2814
A Comprehensive Quality Assessment on AI-assisted Fast MRI Acquisition for China Baby Connectome Project (CBCP)1School of Biomedical Engineering, ShanghaiTech University, Shanghai, China, 2Department of Radiology, Xiamen Children's Hospital, Children's Hospital of Fudan University at Xiamen, Xiamen, China, 3Shanghai United Imaging Healthcare Co., Ltd., Shanghai, China, 4Shanghai United Imaging Intelligence Co., Ltd., Shanghai, China, 5Shanghai Clinical Research and Trial Center, Shanghai, China
Synopsis
Keywords: Machine Learning/Artificial Intelligence, Data Acquisition, MRI Acceleration, Fast Acquisition, New MRI Techniques
Motivation: Acquiring a high-quality 3D brain MRI in a short time is highly desired for infants/children studies.
Goal(s): To optimize and systemically evaluate an innovative technology, AI-assisted Compressed Sensing (ACS), used in Chinese Baby Connectome Project (CBCP) with faster 3D-T1w scans and preserved imaging fidelity.
Approach: We compared ACS with conventional techniques along the entire processing pipeline. CBCP-ACS was also compared with the existing infant cohort (BCP) with P2 acceleration regarding the derived development trajectories.
Results: Results suggested that CBCP data, with halved acquisition time, had comparable quality and derived neuroscience findings to BCP, indicating that a large cohort study with ACS is mature.
Impact: Equip high-resolution 3D-T1w MRI acquisition with ACS effectively shortens the acquisition time by 44%, providing a stable and robust solution for building large-scale infant/children brain imaging cohorts. The established technique could also facilitate clinical scans and patient studies.
Introduction
Early brain development research heavily relies on good MRI quality to gain insights into the structural and functional aspects of infant brains. However, infants and young children are particularly prone to head motion during MRI, leading to motion-induced artifacts or failed scans1. Prolonged scanning time for high-resolution imaging further exacerbates this issue by reducing subject compliance. Previously, limited MRI modalities have to be used in building large infant cohorts due to long acquisition time. To address these challenges, we specifically investigate the potential of a new fast MRI acquisition method, AI-assisted Compressed Sensing (ACS)2, for ongoing China’s largest infant cohort construction.ACS combines deep convolutional neural networks with various traditional acceleration strategies to improve imaging speed and accuracy2. While ACS has been applied successfully in certain clinical scenarios with 2D scans3,4, its application in 3D brain imaging, especially for infants, remains unexplored. Our research aims to fill this gap by assessing ACS's potential to reduce scan time with better preserved image fidelity and its feasibility for future widespread use in building infant brain big data, ultimately benefiting early brain development studies and identifying neurological disorders in many more vulnerable populations.
Methods
Two datasets, an adult pilot study with 24 healthy adults (aged 19–24) and the China Baby Connectome Project (CBCP) with 73 infants/children (aged 0-5) so far, were collected. The adult scans included 3D-T1w FSP images (0.8mm isotropic voxel) with two protocols: paralleled imaging with acceleration factor 2 (P2) in 6min39s and ACS in 3min46s. All other imaging parameters are the same. For CBCP datasets, only ACS was used. All data were acquired with a 64-channel head coil from a United Imaging 3.0T uMR890 scanner.Adult Pilot Study QC: 1) Visual inspection by two radiologists rating 24 image pairs, assessing SNR, artifacts, clarity of gray-white matter boundary, and overall quality on 5-level Likert scales5. Wilcoxon signed-rank tests were used to compare their rates between P2 and ACS6. 2) Quantitative QC was carried out on preprocessed images (N4 correction, FreeSurfer recon-all7) with various evaluation metrics (CNR, SNR, FWHM) computed with MRIQC8, with Qoala-T supplied additional QC scores9. Paired t-tests compared these metrics between P2 and ACS. 3) Vertex-wise and region-wise cortical surface geometric indices were compared between P2 and ACS. The resultant image fidelity was assessed by calculating intra-class correlation (ICC) between P2 and ACS.
Infant Study: using an in-house infant brain MRI processing pipeline, we calculated whole brain volume from 73 CBCP infants and 73 age/sex-matched BCP infants10. After applying ordinary least squares (OLS) regression to both datasets for whole brain volume development, we performed a permutation test to compare their developmental trajectories.
Results
Fig. 1 shows highly comparable image quality between P2 and ACS. Tab. 1 summarizes visual inspection rates from two radiologists for P2 and ACS. No differences were spotted between P2 and ACS, meaning they were highly comparable.Fig. 2 shows that ACS outperforms P2 with improved SNR, CNR, and Qoala-T scores. ACS produced less sharp images (higher FWHM) than P2.
Surface-based geometric measures show little-to-no difference in cortical thickness, area, curvature, and sulcal depth between P2 and ACS (Fig. 3 top). Region-wise ICC values indicate excellent agreement (53.3% of ICC values exceeded 0.9), with the cortical area having the highest mean ICC score (0.94) (Fig. 3 bottom).
Fig. 4 plots the developmental trajectories of whole brain volume for CBCP infants (with ACS scans) and matched BCP infants (with P2 scans)10. The permutation test shows no significant difference between the two curves (p=0.39).
Discussion
ACS improves imaging CNR and SNR by applying image fidelity-keeping constraints using deep learning with other acceleration techniques. While higher ACS accelerating rates generate more blurred images, with a proper accelerating rate (ACS3.32), one can obtain balanced acquisition time and imaging accuracy. Of note, a higher ACS accelerating rate, ACS12 (it acquires a 0.8mm isotropic T1w MRI in only 1min3s) is recommended to alleviate motion artifacts for fidgety infants. Nevertheless, we have observed that ACS has a higher tolerance to head motion than P2. Crucially, ACS maintains image details, as supported by consensus among raters and rigorous statistical analysis of neuroscience measures and neurodevelopmental outcomes.Conclusion
This study established the effectiveness of a new fast MRI acquisition technique (ACS) in 3D high-resolution brain structural MRI. Compared to conventional techniques such as P2, ACS reduces almost 50% of the scanning time in T1w MRI with excellent image fidelity. Saved time for other vital modalities, especially needed in creating large cohorts for vulnerable populations. ACS has been used in building China’s largest infant cohort (CBCP).Acknowledgements
This work is partially supported by the STI 2030—Major Project (2022ZD0209000, 2021ZD0200516), Shanghai Pilot Program for Basic Research—Chinese Academy of Science, Shanghai Branch (JCYJ-SHFY-2022-014), Open Research Fund Program of National Innovation Center for Advanced Medical Devices (NMED2021ZD-01-001), Shenzhen Science and Technology Program (No. KCXFZ20211020163408012), and Shanghai Pujiang Program (No. 21PJ1421400).
References
1. Thieba C, Frayne A, Walton M, et al. Factors Associated With Successful MRI Scanning in Unsedated Young Children. Front Pediatr. 2018;6. doi:10.3389/fped.2018.00146
2. Sheng R fan, Zheng L yun, Jin K pu, et al. Single-breath-hold T2WI liver MRI with deep learning-based reconstruction: A clinical feasibility study in comparison to conventional multi-breath-hold T2WI liver MRI. Magn Reson Imaging. 2021;81:75-81. doi:10.1016/J.MRI.2021.06.014
3. Yan X, Ran L, Zou L, et al. Dark blood T2-weighted imaging of the human heart with AI-assisted compressed sensing: a patient cohort study. Quant Imaging Med Surg. 2023;13(3):1699-1710. doi:10.21037/qims-22-607
4. Liu K, Xi B, Sun H, et al. The clinical feasibility of artificial intelligence-assisted compressed sensing single-shot fluid-attenuated inversion recovery (ACS-SS-FLAIR) for evaluation of uncooperative patients with brain diseases: comparison with the conventional T2-FLAIR with parallel imaging. Acta radiol. 2023;64(5):1943-1949. doi:10.1177/02841851221139125
5. Sullivan GM, Artino AR. Analyzing and Interpreting Data From Likert-Type Scales. J Grad Med Educ. 2013;5(4):541-542. doi:10.4300/JGME-5-4-18
6. Wilcoxon F. Individual Comparisons by Ranking Methods. Biometrics Bulletin. 1945;1(6):80. doi:10.2307/3001968
7. Fischl B. FreeSurfer. Neuroimage. 2012;62(2):774-781. doi:10.1016/j.neuroimage.2012.01.021
8. Esteban O, Birman D, Schaer M, Koyejo OO, Poldrack RA, Gorgolewski KJ. MRIQC: Advancing the automatic prediction of image quality in MRI from unseen sites. PLoS One. 2017;12(9):e0184661. doi:10.1371/journal.pone.0184661
9. Klapwijk ET, van de Kamp F, van der Meulen M, Peters S, Wierenga LM. Qoala-T: A supervised-learning tool for quality control of FreeSurfer segmented MRI data. Neuroimage. 2019;189:116-129. doi:10.1016/j.neuroimage.2019.01.014
10. Howell BR, Styner MA, Gao W, et al. The UNC/UMN Baby Connectome Project (BCP): An overview of the study design and protocol development. Neuroimage. 2019;185:891-905. doi:10.1016/j.neuroimage.2018.03.049
Figures
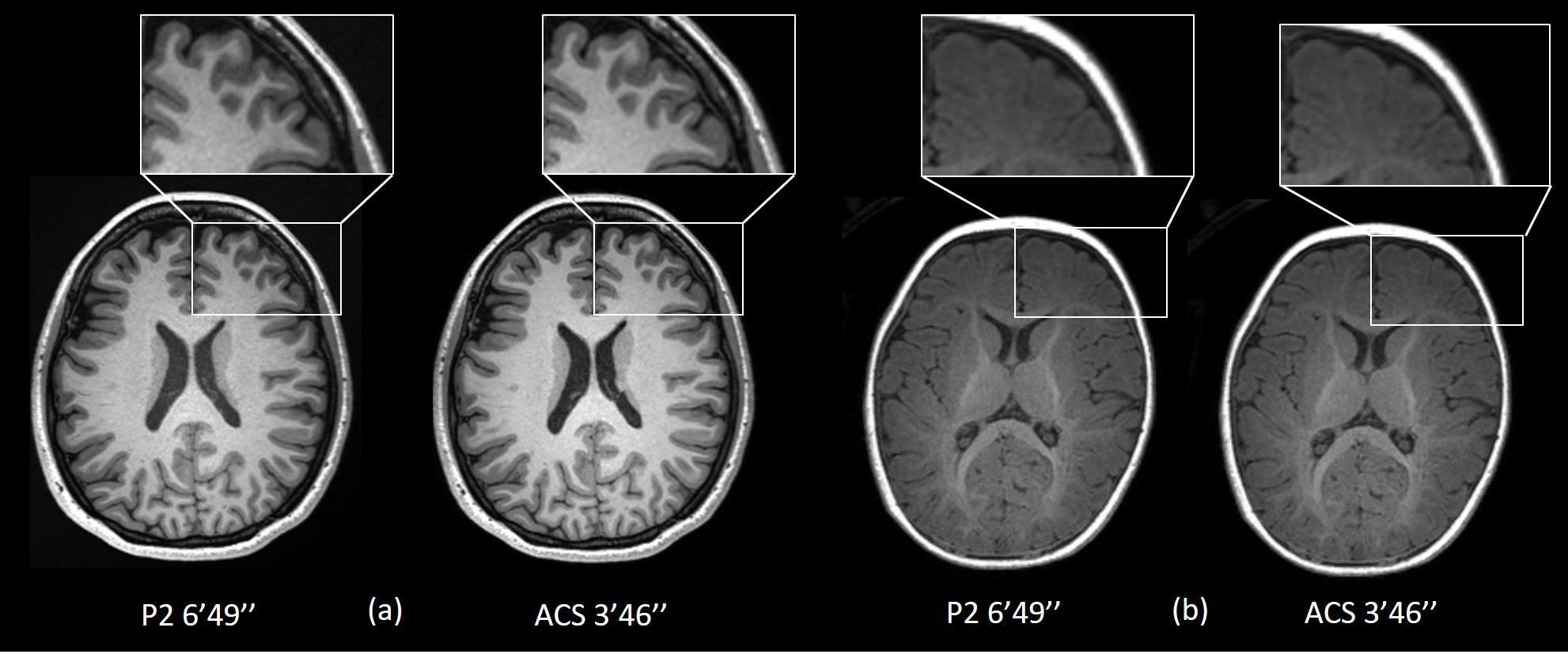
Fig. 1 3D high-resolution (0.8 mm isotropic) T1w MRI acquired with both P2 and ACS for an adult (a) and an infant of 9 months old (b).
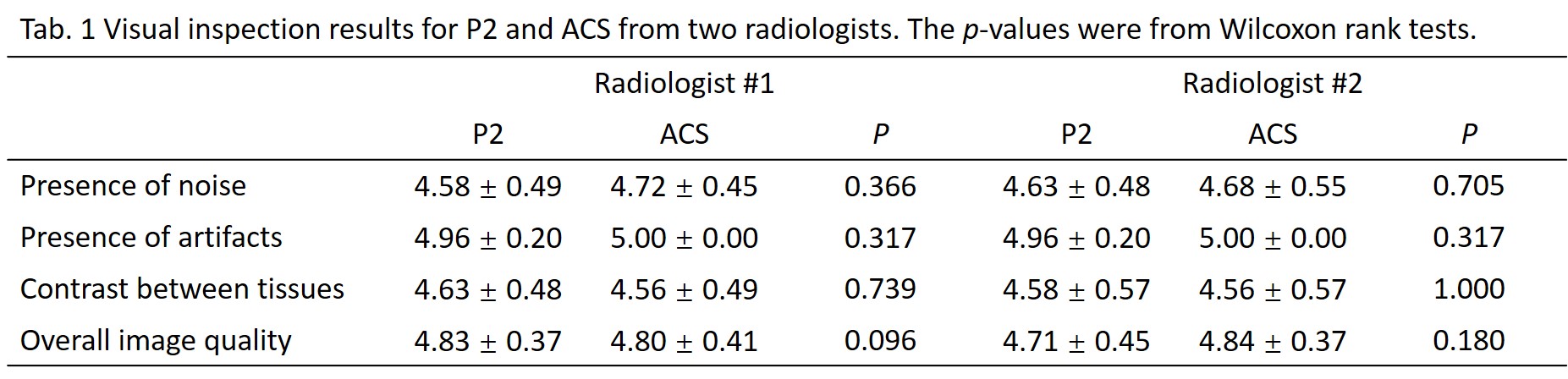
The p-values were derived from Wilcoxon rank tests comparing scores from two radiologists. A p value larger than 0.05 indicate there was no significant difference between two radiologists’ rating results.
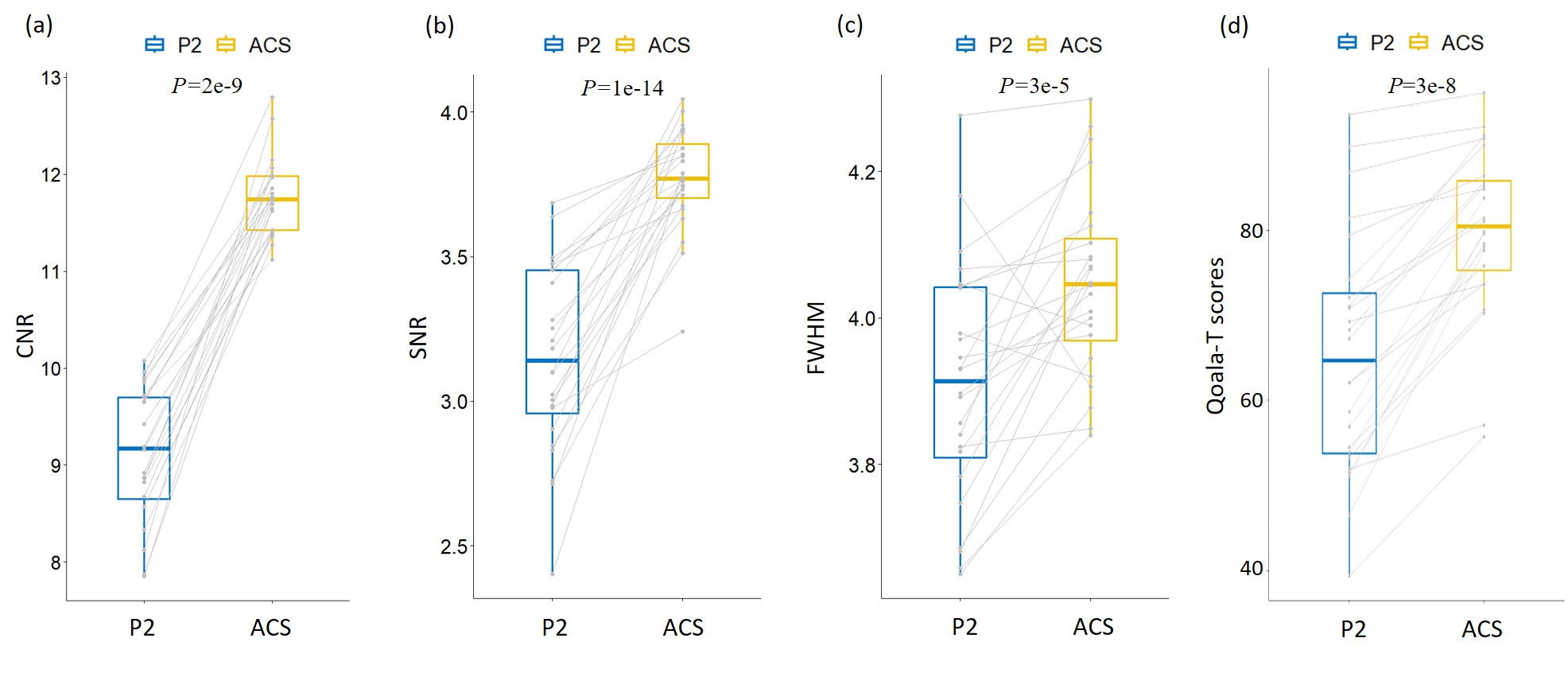
Fig. 2 Comparison of quantitative QC measures between P2 and ACS, including (a) SNR, (b) CNR, (c) FWHM, and (d) Qoala-T scores.
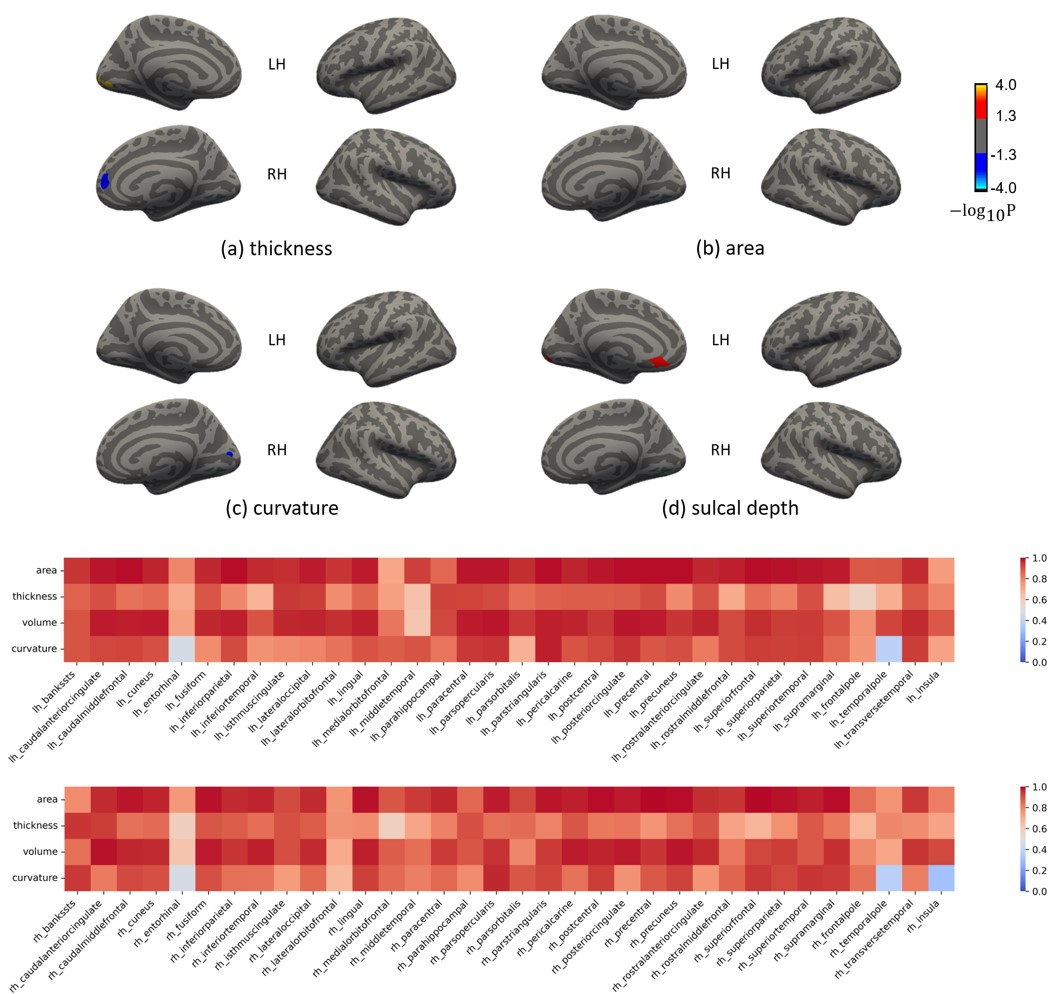
Fig. 3 Top: surface-based vertex-wise comparisons on four geometric features (a, thickness, b, area, c, curvature, and d, sulcal depth) between PP2 and ACS. Warm color indicates significantly higher (vertex-wise p<0.001, cluster-wise p<0.05) values from PP2 compared to ACS, and vice versa. Bottom: ICC values (agreement) of surface-based region-wise measures in both left and right hemispheres.
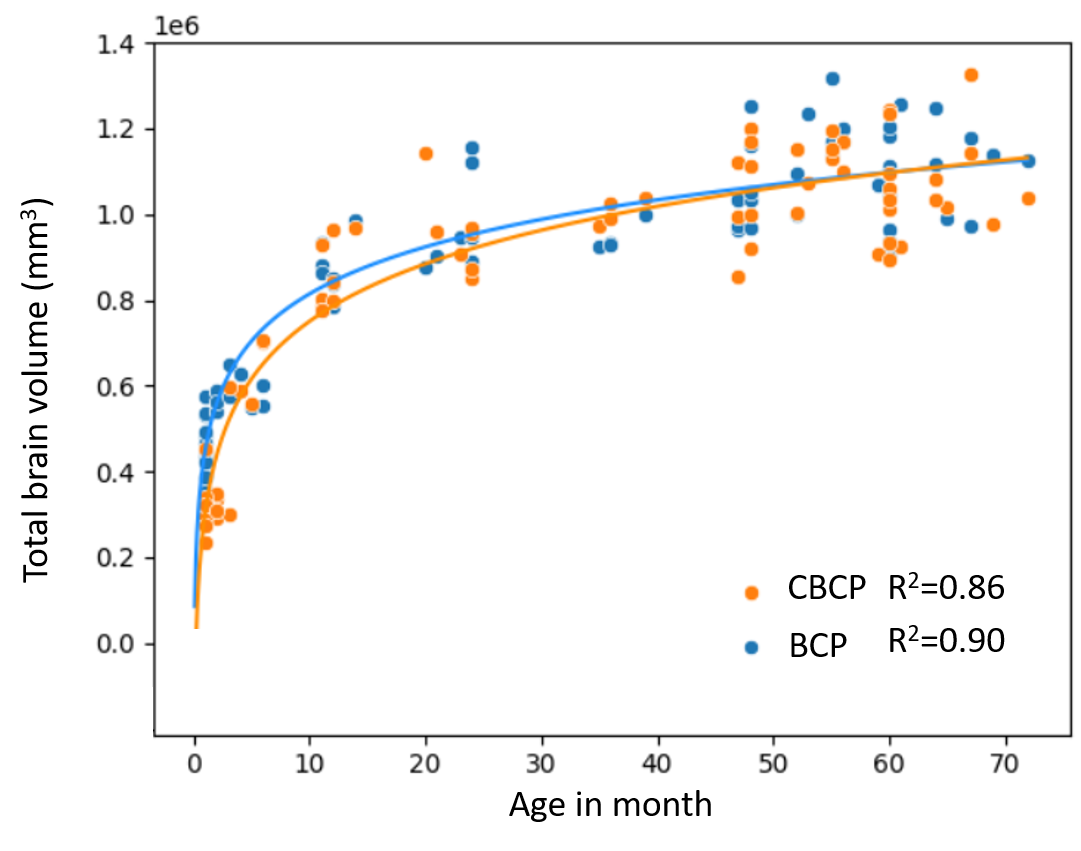
Fig. 4 The developmental trajectories of total brain volume for CBCP infants (with ACS scans) and matched BCP infants (with P2 scans).