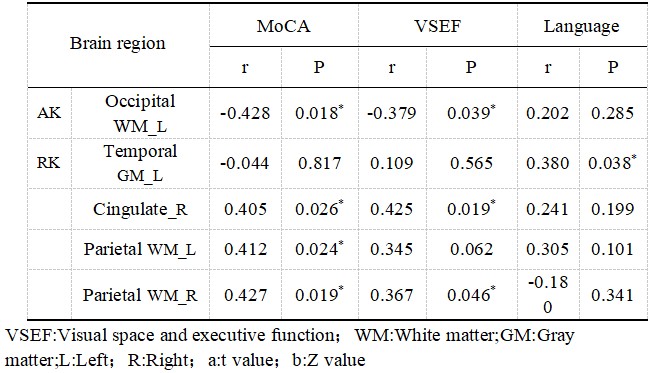
The OSAHS group exhibited higher AK in 9 brain regions and lower RK in 25 brain regions (Table2 and 3) compared to HC group. MoCA scores, including visual space, executive function, attention, language, abstract and delayed recall scores in OSAHS group were significantly lower (Table 1). As shown in Table 4, partial correlation analysis revealed AHI negatively correlating with RK in the white matter of bilateral occipital lobe, and positively with AK in white matter of the left occipital lobe. LSaO2 correlated positively with RK in left precentral gyrus, parietal gray matter, and the right cingulate gyrus, temporal and occipital white matter. Furthermore, in Table 5, the MoCA score correlated positively with the RK in right cingulate gyrus and the white matter in the left and right parietal lobes, and negatively with AK in white matter of left occipital lobe. The visual space and executive function correlated negatively with the AK of the white matter in the left occipital lobe, but positively with the RK values in right cingulate gyrus and parietal white matter. The language function positively correlated with RK in gray matter of left temporal lobe.DISCUSSION
AK measure diffusion kurtosis along axon fiber, indicating axon integrity, while RK measure the radial diffusion kurtosis, reveling myelin sheath integrity 4,5. Chronic intermittent hypoxia and hypercapnia during sleep in patients with OSAHS can trigger molecular and cellular events, resulting in changes in myelin, axons, neuronal branches or synaptic density, glial cells, myelin-supporting oligodendrocytes and so on. In acute stage of hypoxia, increased axon and myelin swelling, as well as glial cells and tissue heterogeneity lead to higher AK and RK. In chronic condition, axonal destruction, demyelination, neuronal loss and other pathological changes occur, resulting in reduced tissue heterogeneity and decreased AK and RK values 6,7. Brain regions in the OSAHS group exhibited higher AK and lower RK, suggesting ongoing axonal injury in the acute stage, and myelin injury progressed to a chronic stage.The results of correlation analysis showed that the values of AK and RK in some brain regions were correlated with respiratory sleep parameters and cognitive scores. This may suggest that with the aggravation of the severity of the disease, the damage of brain microstructure will be further aggravated, which will lead to cognitive impairment in OSAHS patients.
CONCLUSION
The altered AK and RK values in multiple brain regions in OSAHS group indicates the presence of brain tissue microstructure damage. Moreover, the abnormal alterations in brain microstructure were significantly correlated with sleep monitoring and cognitive scores. The DKI kurtosis could serve as quantitative imaging indices, allowing exploration of potential mechanism related to neuropathological impairment in OSAHS.Acknowledgements
The authors acknowledge grant support from The Sixth Hospital of Shanxi Medical University and GE Healthcare.References
1. Veasey SC, Rosen IM. Obstructive Sleep Apnea in Adults. N Engl J Med.2019;380(15):1442-1449.
2. Seda G, Han TS. Effect of obstructive sleep apnea on neurocognitive performance. Sleep Med Clin. 2020;15(1): 77-85.
3. Shieu MM, Dunietz GL, Paulson HL, et al. The association between obstructive sleep apnea risk and cognitive disorders: a population-based study. J Clin Sleep Med. 2022 ;18(4):1177-1185.
4. Marrale M, Collura G, Brai M, et al. Physics, Techniques and Review of Neuroradiological Applications of Diffusion Kurtosis Imaging (DKI). Clin Neuroradiol.2016;26(4):391-403.
5. Xie Y, Zhang Y, Qin W, et al. White Matter Microstructural Abnormalities in Type 2 Diabetes Mellitus: A Diffusional Kurtosis Imaging Analysis. AJNR Am J Neuroradiol.2017;38(3):617-625.
6. Tummala S, Roy B, Vig R, et al. Non-Gaussian Diffusion Imaging Shows Brain Myelin and Axonal Changes in Obstructive Sleep Apnea. J Comput Assist Tomogr.2017;41(2):181-189.
7. Vyas S, Singh P, Khandelwal N,et al. Evaluation of cerebral microstructural changes in adult patients with obstructive sleep apnea by MR diffusion kurtosis imaging using a whole-brain atlas. Indian J Radiol Imaging.2019 ;29(4):356-363.
Figures