2804
Deep Learning-based Reconstruction of Accelerated MR Cholangiopancreatography1Artificial Intelligence in Biomedical Engineering, Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany, 2MR Application Pre-development, Siemens Healthineers AG, Erlangen, Germany
Synopsis
Keywords: Machine Learning/Artificial Intelligence, Image Reconstruction
Motivation: We address the issue of long scan times in MR Cholangiopancreatography (MRCP), which often leads to poor image quality.
Goal(s): We aim to leverage a Deep Learning-based model to accelerate MRCP acquisition.
Approach: We acquired two-times parallel imaging accelerated MRCP data at 3T, trained a variational network with retrospective undersampling to a total acceleration factor of 6, and then tested the trained model with both retrospective and prospective 6-times accelerated data, acquired at both 3T and 0.55T.
Results: The trained model shows potential to improve MRCP by reducing artifacts and enhancing distal ducts compared to parallel imaging and compressed sensing.
Impact: The proposed method effectively removes artifacts in highly accelerated MRCP, shortening scan times from 303 seconds to 138 seconds. Moreover, the corresponding SNR enhancement enables MRCP acquisitions at 0.55T, where traditional image reconstruction methods face challenges.
Motivation
MR Cholangiopancreatography (MRCP) is essential for detailed anatomical imaging of the hepatobiliary ducts. However, the prolonged scan times of 3D T2-weighted sequences make MRCP prone to artifacts caused by breathing motion, which can compromise diagnostic quality. We propose to use Deep Learning (DL)-based reconstruction[1] to reduce the scan time in MRCP. We evaluate our proposed method by performing qualitative and quantitative comparisons to conjugate-gradient SENSE[2] (CG-SENSE) and L1-wavelet-based compressed sensing[3] (CS). These assessments encompass prospective and retrospective undersampling scenarios using MRCP data acquired on 3T and 0.55T.Methods
DataWe acquired MRCP data from 15 healthy volunteers using a 3D T2-weighted turbo spin-echo sequence[4]. Among these, 14 volunteers underwent scanning on a clinical 3T MR scanner, while 1 volunteer was scanned at 0.55T (3T: MAGNETOM Vida and Lumina and 0.55T: MAGNETOM Free.Max, Siemens Healthineers AG, Erlangen, Germany). We performed multiple scans of volunteers on 3T scanners for the purpose of data augmentation. We used the clinical routine protocol, including PACE navigator triggering[5] with a parallel imaging acceleration factor of two and 24 autocalibration signals at the center of k-space to estimate receiving coil sensitivities. The data were acquired in 97 breathing cycles requiring 303 seconds. Prospectively 6-times accelerated data, which necessitated only 39 breathing cycles in 138 seconds, was acquired in 2 healthy volunteers at each 3T and 0.55T, respectively. An inverse Fourier transform was applied along the fully-sampled slice direction, and 2D slices were reconstructed independently. We used the ESPIRiT[6] implementation from Sigpy[7] to estimate coil sensitivity maps.
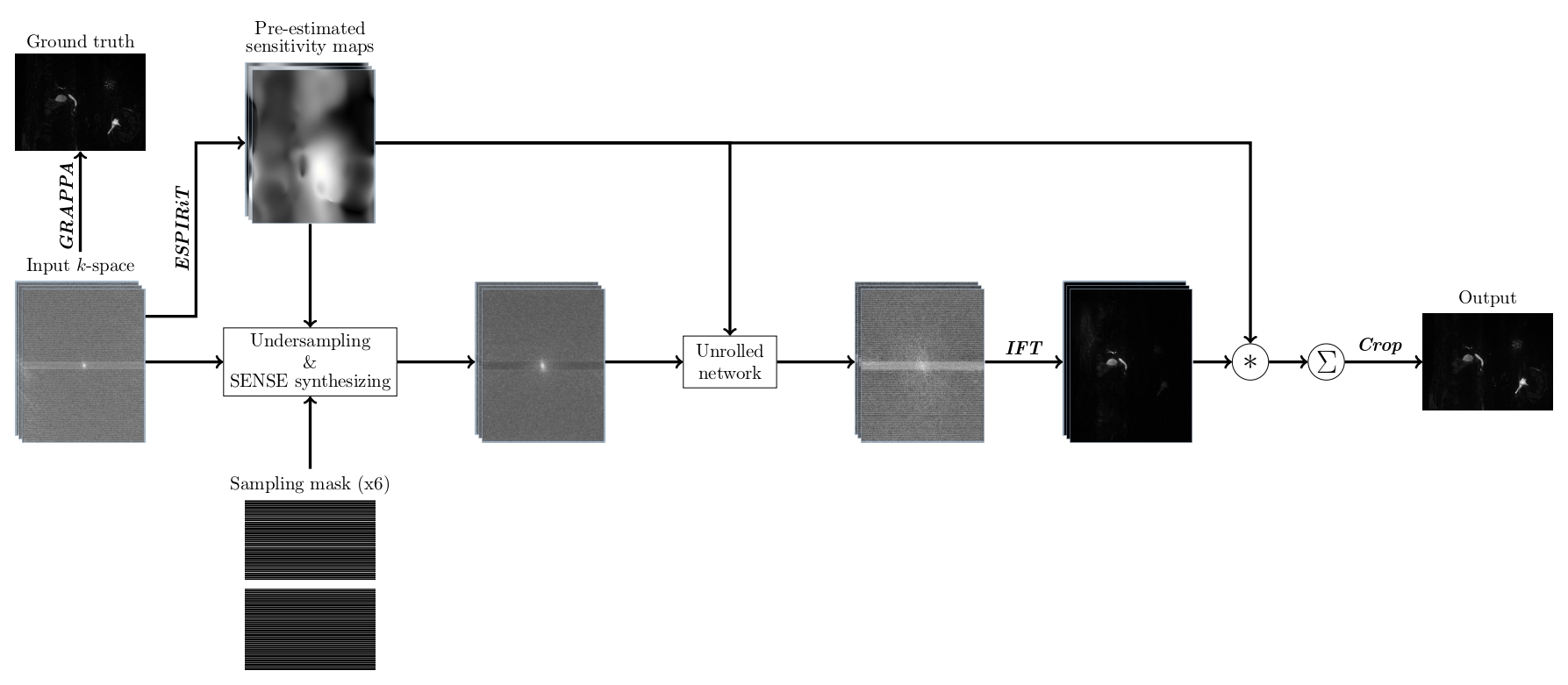
DL-based reconstruction model
We used a modified version of the variational network[1] (VN) with 12 cascades and approximately 103M trainable parameters. Instead of using zero-filled k-space as the input to the VN, we performed an initial SENSE reconstruction and then synthesized the missing k-space coefficients in the accelerated acquisitions from the SENSE reconstruction. To obtain a ground truth for our supervised VN training, we performed a GRAPPA reconstruction[8] of our two-times accelerated data. We utilized 32 datasets from 12 volunteers for training and 1 dataset from 1 volunteer for validation, all of which were obtained at 3T and retrospectively undersampled to a factor of 6. For independent testing, we included two more datasets, each obtained at both 3T and 0.55T. Figure 1 shows an illustration of our training pipeline.
Evaluation
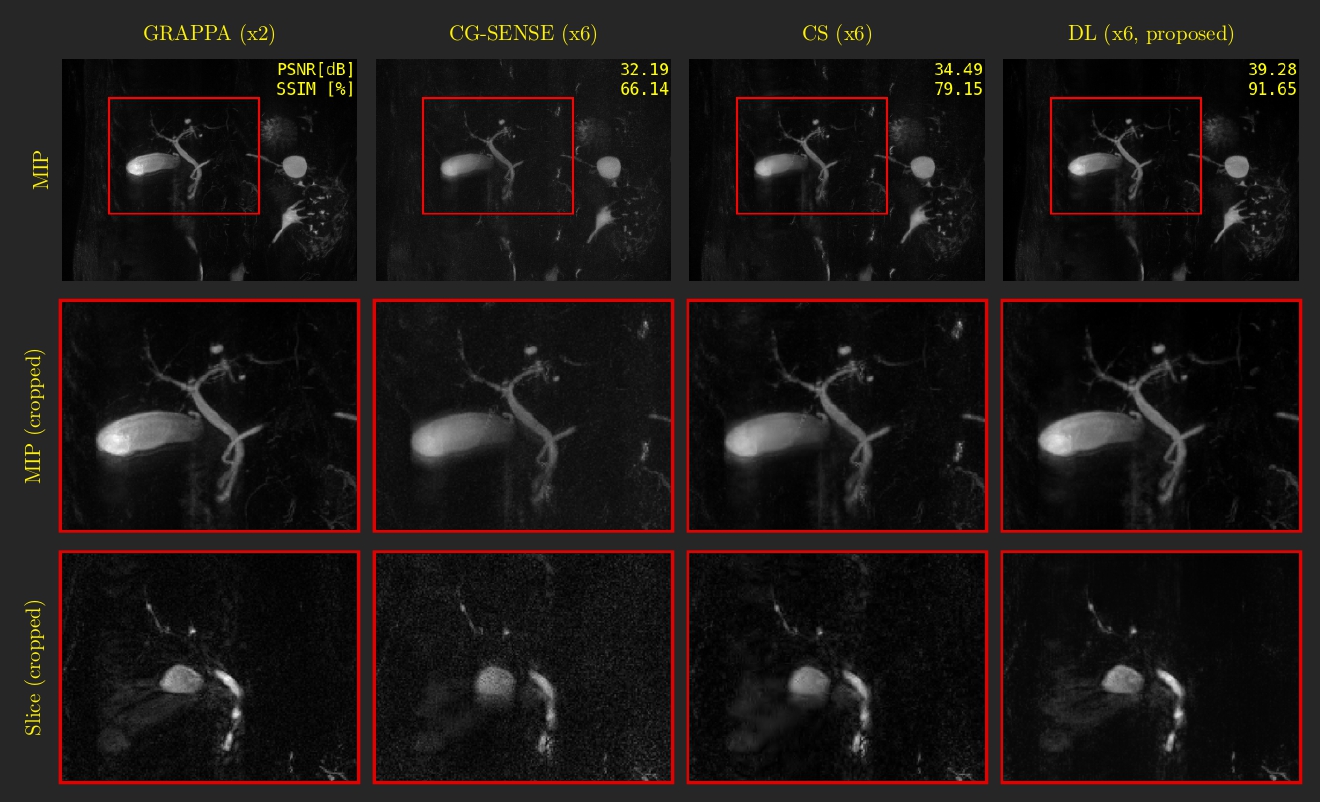
The performance of the proposed method at 6-times acceleration was compared to CG-SENSE and CS reconstructions using the implementation from Sigpy. The same coil sensitivity maps were used in all reconstructions. In our retrospective analysis, we computed structural similarity (SSIM) and peak signal-to-noise ratio (PSNR) to the GRAPPA-reconstructed ground truth in 3D volume. Due to the lack of a ground truth for reference, we only performed qualitative comparisons of the prospective acquisitions to the corresponding two-times accelerated acquisitions from the same volunteer.
Results
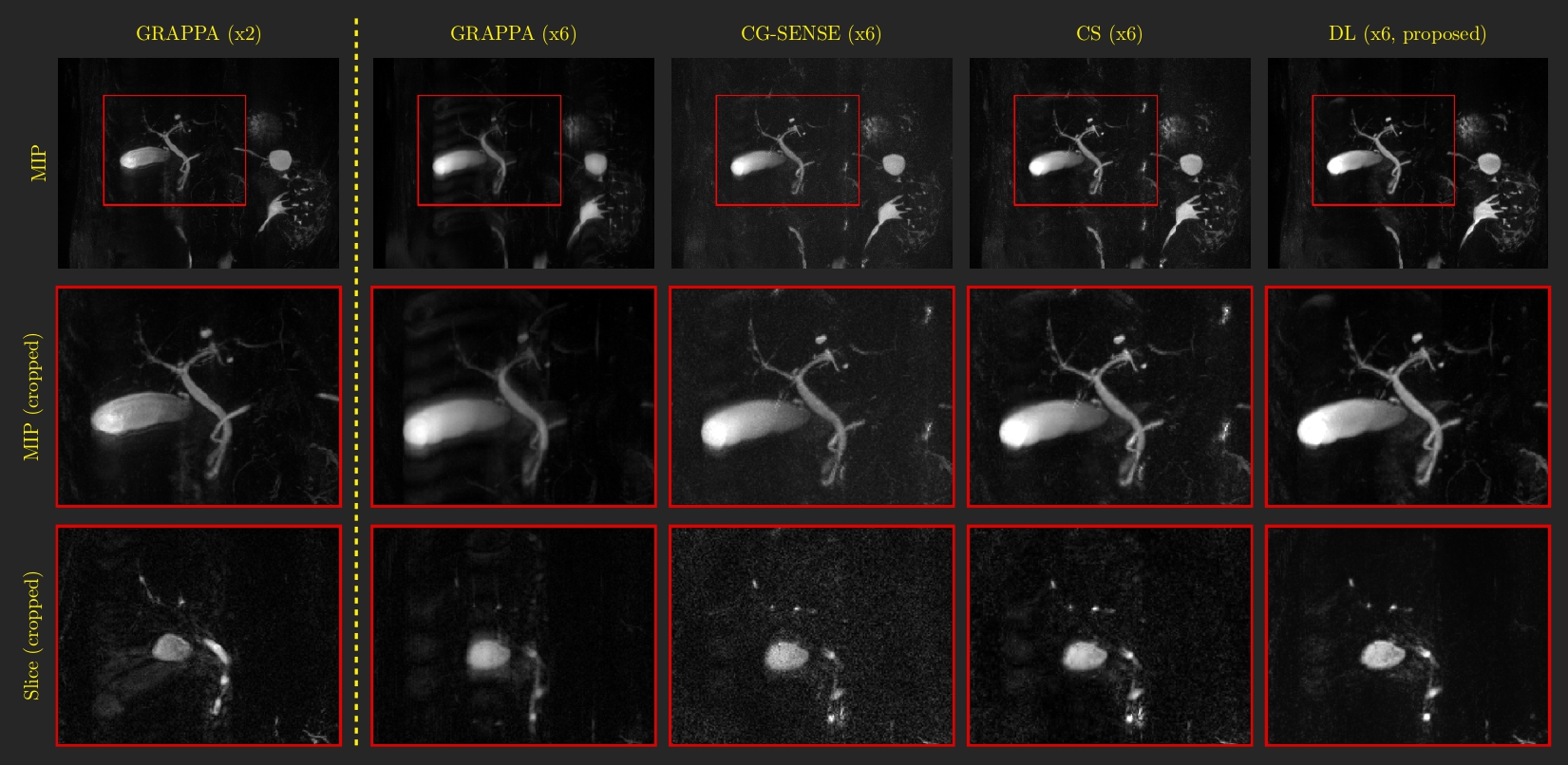
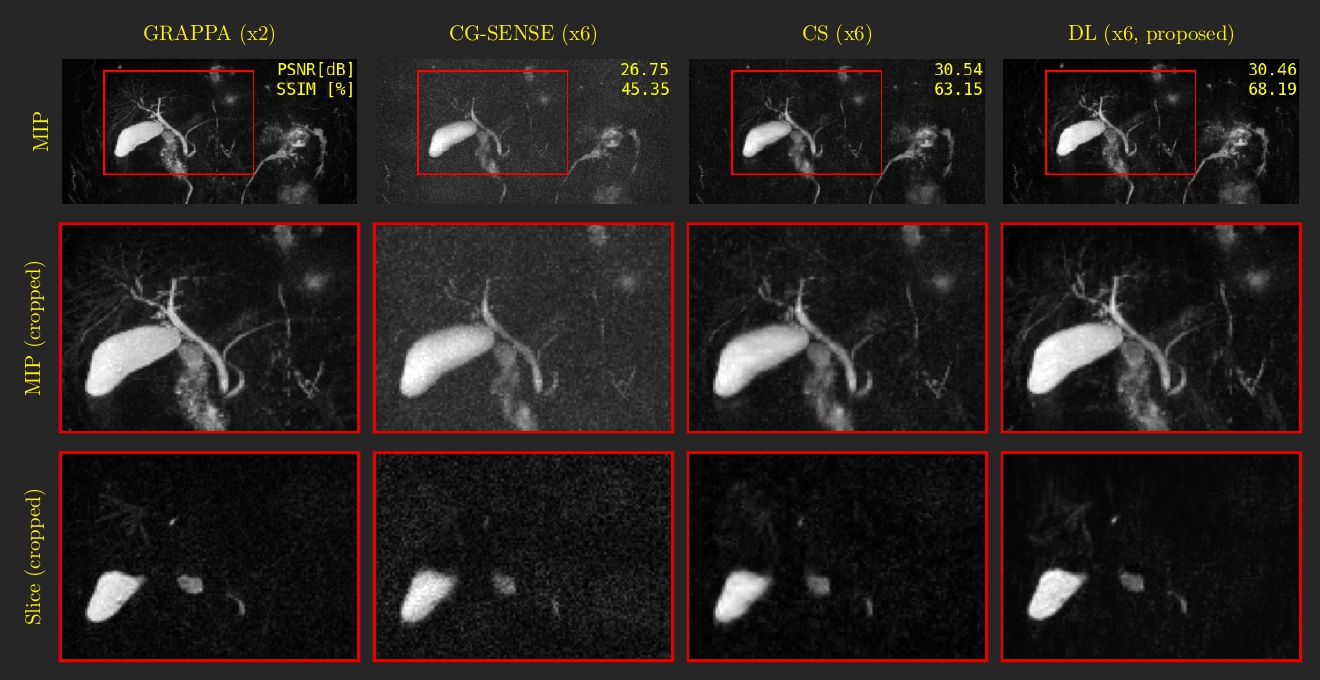
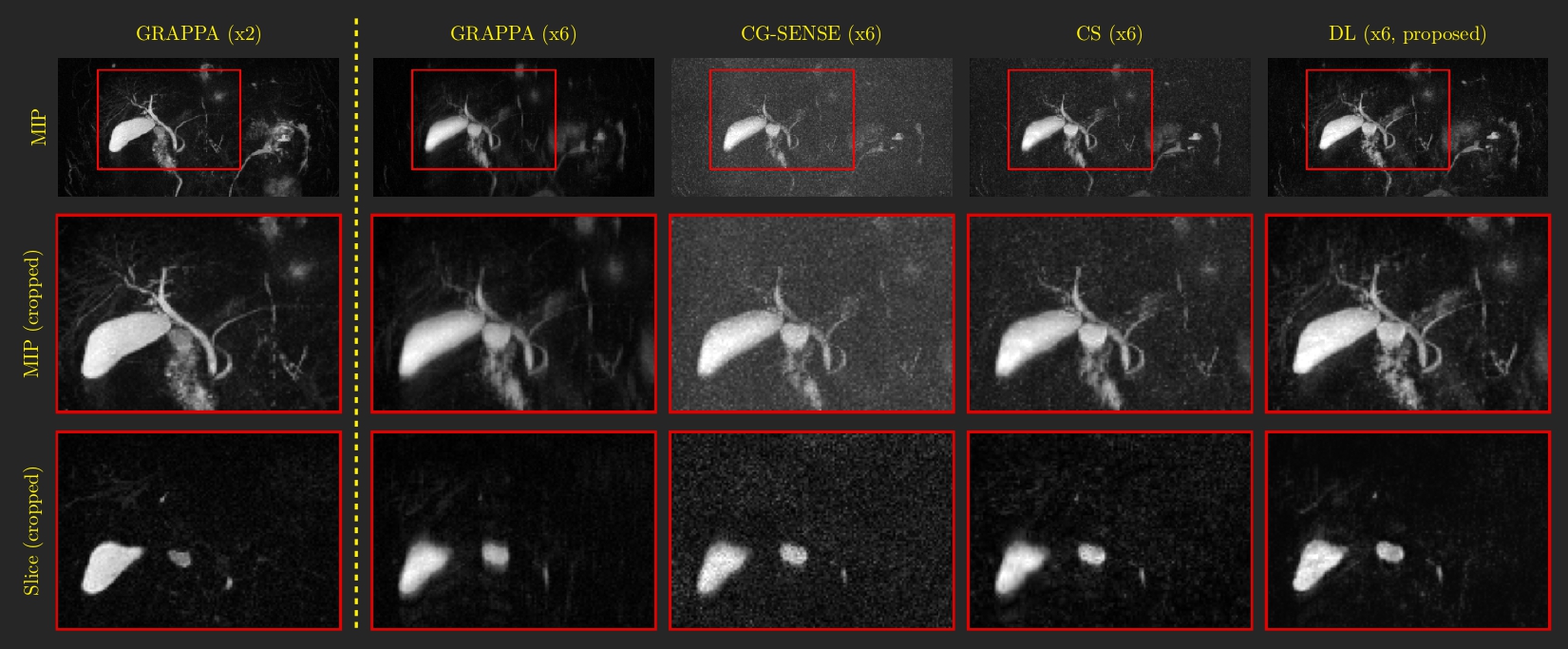
The proposed method consistently outperforms CG-SENSE and CS for prospective and retrospective undersampling at both 3T and 0.55T. DL effectively eliminates crucial aliasing artifacts, compromising image quality in CG-SENSE and CS (Figs. 2 and 3). DL preserves duct intensities, ensuring no disconnections (Fig. 4), and enhances intrahepatic ducts (Figs. 4 and 5). At 0.55T, DL significantly reduces noise levels compared to CG-SENSE and CS (Figs. 4 and 5). For prospectively undersampled data, the DL reconstructions closely resemble the corresponding two-times accelerated acquisitions (Figs. 3 and 5).Discussion and Conclusion
Our results demonstrate that the DL reconstruction can reduce MRCP scan times from 303 seconds to 138 seconds, corresponding to a reduction of 54.5%. Moreover, we observed a noticeably increased signal-to-noise ratio (SNR) for low-field scans. We interpreted this observation that the DL model, trained initially with MRCP data at 3T, effectively leverages its learned capacity to enhance SNR. This capability extends seamlessly to low-field MRI, demonstrating its potential to mitigate the substantial SNR limitations commonly encountered in imaging across various field strengths. Consequently, DL methods represent an effective solution to address the challenging SNR issues encountered in low-field MRCP.Additional clinical evaluations are imperative to validate our method’s clinical efficacy. These studies should encompass patients with irregular breathing patterns, requiring high accelerations, and with lesions to ensure diagnostic-level representation. Through these evaluations, we aim to provide empirical evidence of the method’s safety and benefits when deployed in a clinical setting, underlining its robustness and potential for diverse clinical applications.
In conclusion, our proposed DL reconstruction significantly improves image quality in MRCP for retrospective and prospective acquisitions at 3T and 0.55T. This translates into a noticeable reduction in scan time, making MRCP imaging more efficient and accessible for patients.
Acknowledgements
No acknowledgement found.References
- Hammernik, K. Et al. (2018). Learning a variational network for reconstruction of accelerated MRI data. Magnetic Resonance in Medicine, 79(6), 3055–3071. https://doi.org/10.1002/mrm.26977
- Pruessmann, K. P. Et al. (2001). Advances in sensitivity encoding with arbitrary k-space trajectories. Magnetic Resonance in Medicine, 46(4), 638–651. https://doi.org/10.1002/mrm.1241
- Lustig, M. Et al. (2007). Sparse MRI: The application of compressed sensing for rapid MR imaging. Magnetic Resonance in Medicine, 58(6), 1182–1195. https://doi.org/10.1002/mrm.21391
- Tins, B. Et al. (2012). Three-dimensional sampling perfection with application-optimised contrasts using a different flip angle evolutions sequence for routine imaging of the spine: Preliminary experience. British Journal of Radiology, 85(1016). https://doi.org/10.1259/bjr/25760339
- Morita, S. Et al. (2008). Navigator-triggered prospective acquisition correction (PACE) technique vs. conventional respiratory-triggered technique for free-breathing 3D MRCP: An initial prospective comparative study using healthy volunteers. Journal of Magnetic Resonance Imaging, 28(3), 673–677. https://doi.org/10.1002/jmri.21485
- Uecker, M. Et al. (2014). ESPIRiT - An eigenvalue approach to autocalibrating parallel MRI: Where SENSE meets GRAPPA. Magnetic Resonance in Medicine, 71(3), 990–1001. https://doi.org/10.1002/mrm.24751
- Ong, F. Et al. (2019) SigPy: A Python Package for High Performance Iterative Reconstruction. Proc. ISMRM Annu. Meet. Exhib.
- Griswold, M. A. Et al. (2002). Generalized Autocalibrating Partially Parallel Acquisitions (GRAPPA). Magnetic Resonance in Medicine, 47(6), 1202–1210. https://doi.org/10.1002/mrm.10171
Figures