2857
Non-complete Recovery of White Matter Diffusion Metrics at One Year Post-Radiotherapy: Implications for Radiation-Induced Necrosis Risk1Sun Yat-Sen University Cancer Center, Guangzhou, China, 2School of Biomedical Engineering, Southern Medical University, Guangzhou, China, 3Guangdong Provincial Key Laboratory of Medical Image Processing and Guangdong Province Engineering Laboratory for Medical Imaging and Diagnostic Technology, Southern Medical University, Guangzhou, China
Synopsis
Keywords: DWI/DTI/DKI, Head & Neck/ENT, nasopharyngeal carcinoma, radiation-induced TL necrosis, multi-shell diffusion MRI, automated fiber-tract quantification, Cox proportional-hazards regression model, Normal Tissue Complication Probability
Motivation: Radiotherapy for nasopharynx carcinoma (NPC) can lead to various white matter (WM) abnormalities.
Goal(s): Explores the connection between WM injuries and temporal lobe necrosis (TLN) and optimizing radiotherapy (RT) regimens for NPC.
Approach: Multi-shell diffusion MRI (MS-dMRI) quantification using automated fiber-tract quantification (AFQ). Diffusion metrics alterations analysis using rANOVA. TLN risk factors identification using Cox regression models. Optimal RT regiments development using normal tissue complication probability (NTCP) models.
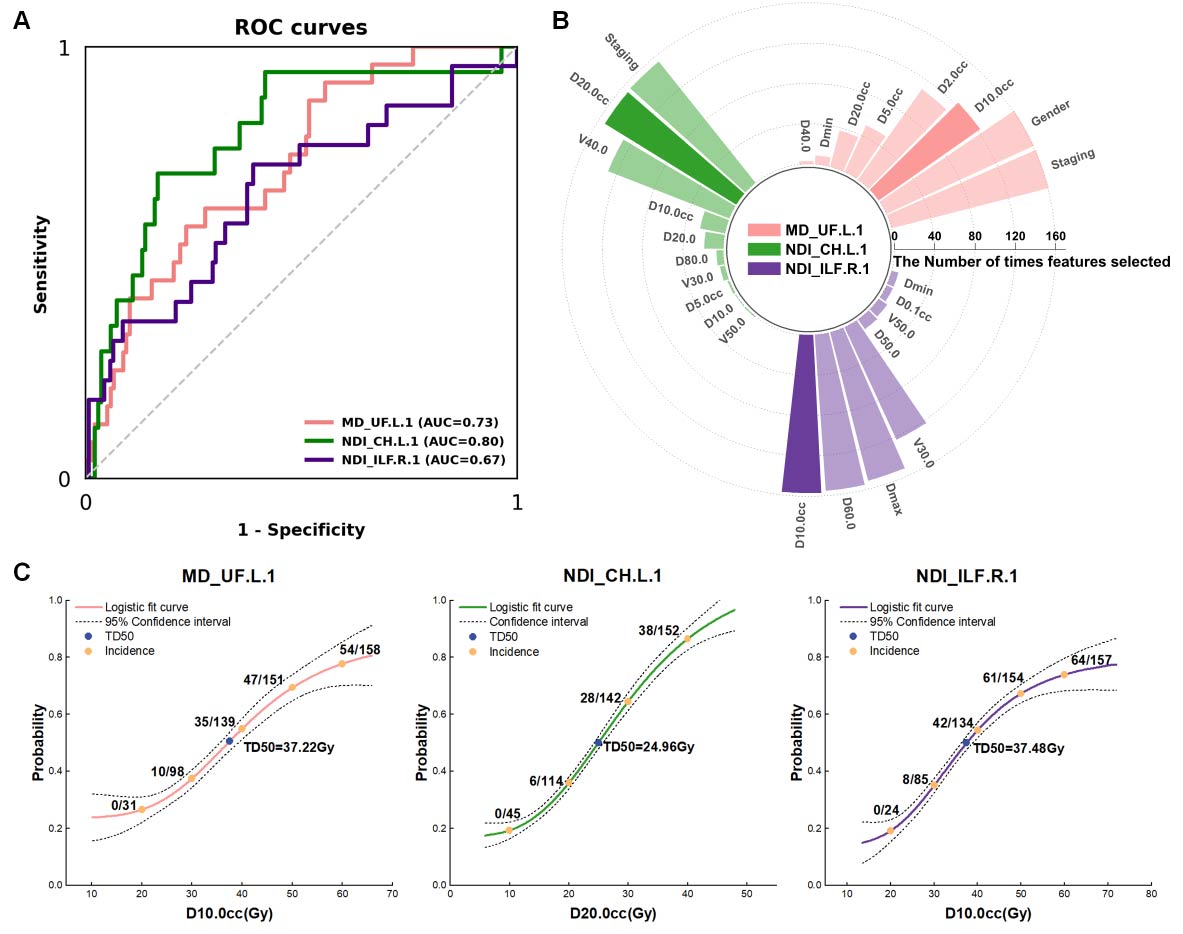
Results: Most TL WM tract segments showed a "decrease/increase without complete recovery" pattern. MD_UF.L.1, NDI_CH.L.1, and NDI_ILF.R.1 were identified as TLN risk predictors. Tolerance dose for D10cc.L, D20cc.L and D10cc.R were revealed for optimal regiments.
Impact: Our findings highlight the importance of "decrease/increase without complete recovery" pattern in TL WM tract segment impairments in TLN development. Identifying high-risk WM tract segments and their tolerance doses can aid in optimizing radiotherapy regimens for NPC.
Background
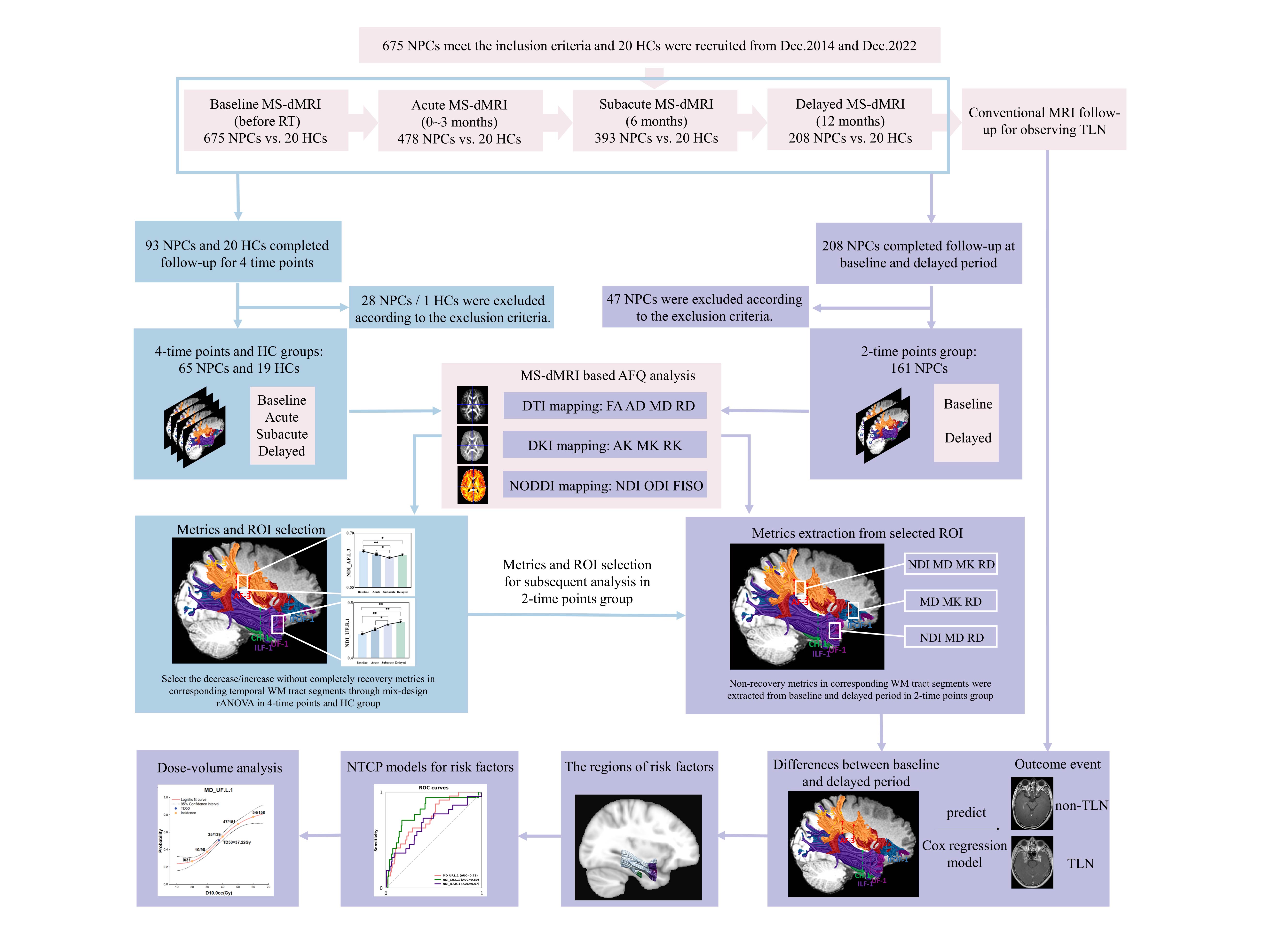
Recent studies revealed that the radiotherapy (RT)-induced temporal lobe (TL) white matter (WM) microstructural injuries occurs early in nasopharyngeal carcinoma patients (NPCs) [1], but some does not fully recovery in the delayed period yet [2]. Based on previous preclinical studies [3-5], we hypothesize that non-complete recovery TL WM tract segments have close relationship with TLN. Thus, in this exploratory study, we aimed to investigate the characteristic of TL WM segmental impairments using multi-shell diffusion MRI (MS-dMRI) [2] based AFQ technology [6] at multiple time points (baseline, acute, subacute and delayed period) [1], and find out the non-recovery injury of TL WM tract segments which still show no recovery in delayed period after RT in NPC patients. The secondary goal of this study was to investigate the role of non-recovery WM tract segmental impairments in the development of TLN. Furthermore, we hypothesized that assessing the dose tolerance of these vulnerable WM tract segments will aid in the optimalization of RT plans to decrease risk of TLN in clinical practice [7]. Therefore, the third aim of the study was constructing NTCP models and investigating the tolerance doses of TLN high-risk WM tract segments.Methods
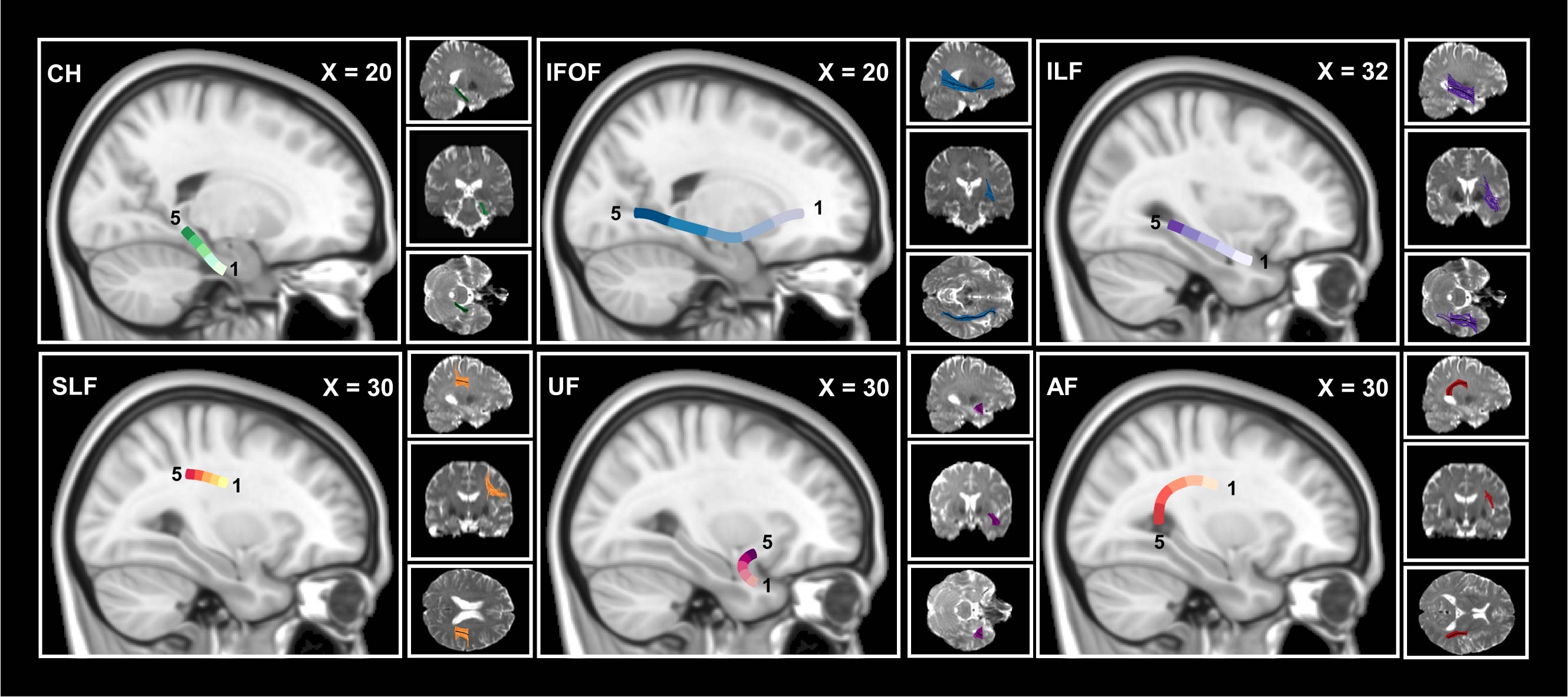
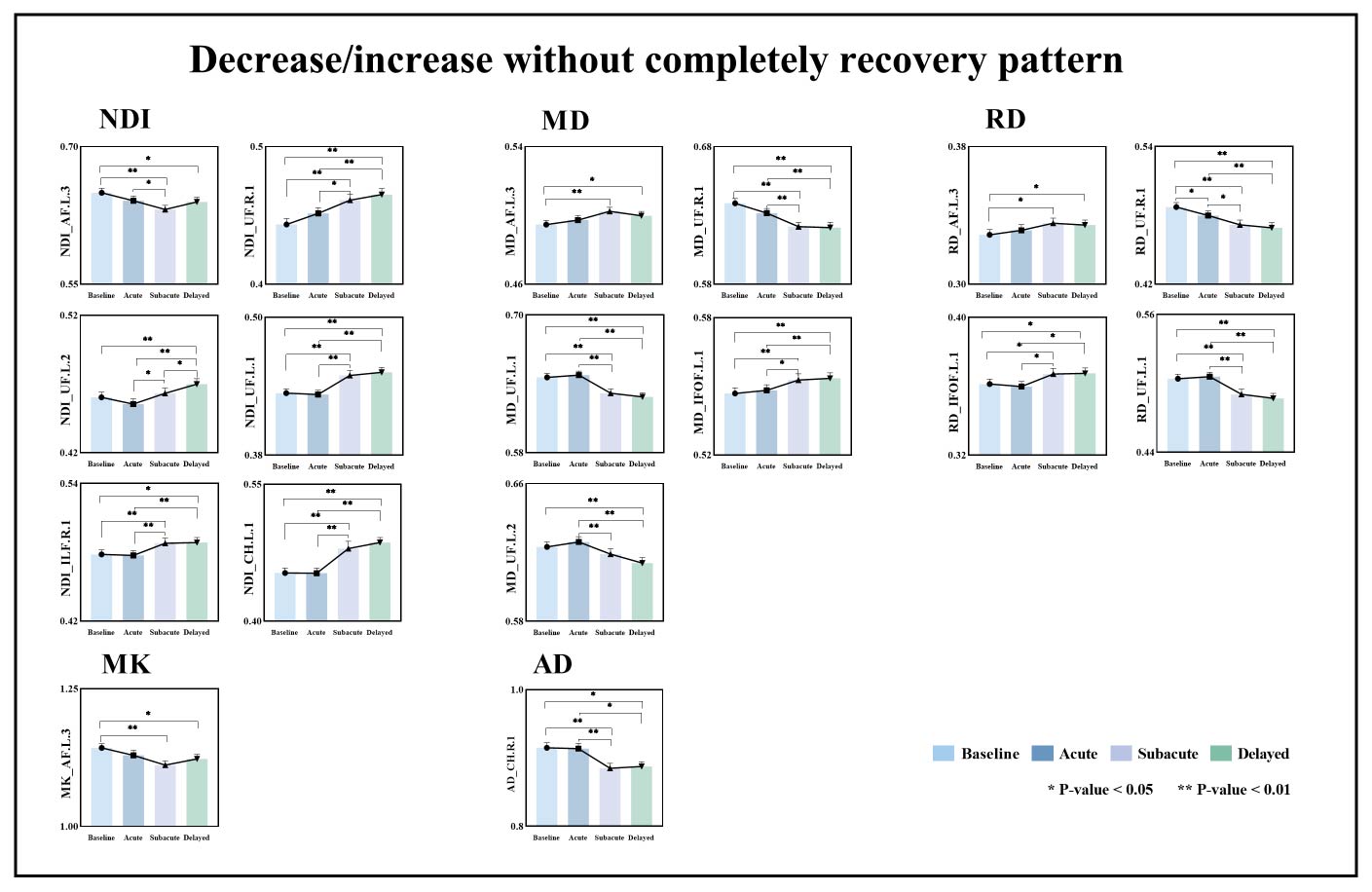
We longitudinally examined 161 NPC patients (NPCs) and 19 healthy controls (HCs) using MS-dMRI [2]. The diffusion parameters of bilateral temporal lobe (TL) WM tracts were segmentally quantified by automated fiber-tract quantification (AFQ) [6]. Mix-designed rANOVA was computed to investigate the dynamic alterations of diffusion metrics and found the non-complete recorvery WM tract segments in one-year follow-up NPC patients after RT (P < 0.05). Cox regression models identified TLN risk factors utilizing non-complete recovery diffusion parameters from follow-up NPC patients [8]. Normal tissue complication probability (NTCP) models and dose-response analysis were conducted to further investigate RT-related toxicity to these high-risk WM tract segments [7].Results
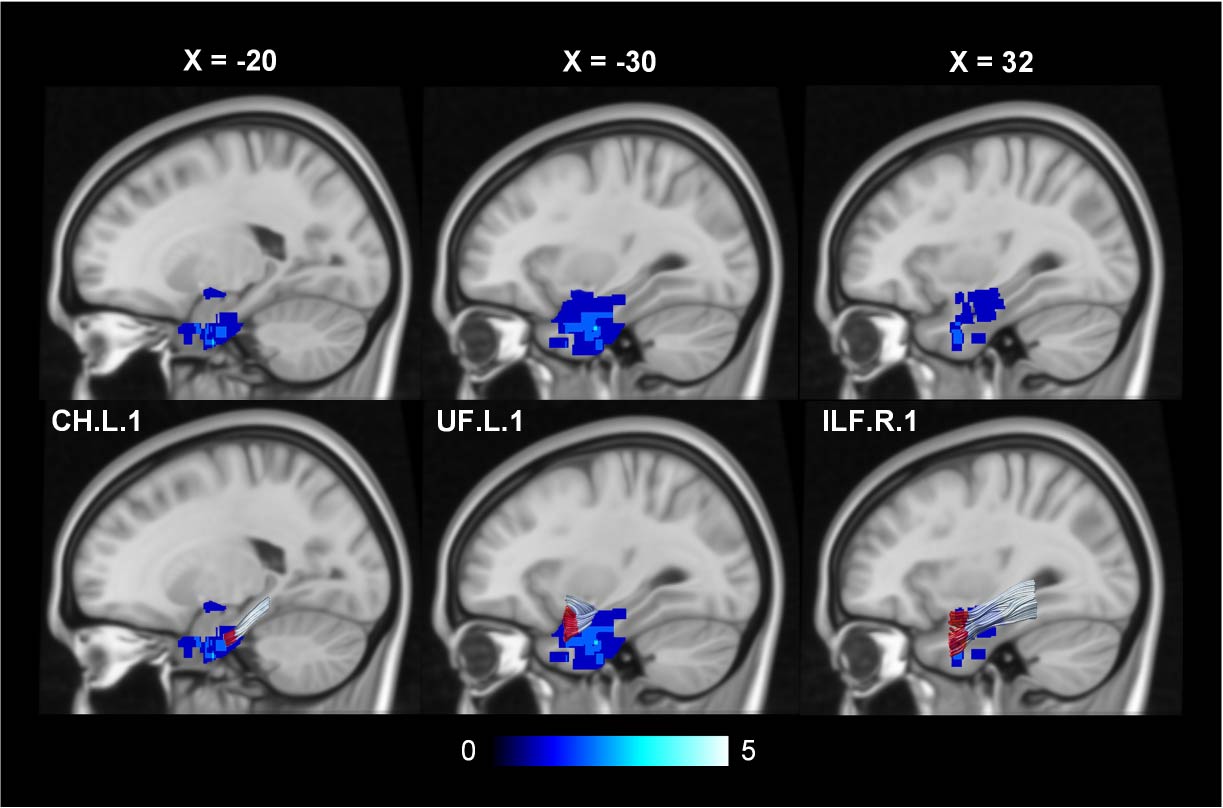
In this present study, AFQ analysis based on MS-dMRI were applied to investigate the characteristic of longitudinal changes of TL WM tract segments after RT in NPC patients one-year post-RT. Dominant diffusion metrics of WM tract segments showed ‘‘decrease/increase without completely recovery pattern” over time. Furthermore, we have shown the MD_UF.L.1 and NDI_CH.L.1 and NDI_ILF.R.1 in the decrease/increase without completely recovery pattern were the independent risk factors for the left- and right-TLN occurrence, respectively. Finally, with the aim to optimize RT treatment planning for NPC, NTCP models were constructed for these TLN high-risk WM tract segments. The dose-response analysis shows the tolerance dose for the most critical dosimetry variables, including D10cc.L, D20cc.L, and D10cc.R with TD50 of 37.22-Gy, 24.96-Gy and 37.48-Gy equivalents, respectively. As a result, our findings investigated that the non-recovery WM tract segmental quantification metrics were the high-risk factors of TLN, and dose analysis could provide dose references for optimal RT regimens in clinical practice.Conclusions
Our study demonstrated that the “decrease/increase with completely recovery” pattern was the dominant WM impairments pattern in TLs and three WM tract segments among this pattern was proved to be risk factors of TLN. Subsequently, NTCP models for these risk factors were constructed and dose-response relationship were analyzed which hopefully provided dose reference of RT regimens optimization and target volume delineation for NPC patients. Overall, our findings underscore the value of non-recovery WM tract segments quantifying metrics in risk prediction of TLN and provided opportunities to optimize RT regimens above the basis.Acknowledgements
This work was supported by the Natural Science Foundation of Guangdong Province, China (Grant No. 2019A1515011143)References
[1] Z. Zheng, B. Wang, Q. Zhao, Y. Zhang, J. Wei, L. Meng, Y. Xin, X. Jiang, Research progress on mechanism and imaging of temporal lobe injury induced by radiotherapy for head and neck cancer, European Radiology. 32 (2022) 319–330. https://doi.org/10.1007/s00330-021-08164-6.
[2] J. Liang, X. Zhang, Y. Lin, G. Fu, J. Pan, Y. Feng, X. Lv, Disparate Radiation-Induced Microstructural Injuries in Whole-Brain White Matter of Patients With Nasopharyngeal Carcinoma: A Longitudinal Study Using Multishell Diffusion MRI, J Magn Reson Imaging. (2023). https://doi.org/10.1002/jmri.28674.
[3] H.Z. Wang, S.J. Qiu, X.F. Lv, Y.Y. Wang, Y. Liang, W.F. Xiong, Z.B. Ouyang, Diffusion tensor imaging and 1H-MRS study on radiation-induced brain injury after nasopharyngeal carcinoma radiotherapy, Clin Radiol. 67 (2012) 340–5. https://doi.org/10.1016/j.crad.2011.09.008.
[4] W.F. Xiong, S.J. Qiu, H.Z. Wang, X.F. Lv, 1H-MR spectroscopy and diffusion tensor imaging of normal-appearing temporal white matter in patients with nasopharyngeal carcinoma after irradiation: initial experience, J Magn Reson Imaging. 37 (2013) 101–8. https://doi.org/10.1002/jmri.23788.
[5] X. Zhang, J. Pan, Y. Lin, G. Fu, P. Xu, J. Liang, C. Ye, J. Peng, X. Lv, Y. Yang, Y. Feng, Structural network alterations in patients with nasopharyngeal carcinoma after radiotherapy: A 1-year longitudinal study, Front Neurosci. 16 (2022) 1059320. https://doi.org/10.3389/fnins.2022.1059320.
[6] S.S. Keller, G.R. Glenn, B. Weber, B.A.K. Kreilkamp, J.H. Jensen, J.A. Helpern, J. Wagner, G.J. Barker, M.P. Richardson, L. Bonilha, Preoperative automated fibre quantification predicts postoperative seizure outcome in temporal lobe epilepsy, Brain. 140 (2017) 68–82. https://doi.org/10.1093/brain/aww280.
[7] D.W. Wen, L. Lin, Y.P. Mao, C.Y. Chen, F.P. Chen, C.F. Wu, X.D. Huang, Z.X. Li, S.S. Xu, J. Kou, X.L. Yang, J. Ma, Y. Sun, G.Q. Zhou, Normal tissue complication probability (NTCP) models for predicting temporal lobe injury after intensity-modulated radiotherapy in nasopharyngeal carcinoma: A large registry-based retrospective study from China, Radiother Oncol. 157 (2021) 99–105. https://doi.org/10.1016/j.radonc.2021.01.008.
[8] L. Mah, M.A. Binns, D.C. Steffens, Alzheimer’s Disease Neuroimaging Initiative, Anxiety symptoms in amnestic mild cognitive impairment are associated with medial temporal atrophy and predict conversion to Alzheimer disease, Am J Geriatr Psychiatry. 23 (2015) 466–476. https://doi.org/10.1016/j.jagp.2014.10.005.
Figures