2816
Respiratory-resolved 4D MRI: Further enhancements on the interplay of DL reconstruction and binning strategies1GE HealthCare, Munich, Germany, 2GE HealthCare, Houston, TX, United States, 3GE HealthCare, Madison, WI, United States, 4GE HealthCare, Little Chalfont, Amersham, United Kingdom, 5GE HealthCare, Boston, MA, United States, 6Massachusetts General Hospital, Boston, MA, United States
Synopsis
Keywords: Machine Learning/Artificial Intelligence, Image Reconstruction, Respiratory-resolved 4D MRI, Deep Learning reconstruction, radiation therapy planning
Motivation: To contribute to the clinical evidence generation for 4D MRI in radiation therapy planning.
Goal(s): Emphasize the impact of a DL reconstruction with amplitude and phase binning on respiratory motion characterization.
Approach: 4D MRI data of 10 healthy volunteers and 8 patients were acquired using a free-breathing T1-weighted stack-of-stars sequence at 1.5T or 3T.
Results: Independent of the binning strategy, DL reconstruction consistently improves image quality and conspicuity of small anatomical details with the potential to shorten scan times. Differences of binning strategies become prominent for irregular breathers, where amplitude binning reveals larger motion ranges than phase binning.
Impact: To foster the ultimate goal of clinical adoption of 4D MRI for radiotherapy planning, we present an enhanced 4D MRI application supporting multiple binning strategies and an embedded DL reconstruction.
Introduction
One of the main challenges for radiotherapy (RT) planning for thoracic and abdominal cancer treatment is to accurately account for respiratory motion to ensure a precise dose delivery to the tumor volume while sparing surrounding organs-at-risk (OARs).1 In clinical practice, abdominal compression and/or breath-holds are predominant strategies to minimize respiratory-induced movement already in the first place, while 4D CT is the state-of-the-art to estimate respiratory and hence tumor motion.2Recent advances in respiratory-resolved 4D MRI have demonstrated encouraging potential to overcome the current shortcomings of 4D CT.3 One key advantage of 4D MRI is its superior soft-tissue contrast facilitating more accurate delineation of tumor structures and OARs. Due to the continuous sampling over multiple breathing cycles, 4D MRI provides a desirable probabilistic representation of the respiratory motion compared to the snapshot-like 4D CT capturing a single respiratory cycle only. As such, 4D MRI can add value to conventional CT-based RT planning and plays an important role in establishing MR-only RT workflows.4
To contribute to the evidence generation required for clinical translation of 4D MRI for RT planning, the objective of this study is two-fold: 1) We demonstrate a versatile DL-based reconstruction (DLR) to improve image quality and/or shorten scan time. 2) We investigate the impact of different binning strategies on the depiction of respiratory motion with 4D MRI based on a 3D stack-of-stars readout. While other DL-based 4D MRI techniques have been demonstrated for a specific binning method, we show that the proposed DLR is agnostic to the binning strategy.
Methods
As part of an IRB-approved study, 10 healthy volunteers and 8 patients were prospectively recruited for an abdominal 1.5T or 3T MRI examination.For 4D MRI, raw k-space data are continuously acquired over multiple respiratory cycles using an FDA-approved free-breathing T1-weighted steady-state gradient echo product sequence with intermittent fat suppression and stack-of-stars spatial sampling. To temporally resolve the respiratory cycle, a motion surrogate signal is derived from the k-space center. The acquired data are retrospectively divided into ten respiratory-correlated phases by
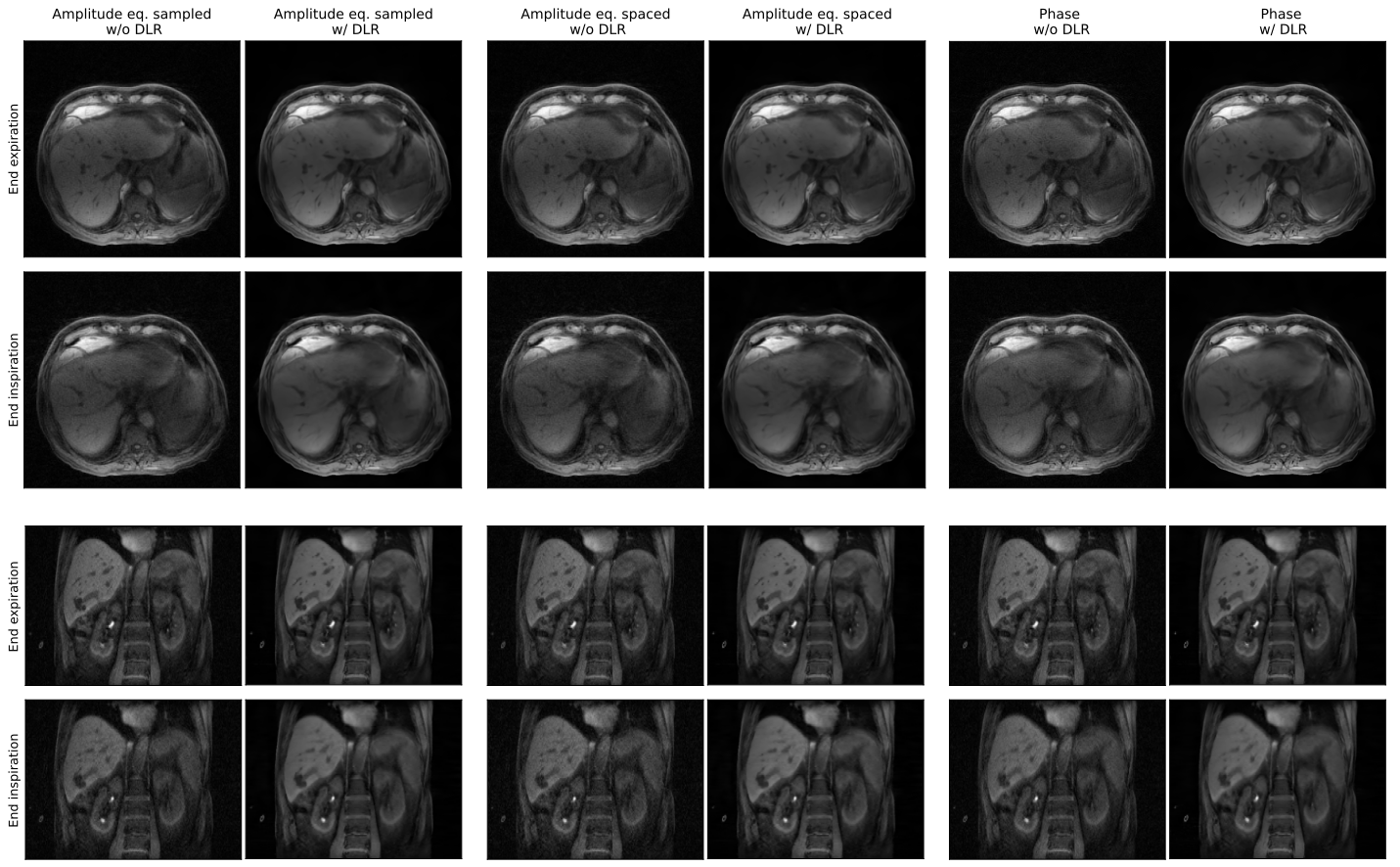
1) binning the amplitude of the motion signal such that all resulting motion states are equally sampled (Amplitude eq. sampled)
2) binning the amplitude of the motion signal into equidistant states (Amplitude eq. spaced)
3) binning each respiratory cycle into temporally equidistant states (Phase).
To increase SNR and spatial resolution and to reduce truncation and streak artifacts, a CNN-based model trained on a dataset of over 10,000 images was incorporated into the conventional reconstruction pipeline with Gaussian soft-gating.5 Volunteer and patient imaging was performed on 1.5T SIGNA™ Artist and 3T SIGNA™ Premier MRI scanners (GE HealthCare, Waukesha, WI) using the free-breathing LAVA Star sequence with 3D stack-of-stars encoding (FOV=420×420×300mm3, voxel size=1.6×1.6×2.5mm3, scan times=6:21/5:38min) and body array AIR™ coils (GE HealthCare, Chicago, IL). In addition, high resolution healthy volunteer data were acquired at 3T (voxel size=1.2×1.2×2.5mm3, scan time=8:36min).
Results and Discussion
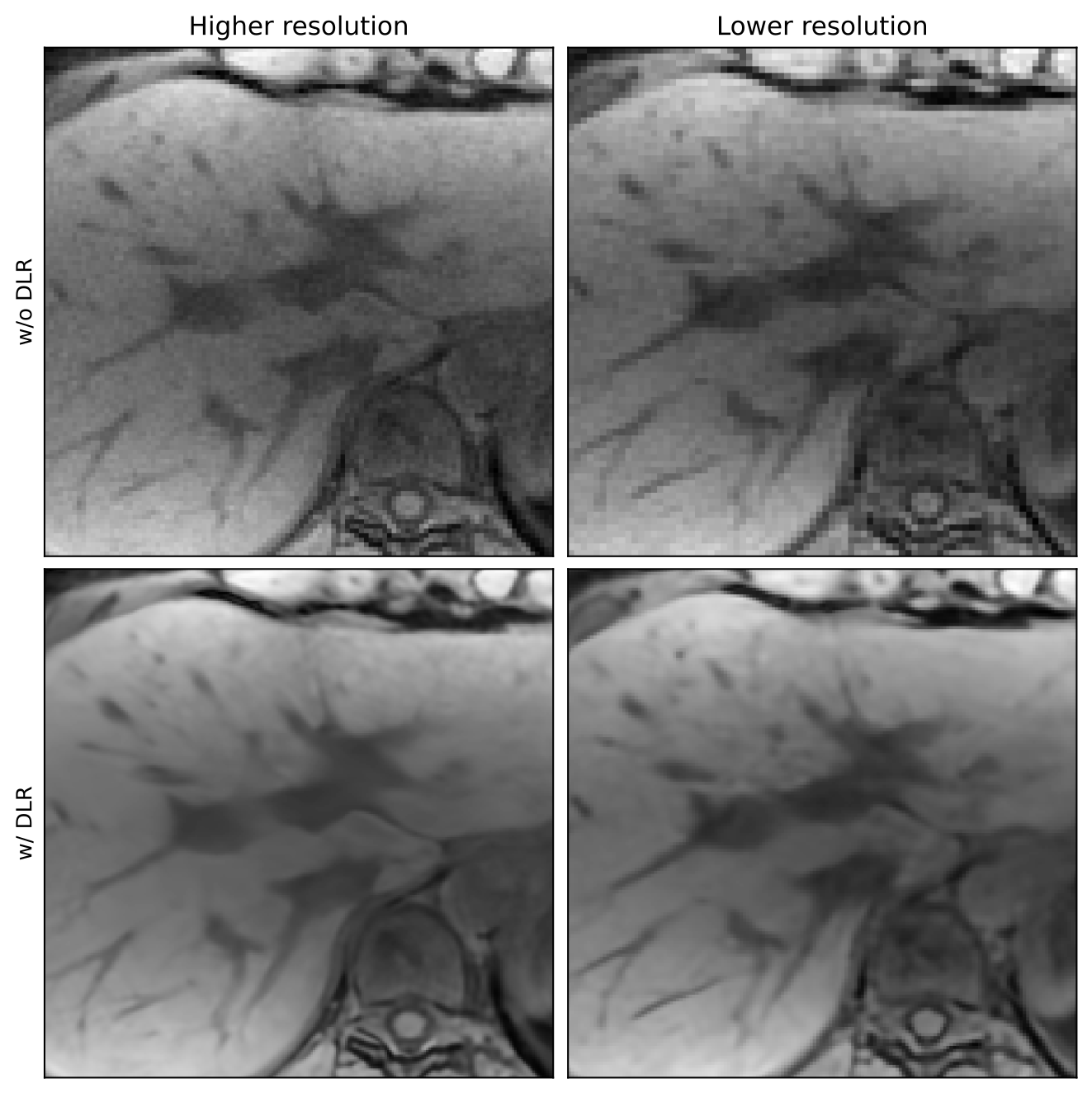
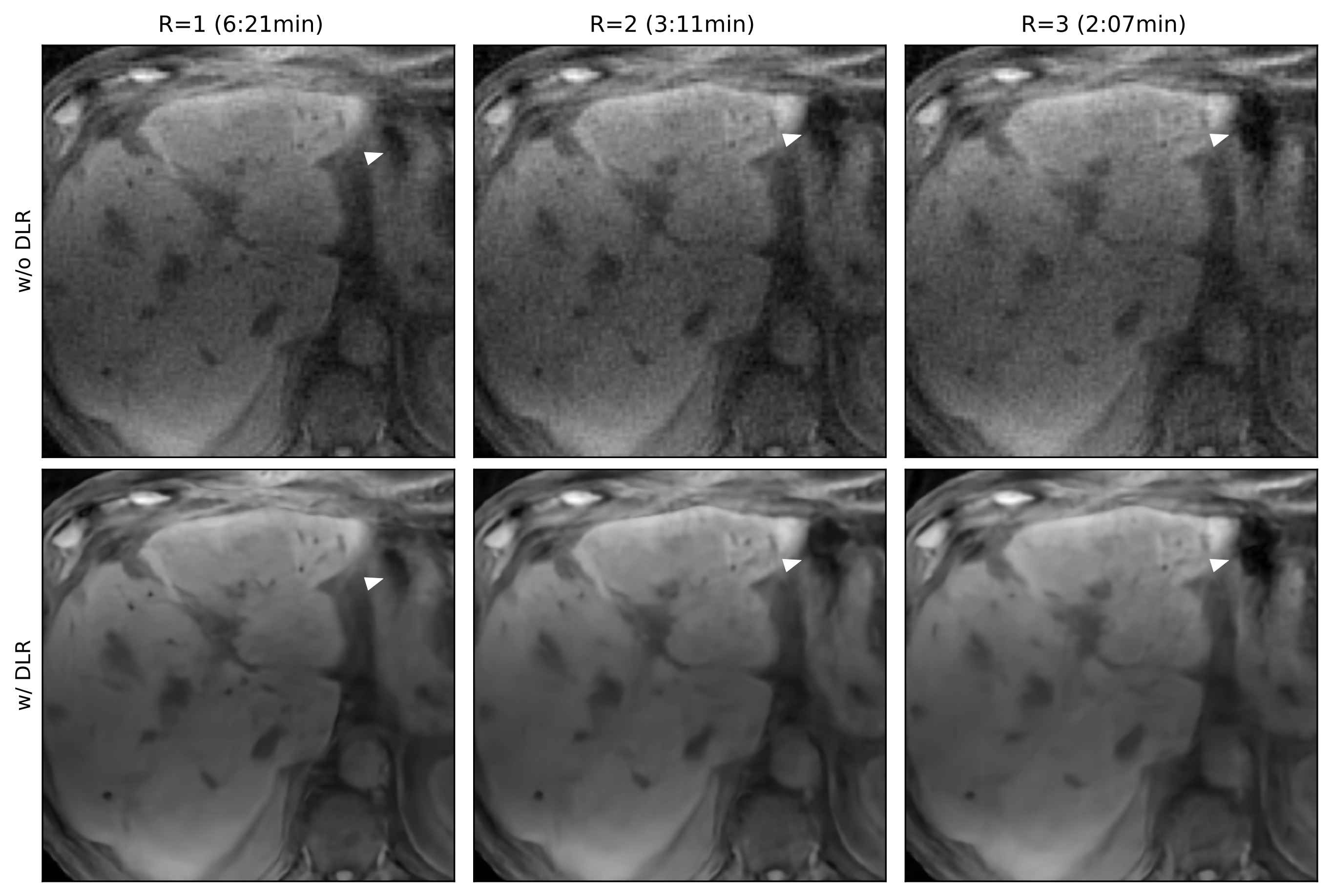
The proposed DL reconstruction consistently reduces noise, mitigates truncation and streaking artifacts, whilst preserving small anatomical structures (Figure 1). Generally, the image quality is enhanced independent of the underlying binning strategy, suggesting good generalizability of the DL reconstruction.As such, there are two main application scenarios for the DL reconstruction: As shown in Figure 2, it enhances overall image quality of 4D MRI independent of the native scan parameters, such as resolution. The capabilities of the DL reconstruction could also enable shortening 4D MRI scanning by acquiring fewer radial spokes (Figure 3).
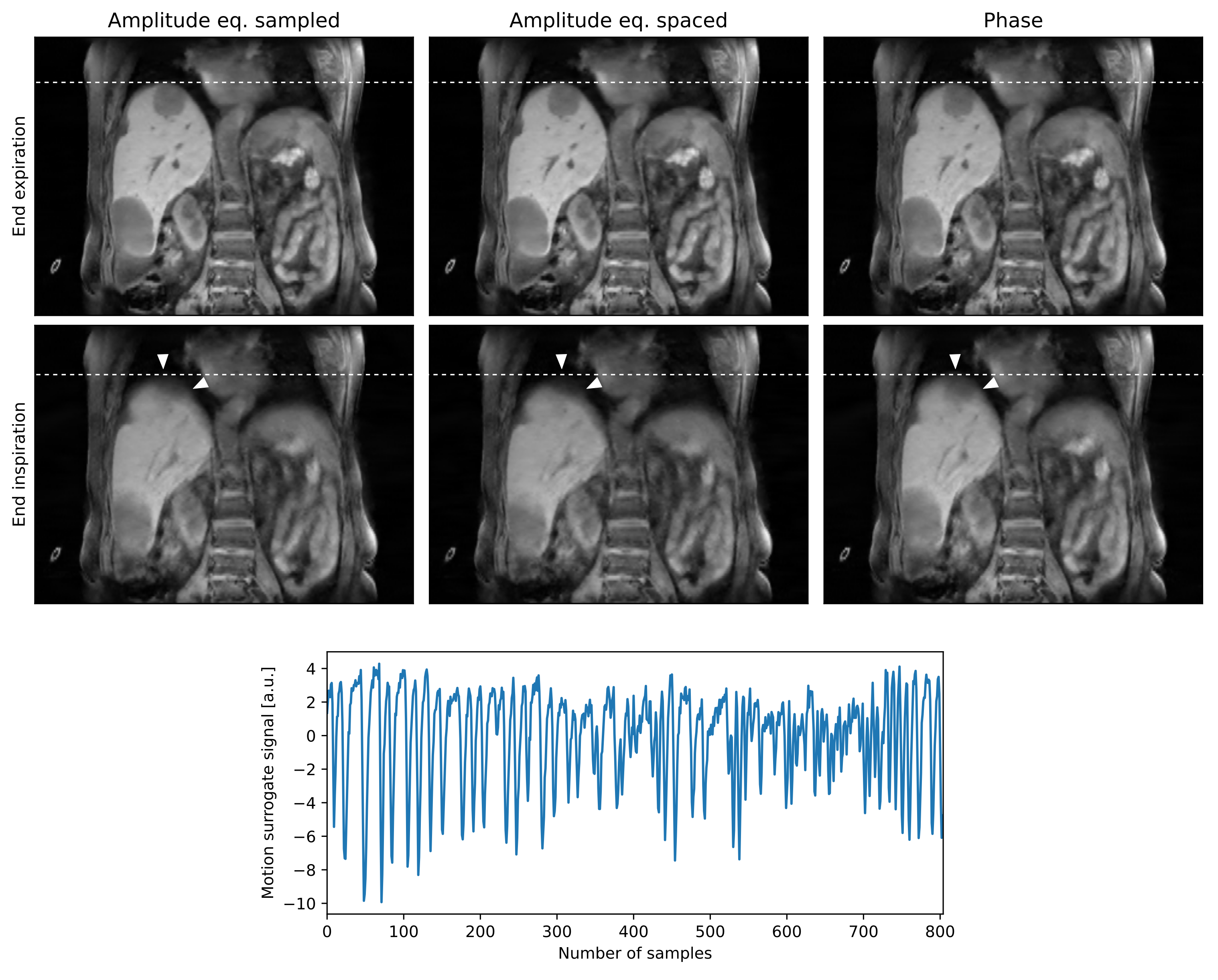
Regarding 4D MRI-based motion characterization, it is seen from Figure 4 that all binning strategies consistently reveal the end expiration phase. For irregular breathers, both amplitude binning techniques reveal a larger respiratory motion range than phase binning. Amplitude binning tends to be more prone to motion-induced blurring, e.g., at the lung liver interface. Phase binning produces more consistent image quality throughout the phases, while for both amplitude binning techniques image quality improves towards the end expiration phase. Equally sampled amplitude binning can improve image quality compared to equally spaced amplitude binning for irregular breathing patterns and hence unevenly populated phases.
Conclusion
In this 4D MRI study, we demonstrate the impact of amplitude and phase binning strategies on motion characterization in abdominal cancer patients and present a versatile DL reconstruction that is agnostic to the respective type of motion binning and magnetic field strength, effectively enhancing overall image quality of the derived motion phases. To further promote the clinical adoption of 4D MRI for RT planning workflows, next steps will focus on 1) DL-based image translation for 4D pseudo-CT generation which is key for MR-only RT planning and 2) DL-based OAR segmentation.Acknowledgements
We would like to acknowledge the MGH Radiation Oncology staff and clinical research coordinators who helped with acquiring the MRI data. This work has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No. 952172.References
- Keall PJ, Mageras GS, Balter JM, et al. The management of respiratory motion in radiation oncology report of AAPM Task Group 76a). Med. Phys. 2006;33(10):3874–3900.
- Ball HJ, Santanam L, Senan S, et al. Results from the AAPM Task Group 324 respiratory motion management in radiation oncology survey. J. Appl. Clin. Med. Phys. 2022;23(11):e13810.
- Tryggestad E, Li H, Rong Y. 4DCT is long overdue for improvement. J. Appl. Clin. Med. Phys. 2023;24(4):e13933.
- Otazo R, Lambin P, Pignol J-P, et al. MRI-guided Radiation Therapy: An Emerging Paradigm in Adaptive Radiation Oncology. Radiology. 2021;298(2):248–260.
- Wang X, Lee Y, Lee J, et al. Convolutional Neural Network based Stack-of-Star Imaging with Noise and Artifacts Removal. In: Proc. Intl. Soc. Mag. Reson. Med. 31. Toronto, Canada; 2023.
Figures