2865
Feasibility of high b value in vivo cardiac diffusion in humans with ultra-high gradient strength scanner1Cardiovascular Innovation Research Center, Heart Vascular Thoracic Institute, Cleveland Clinic, Cleveland, OH, United States, 2Siemens Medical Solutions USA, Inc., Cleveland, OH, United States, 3Siemens Medical Solutions USA, Inc, Los Angeles, CA, United States, 4Cardiovascular Medicine, Heart Vascular Thoracic Institute, Cleveland Clinic, Cleveland, OH, United States, 5Imaging Institute, Cleveland Clinic, Cleveland, OH, United States, 6Department of Biomedical Engineering, Case Western Reserve University & Cleveland Clinic, Cleveland, OH, United States
Synopsis
Keywords: DWI/DTI/DKI, Diffusion Tensor Imaging
Motivation: New technology allows for higher gradient strengths and therefore higher b-values to be used in cardiac diffusion tensor imaging (cDTI).
Goal(s): To compare cDTI parameter maps for the current standard and increased b-values both qualitatively and quantitatively.
Approach: Two cDTI datasets with b=500 s/mm2 and b=1000s/mm2 were acquired from nine healthy subjects. The resulting DTI parameter maps were compared through visual analysis and a series of paired t-tests.
Results: Both qualitative and quantitative data between parameter maps show improved detail and higher precision in high b-value data compared to standard b-value data.
Impact: A new ultra-high-performance 3T MR system allows for higher diffusion gradients and b-values. Our study shows high b-values (b=1000 s/mm2) lead to higher levels of detail and precision in cardiac DTI of healthy subjects compared to standard b-values (b=500 s/mm2).
Introduction
Cardiac diffusion tensor imaging (cDTI) is a non-invasive magnetic resonance imaging (MRI) technique that allows for an in-vivo analysis of myocardial microstructure1. With the introduction of a new 3T MR system (MAGNETOM Cima.X, Siemens Healthineers AG, Erlangen, Germany), higher gradients can be achieved allowing for in-vivo spin-echo based cDTI in humans with high b-value. In the brain, previous studies have shown that higher b-values show increased contrast between lesions and healthy tissue2. Similarly, in cDTI, high b-value DTI acquisitions could allow for enhanced detection of changes in myocardial structure due to phenotypic variations as is observed in cardiovascular disease. The goal of this study is to compare the image quality and cDTI parameter quantification at b = 500 s/mm2 and b = 1000s/mm2 on an ultra-high gradient MR system.Methods
Nine healthy volunteers (mean age 27.6 years, six female) were recruited with approval from the institutional review board of the Cleveland Clinic. Diffusion tensor imaging with second-order motion compensating (M2), diffusion prepared spin echo sequences was performed during free breathing on a 3T investigational MR system (MAGNETOM Cima.X, Siemens Healthineers AG, Erlangen, Germany) that has a maximum gradient strength Gmax=200 mT/m (12 diffusion directions, 8 averages, b0=50 s/mm2 with 1 average, 2.7 x 2.7 mm resolution, 8 mm slice thickness, 128x48 matrix, TR=500 ms, end systole). In a single session, complete DTI datasets were acquired with b=500 s/mm2 (b500) and b=1000 s/mm2 (b1000) for all volunteers. Post-processing was done using a custom code in python which consisted of low rank tensor motion correction of the DW images3, and calculation of the mean diffusivity (MD), fractional anisotropy (FA), and helix angle (HA). Mean and standard deviation values of MD, FA, and helix angle transmurality (HAT) in the left ventricle (LV) were calculated from manual segmentations. Statistical analysis was done using GraphPad Prism (v9.5.1) to perform a series of paired t-tests comparing the FA, MD, HAT, and the standard deviations of FA and MD from the b500 and b1000 data.Results
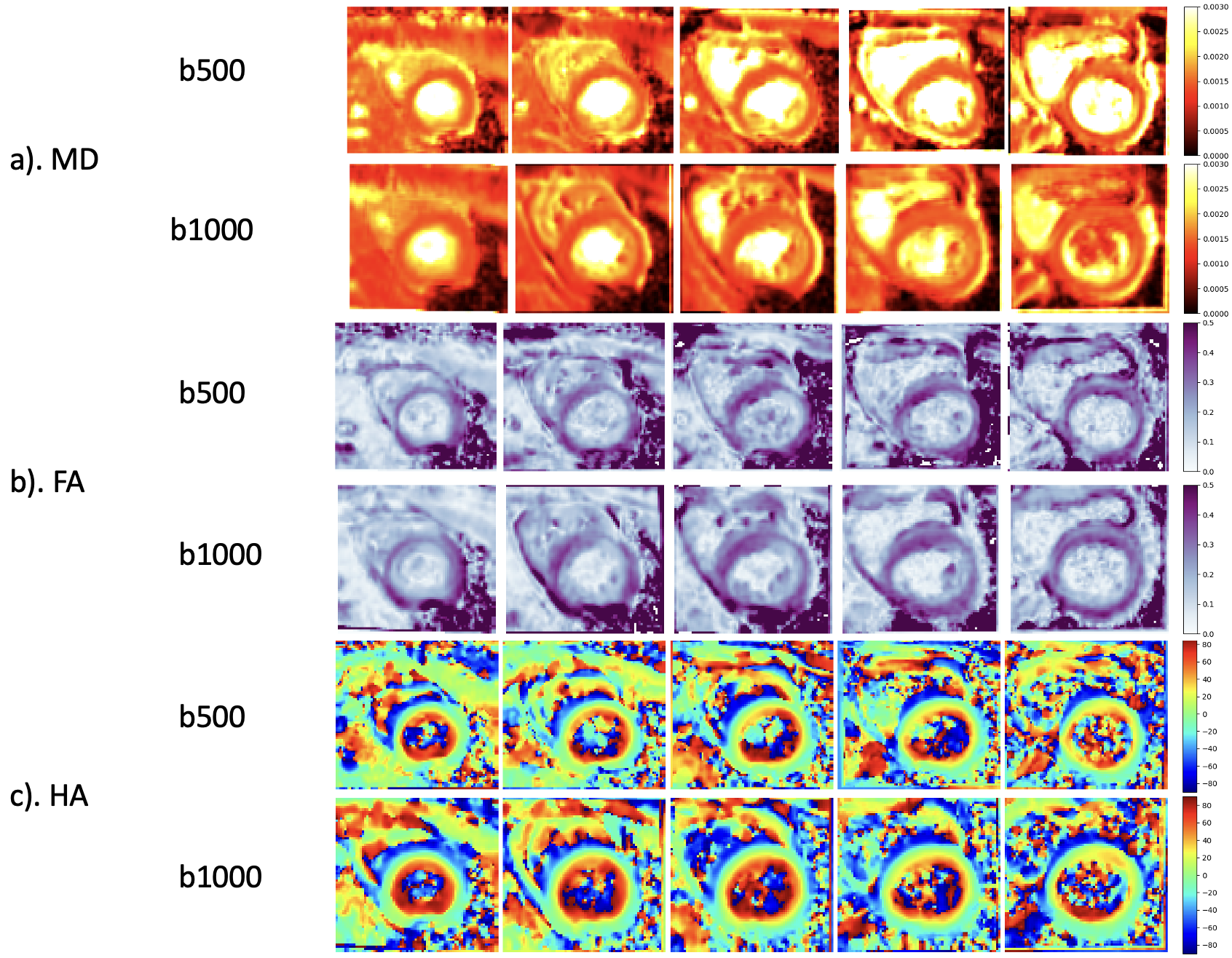
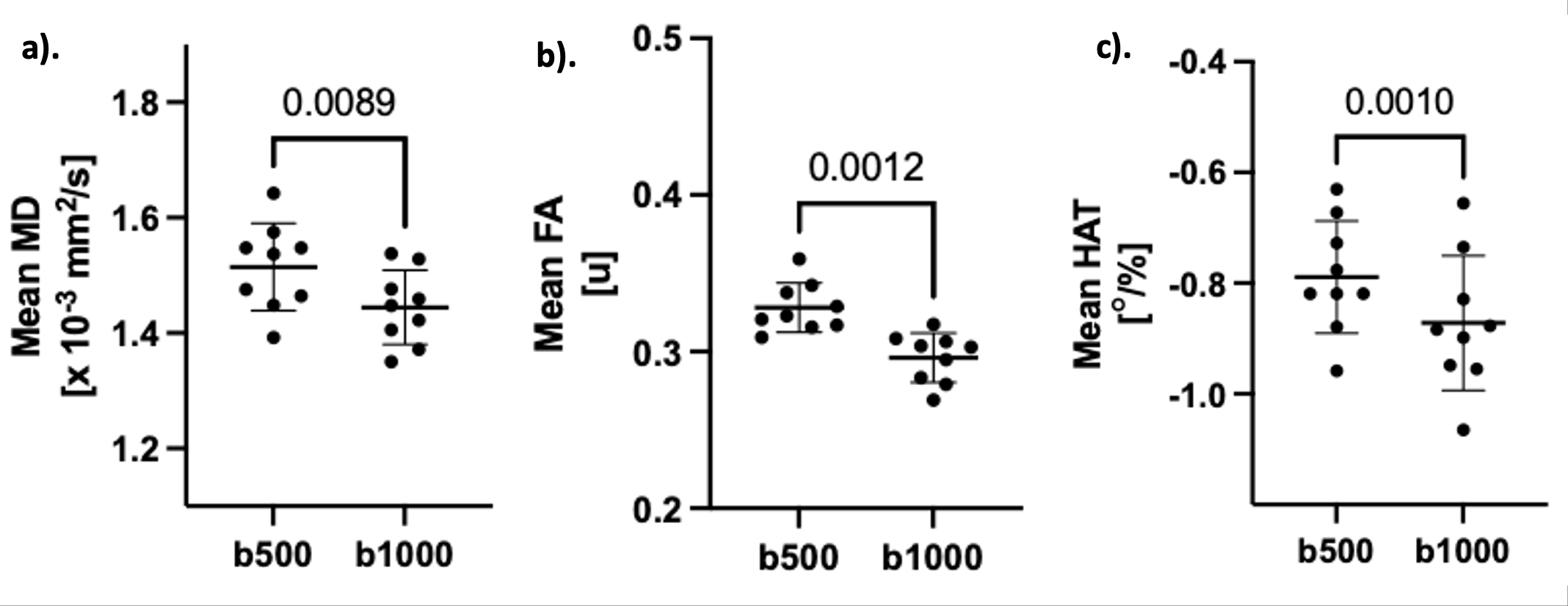
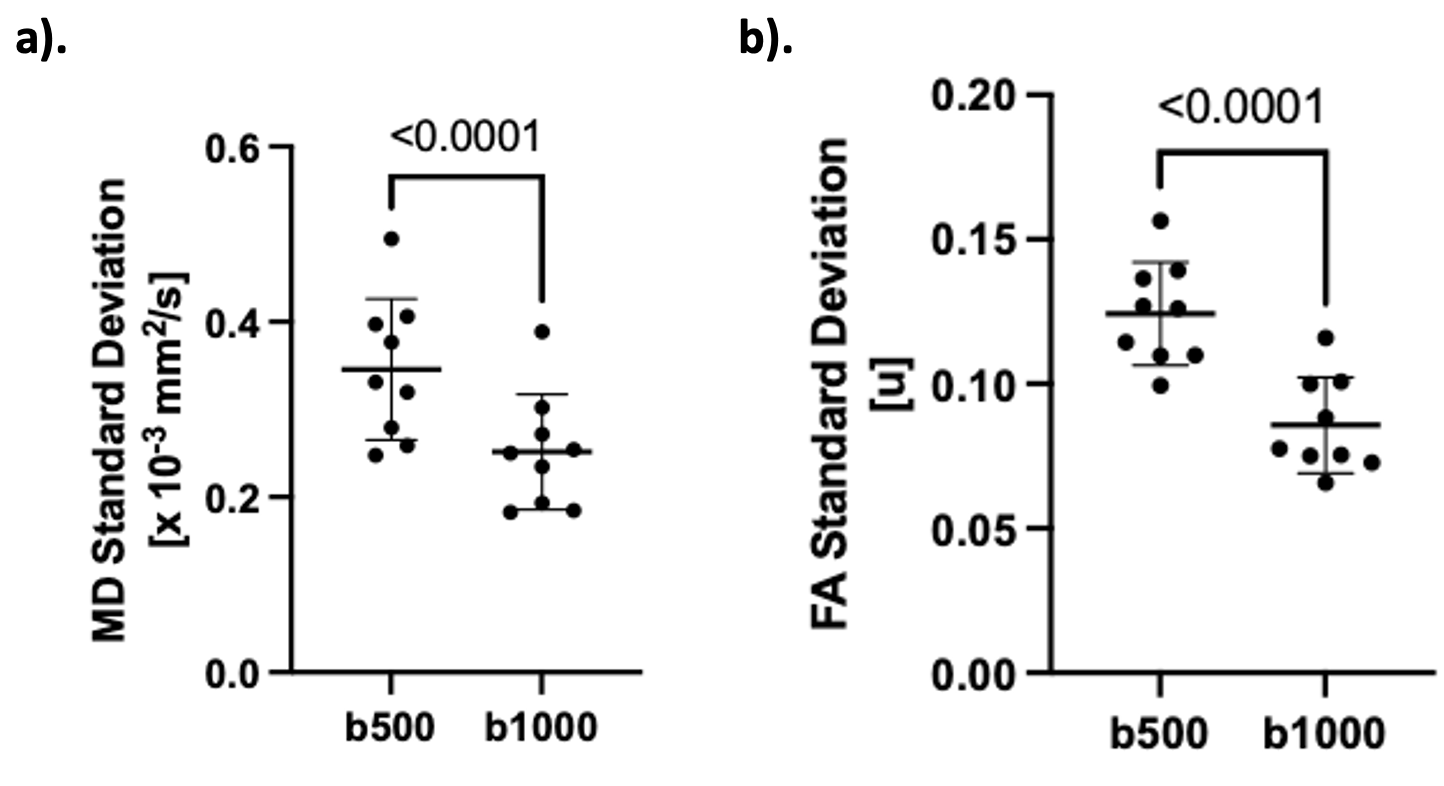
Calculated MD, FA, and HA maps for both b500 and b1000 data from one representative volunteer are shown in Figure 1. In the MD and FA maps, there are noticeable visual differences in the smoothness of the left ventricular wall with more unstructured variance observed in the b500 maps in comparison to b1000’s smooth, gradual changes. In the HA maps, b1000 appears to have much deeper blues and reds visually, and a more clearly defined transition from right to left-handed helical structure when traversing from endocardium to epicardium. Box plots of the paired t-tests comparing the mean MD, FA, and HAT for b500 and b1000 data can be seen in Figure 2. b1000 was shown to have decreased values for all three parameters. The paired t-tests yield p-values of 0.0089, 0.012, and 0.001, respectively, indicating significant difference in the mean MD, FA, and HAT values obtained for the b500 and b1000 data. The box plots for the paired t-tests of the comparison between b500 and b1000 for the standard deviations of MD and FA can be seen in Figure 3. The standard deviations for b1000 are distinctively lower than those of b500 for both MD and FA. The differences in the standard deviations across the LV are both shown to be statistically significant (p < 0.0001).Discussion
Increasing the b value from b = 500 s/mm2 to b = 1000 s/mm2 yields significant differences in the quantification of DTI parameters, including mean diffusivity, fractional anisotropy, and helix angle transmurality in healthy volunteers. In addition, significantly lower standard deviations for MD and FA in the LV indicate that more precise DTI maps can be generated from data acquired with b = 1000 s/mm2 than with b = 500 s/mm2. Increased precision in the b1000 maps can be attributed to the higher diffusion contrast in DW images acquired with the higher b-value.Conclusion
Use of an increased b-value in human, in-vivo cardiac DTI leads to more precise results with improved detail visualization when compared to standard b-values.Acknowledgements
This work was supported by NIHLBI (R01 HL151704, R01 HL159010) and NIBIB (R01 EB033853). We thank the Imaging Institute and the Cardiovascular Innovation Research Center for their support.References
- Dou, J., Reese, T. G., Tseng, W. Y. I., & Wedeen, V. J. (2002). Cardiac diffusion MRI without motion effects. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine, 48(1), 105-114.
- Dudink, J., Larkman, D. J., Kapellou, O., Boardman, J. P., Allsop, J. M., Cowan, 2.F. M., ... J.V. Hajnal, A.D. Edwards, M.A. Rutherford & Counsell, S. J. (2008). High b-value diffusion tensor imaging of the neonatal brain at 3T. American journal of neuroradiology, 29(10), 1966-1972.
- Nguyen CT, Christodoulou AG, Coll‐Font J, Ma S, Xie Y, Reese TG, et al. Free‐breathing diffusion tensor MRI of the whole left ventricle using second‐order motion compensation and multitasking respiratory motion correction. Magn Reson Med. 2021 May;85(5):2634–48.
Figures