2819
Deep learning-based acceleration of compressed SENSE brain ASL MRI using 3D Cartesian TSE with improved spatial resolution1Philips Healthcare, Shanghai, China, 2MR R&D, Philips Healthcare, Suzhou, China, 3MR Application, Philips Healthcare, Suzhou, China
Synopsis
Keywords: Machine Learning/Artificial Intelligence, Brain, ASL, 3D Cartesian TSE, CS-AI, Deep Learning
Motivation: Brain ASL images are frequently obtained at relatively low spatial resolutions, necessitating a desire for higher-resolution ASL MRI without extended scan times.
Goal(s): To evaluate the potential of employing CS-AI for accelerating higher-resolution brain ASL MRI
Approach: Acceleration of higher-resolution 3D Cartesian TSE ASL MRI was achieved using CS-AI at 2, 3, and 4-fold rates, and its performance was compared with SENSE.
Results: CS-AI-accelerated 3D brain ASL images exhibited good SNR and quality, surpassing those acquired with SENSE, without affecting CBF quantification.
Impact: This investigation may improve the clinical utility of brain ASL, particularly in quantifying perfusion alterations in small-sized lesions.
Introduction
3D Spiral TSE and GraSE techniques are often recommended for brain Arterial Spin Labeled (ASL) MRI due to their high Signal-to-Noise Ratio (SNR) and compatibility with optimized background suppression [1]. However, these methods can be challenging in regions with increased B0 inhomogeneities (such as the skull base), potentially leading to signal loss and geometric distortion. An alternative approach, 3D Cartesian TSE, shows promise for ASL and has demonstrated increased robustness to B0 inhomogeneities in both brain and kidney ASL applications [2-4]. Nevertheless, due to its inherently lower SNR, brain ASL images are often acquired at reduced spatial resolutions (e.g., 3.5x3.5x6mm³), prompting a desire for higher resolution ASL imaging within clinically-feasible scan times. Recently, a compressed sensing artificial intelligence (CS-AI) framework, leveraging an adaptive-CS-Network, has emerged as a potential solution to accelerate various MR imaging techniques, demonstrating promise across different applications [5]. Consequently, this study aims to assess the viability of utilizing CS-AI to accelerate brain ASL imaging using 3D Cartesian TSE with higher spatial resolution.Methods
Pseudo-continuous ASL (pCASL) with background suppression (BGS) was used for brain perfusion imaging on a 3T Philips scanner under IRB approval. (Ingenia Elition, Philips Healthcare, Best, The Netherlands). Five healthy volunteers were scanned in an axial orientation. Vendor-supplied 3D TSE Cartesian acquisition with low-high profile ordering and a radial turbo direction was used. Other parameters were: TR/TE = 4700/12 ms, FOV = 240x240x96 mm3, matrix = 96x96 with 32 slices, acquired resolution = 2.5x2.5x6 mm3, reconstructed resolution = 2.15x2.15x3 mm3, ETL = 80, echo spacing = 2.1 ms, label duration = 1.8 s, post-label delay = 1.8 s, NSA = 1, and 4 BGS pulses. CS-SENSE acquisitions with 2-fold, 3-fold, and 4-fold accelerations were performed in 2:50 min, 1:53 min, and 1:34 min respectively, and the acquired data were subsequently reconstructed with a vendor-supplied artificial intelligence (AI)-based algorithm. Additionally, for comparison, SENSE acquisitions, with 2-fold, 3-fold, and 4-fold accelerations were also performed in 2:22 min, 1:53min, and 1:25 min respectively. In addition, ASL acquisition with no acceleration was performed in 4:25 min, serving as a benchmark for image quality. For CBF quantification, M0 images were acquired using CS-AI with 2-fold, 3-fold and 4-fold accelerations in 1:25 min, 0:56 min, and 0:47 min respectively, as well as with no acceleration in 2:12 min.CBF quantification was performed using the recommended approach [1], CBF maps were subsequently generated for each of the ASL/M0 acquisitions with CS-AI, and for the acquisitions with no acceleration. Circular ROIs were manually drawn on gray matter, and the mean CBF values within the ROIs were extracted. The ROIs covered a variety of brain regions, including upper frontal, upper parietal, lower operculum, lower occipital, thalamus, cerebellum, and brainstem. Linear regression and Bland-Altman analysis were used to compare the agreement of the ROI-based mean CBF values calculated from the ASL/M0 images acquired with 2-fold accelerated CS-AI, and with no acceleration.
Results
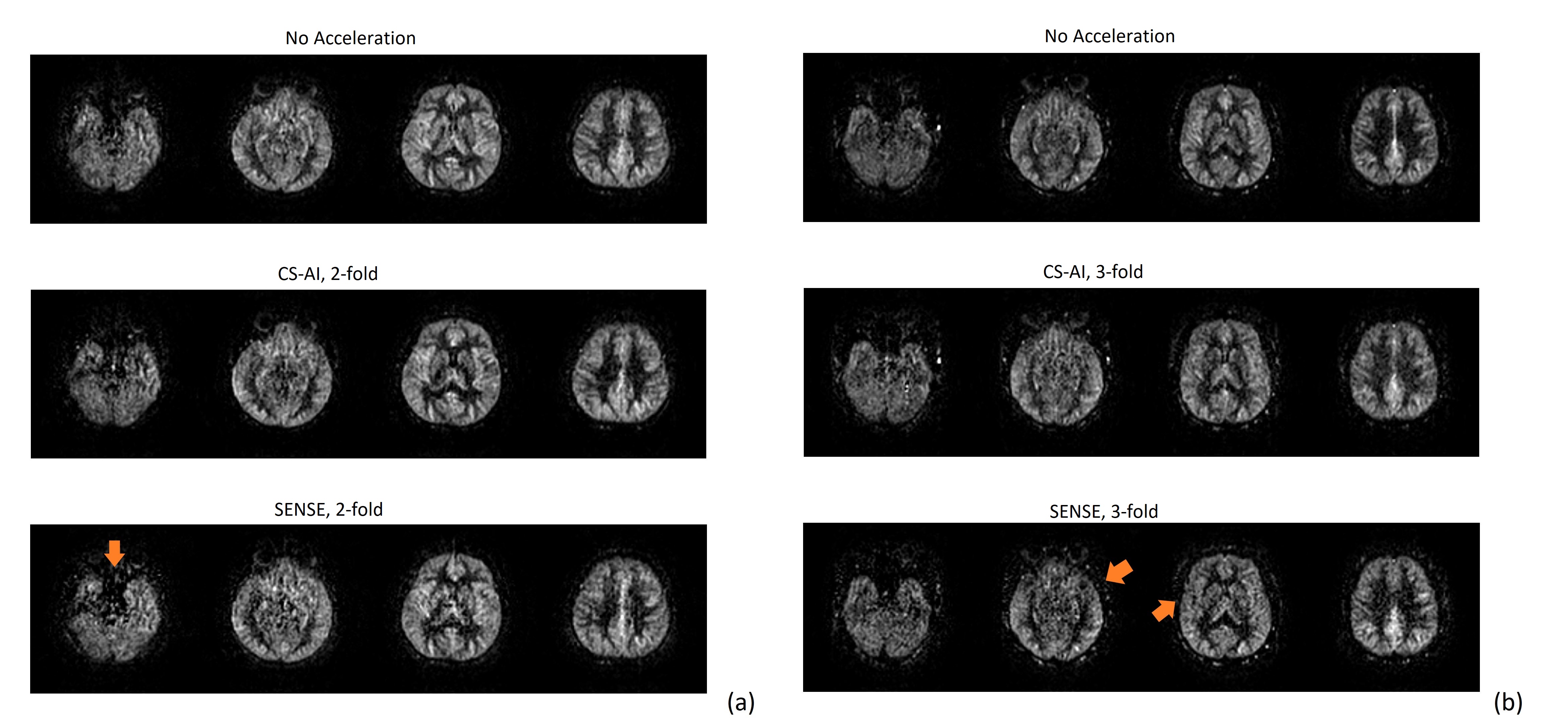
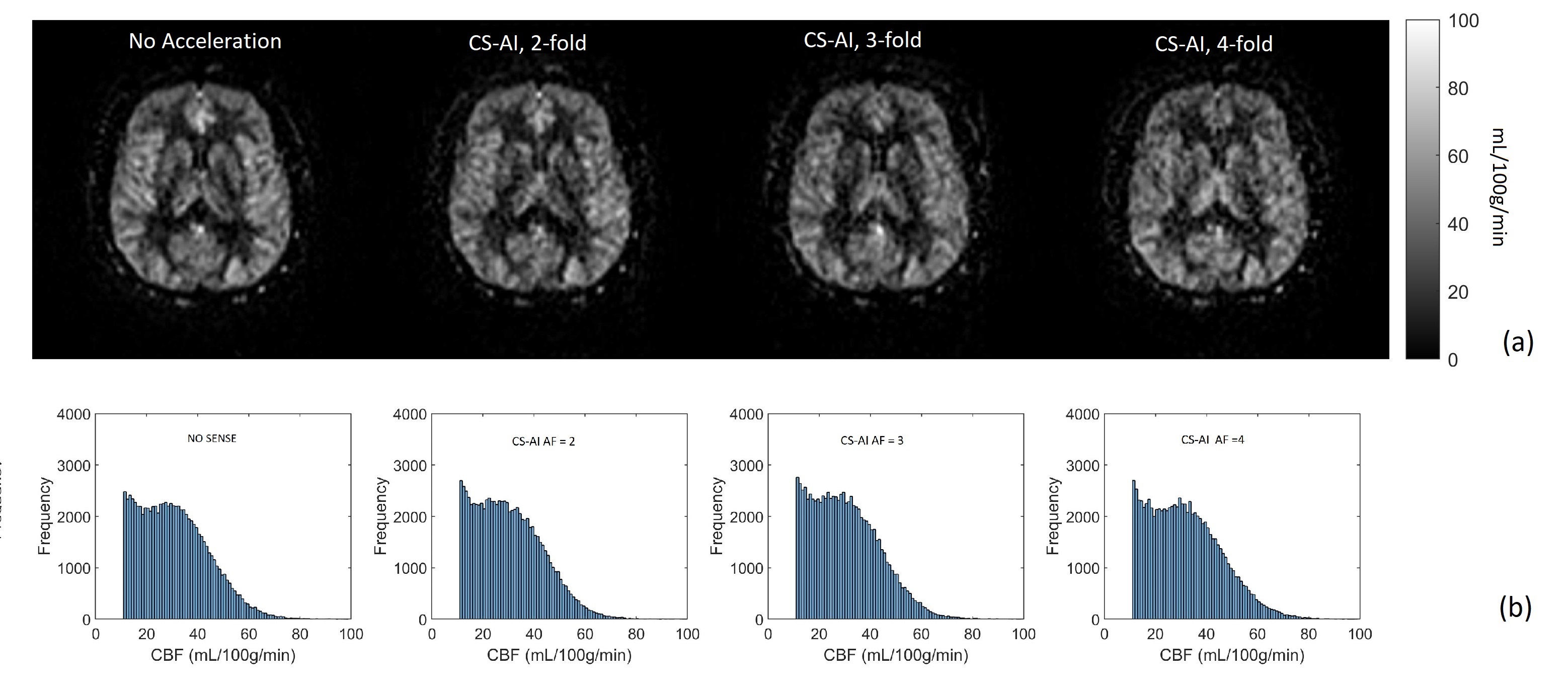
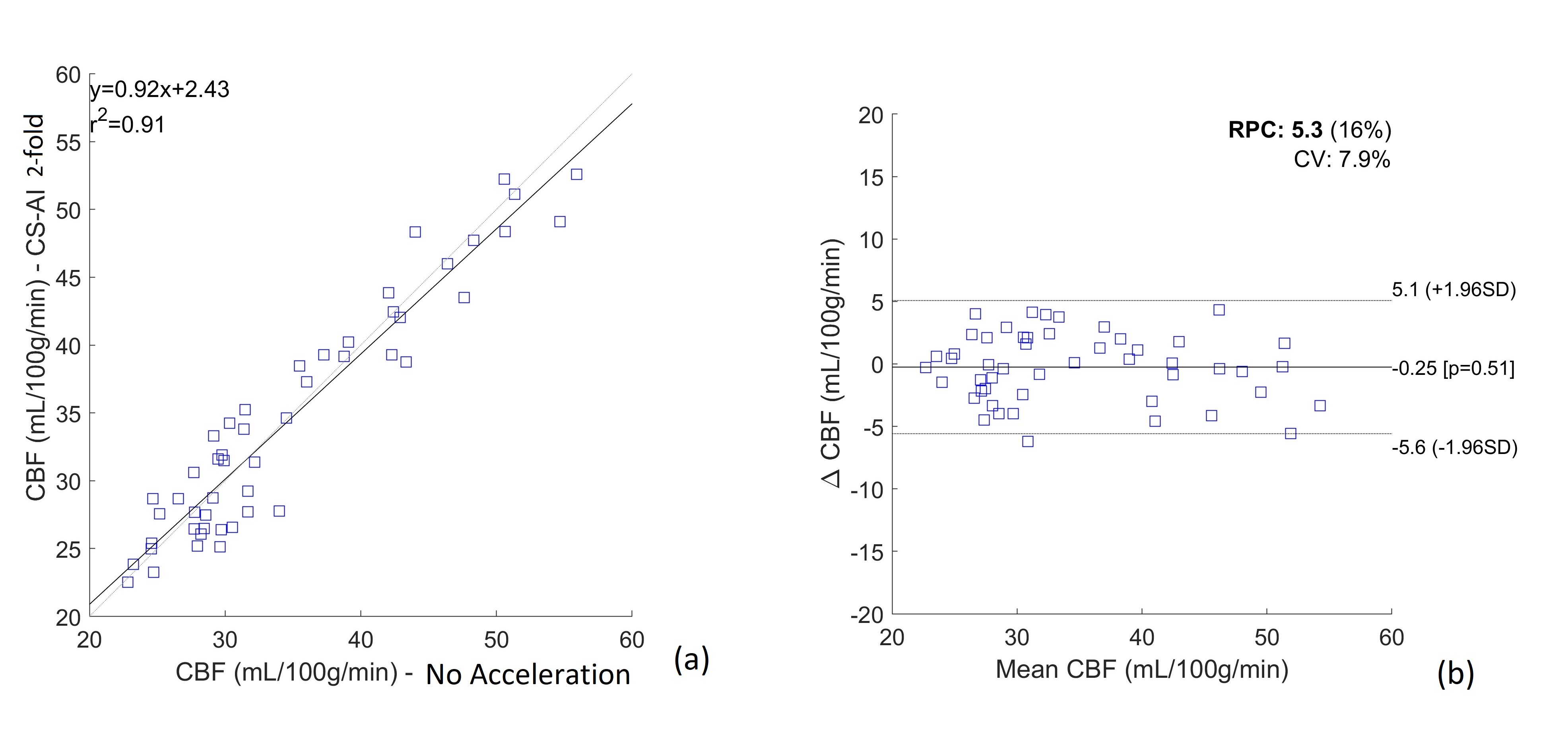
Brain perfusion weighted images acquired with improved spatial resolution (2.5x2.5x6 mm3) using CS-AI showed good SNR (fig.1). With 2-fold (fig. 1a) and 3-fold (fig. 1b) accelerations, the images acquired using CS-AI showed significantly higher SNR and better robustness to signal loss than the corresponding images acquired using SENSE with the same accelerations. CBF maps calculated from the ASL/M0 images acquired using CS-AI with 2-fold, 3-fold, and 4-fold accelerations are similar to the CBF map acquired with no acceleration (fig. 2a). In addition, the CBF distributions of CS-AI with different accelerations are consistent with the CBF map acquired with no acceleration (fig. 2b). This indicates the use of CS-AI with up to 4-fold acceleration does not introduce significant bias to the CBF quantification. The CBF values acquired using no acceleration and using CS-AI with 2-fold acceleration showed high correlation (R2 = 0.91, fig. 3a), as well as excellent agreement without significant bias (fig. 3b).Conclusion
We applied a compressed sensing artificial intelligence (CS-AI) framework to accelerate the brain ASL MR Imaging using 3D Cartesian TSE with higher spatial resolution (2.5x2.5x6 mm3). Perfusion weighted images acquired using CS-AI showed good SNR and image quality, and the SNR is significantly higher than the corresponding images acquired with SENSE. In addition, the use of CS-AI does not introduce bias to CBF quantification. CS-AI enables higher resolution 3D ASL MRI in the brain in a clinically feasible scan time (ASL/M0 acquisition in less than 4 min with 2-fold acceleration). This could be particularly useful to measure perfusion alterations in small-sized brain lesions, such as small metastatic and ischemic lesions.Acknowledgements
No acknowledgement found.References
[1] Alsop, DC et al. MRM 2015 Jan;73(1):102-16.
[2] Robson, PM et al. Acad Radiol 2016; 23(2):144-154.
[3] Taso, M et al. MRM 2019; 82(2):680-692.
[4] Greer, JS et al. MRM 2019; 82(5):1713-1724.
[5] Pezzotti, N et al. IEEE Access 2020 ; 8:204825–204838.
[6] Forman, SC et al. Euro Radiol 2022; 32:8376–8385.
Figures