2794
RANGR: Deep Learning Autonavigation of Free-Breathing Golden-Angle Radial Abdominal MRI1Weill Cornell Graduate School of Medical Sciences, New York, NY, United States, 2Department of Radiology, NewYork-Presbyterian/Weill Cornell Medical Center, New York, NY, United States, 3Department of Medical Physics, Memorial Sloan Kettering Cancer Center, New York, NY, United States, 4Department of Radiology, Memorial Sloan Kettering Cancer Center, New York, NY, United States
Synopsis
Keywords: Machine Learning/Artificial Intelligence, Machine Learning/Artificial Intelligence
Motivation: Current autonavigation methodology for free-breathing MRI methods lacks reliability.
Goal(s): Develop deep learning methodology to estimate a motion signal directly from the acquired data without manually tuned filtering or PCA transformation.
Approach: RANGR uses an encoder network based on the popular VGG architecture to estimate a 1-D respiratory navigator signal from 1-D projections extracted directly from the data.
Results: RANGR improved motion estimation and results on motion-resolved images with reduced artifacts, and was even able to detect motion even in cases where filtering+PCA completely failed.
Impact: The improved robustness and automation presented by RANGR can promote the use of free-breathing motion-resolved imaging for both diagnostic and treatment guidance purposes.
INTRODUCTION
Respiratory motion remains a challenge for abdominal MRI1. Motion-resolved imaging, such as XD-GRASP2, represents a powerful alternative to breath-hold or gating, and recent deep learning approaches, such as Movienet3, have increased acquisition and reconstruction efficiency over compressed sensing. However, the autonavigation technique to sort acquired data into motion states was not updated, and still relies on a combination of adaptive spatial and temporal filtering with principal component analysis (PCA). This method requires manual tuning of numerous parameters and fails to capture a respiratory motion in cases with limited diaphragm coverage and variable motion patterns. Similar unreliability in navigation using electrocardiography has been reported in cardiac MRI, and a deep learning-based electrocardiography-free navigation method for motion-resolved cardiac MRI was recently developed4. Inspired by the work in cardiac MRI, this work proposes a novel data-driven alternative for respiratory autonavigation called RANGR (Respiratory AutoNavigator for Golden-angle Radial free-breathing abdominal MRI) to improve reliability of autonavigated motion-resolved MRI. RANGR is tested on free-breathing golden-angle stack-of-stars acquisitions performed on patients with abdominal tumors and evaluated against the conventional filtering+PCA methodology to reconstruct motion-resolved 4D MRI.METHODS
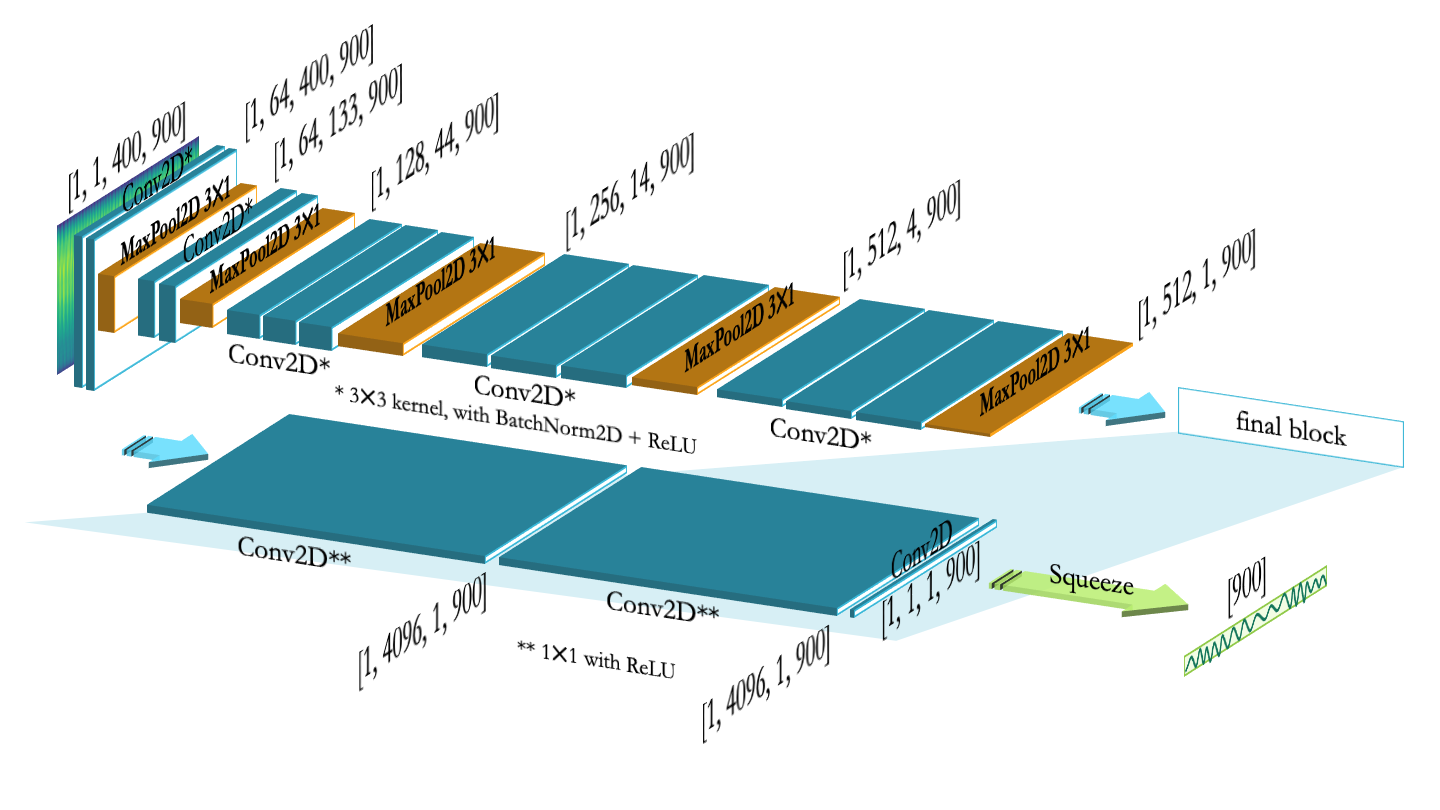
RANGR workflow: The input to RANGR is the matrix of z-projections over time computed directly from the acquired golden-angle stack-of-stars data after taking an inverse Fourier transform along the central position (kx=ky=0) and sum-of-squares coil combination (Figure 1a). The output of RANGR is a 1D respiratory motion signal (1 motion amplitude per time point). Respiratory waveforms obtained via filtering and PCA were used as the target signal. For testing cases, the respiratory motion signal estimated by RANGR was used to sort the acquired k-space data into motion states and perform motion-resolved reconstruction with compressed sensing (XD-GRASP) or Movienet.RANGR architecture and training: RANGR's architecture is based on VGG-164, however, the fully-connected classification head was replaced by 3 convolutional layers of up to 4096 channels (preserving VGG-16’s final feature dimensionality) in order to maintain locality within the learned spatiotemporal features throughout the network. RANGR outputs a respiratory waveform with the same number of time points (or angles) as the input, which is evaluated against the reference waveform using a L1 loss function. RANGR is trained with a batch size of 1, learning rate of 0.001, with the Adam optimizer, for 1000 epochs.
Data acquisition: Free-breathing abdominal MRI data previously acquired from 16 adult subjects were used for training. These subjects were scanned on 5 different 3-T scanners (4 Discovery MR750 and 1 Signa Premier, GE Healthcare) using a 3-D T1-weighted golden-angle stack-of-stars acquisition. Two additional subjects were scanned for validation. Scan parameters are as follows: TR = 3-4 ms, TE = 1.5-2 ms, flip angle = 12º, in-plane resolution = 1.25-1.5 mm, slice thickness = 4-5 mm, number of radial spokes = 900, and scan time = 2.25 min.
Image reconstruction: k-space data was binned by amplitude using the respiratory navigator waveform into 10 different motion states, with an equal number of spokes per motion state (90 spokes). Reconstruction of the undersampled motion-resolved data is performed with temporal compressed sensing as in XD-GRASP2 and with deep learning reconstruction as with Movienet3.
RESULTS
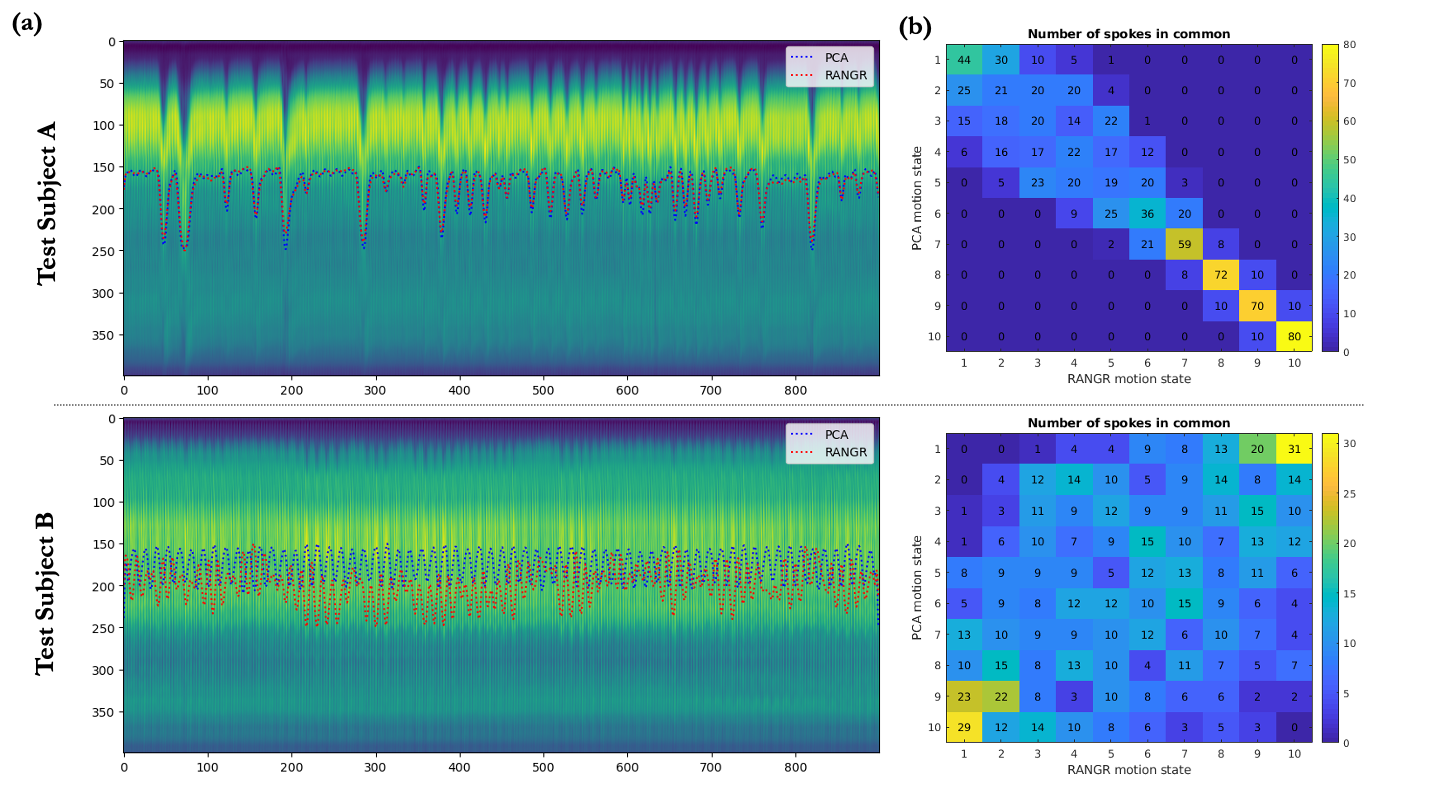
The computation time of RANGR was 0.68 seconds compared to 2.53 seconds using filtering+PCA on the same computer. In Test Subject A for whom PCA had been functional, considerable redistribution of spokes between PCA and RANGR were observed (Figure 3b, top), leading to improved motion-resolved reconstruction for RANGR autonavigation, particularly in terms of flickering and streaking artifacts (Figure 4). In Test Subject B, PCA navigation completely failed to detect respiratory motion, while RANGR was able to estimate a respiratory motion signal that resulted in motion-resolved imaging that correspond to anatomical deformations produced by motion (Figure 5).DISCUSSION
RANGR is a promising robust deep learning alternative to the current PCA-based methodology for respiratory autonavigation. Unlike PCA, RANGR is independent of adaptive filters, which require meticulous tuning of parameters. Additionally, RANGR performs autonavigation in about a quarter of the time as with PCA and can extract motion signal in challenging cases where PCA fails. The improved robustness and automation presented by RANGR can improve respiratory navigation and promote the use of free-breathing imaging in clinical practice.CONCLUSION
RANGR is a reliable and fast alternative to PCA-based autonavigation for free-breathing abdominal MRI. The improvement in motion resolution and reconstruction quality using RANGR can be important both diagnostically (free-breathing adult and pediatric imaging) and therapeutically (MRI-guided radiotherapy of tumors affected by respiratory motion).Acknowledgements
The work was supported by NIH grant R01-CA255661.References
- Stadler, A., Schima, W., Ba-Ssalamah, A., Kettenbach, J. and Eisenhuber, E., 2007. Artifacts in body MR imaging: their appearance and how to eliminate them. European radiology, 17, pp.1242-1255.
- Feng, L., Axel, L., Chandarana, H., Block, K.T., Sodickson, D.K. and Otazo, R., 2016. XD‐GRASP: golden‐angle radial MRI with reconstruction of extra motion‐state dimensions using compressed sensing. Magnetic resonance in medicine, 75(2), pp.775-788.
- Murray, V., Siddiq, S., Crane, C., El Homsi, M., Kim, T.H., Wu, C. and Otazo, R., 2023. Movienet: Deep space–time‐coil reconstruction network without k‐space data consistency for fast motion‐resolved 4D MRI. Magnetic Resonance in Medicine.
- Hoppe, E., Wetzl, J., Yoon, S.S., Bacher, M., Roser, P., Stimpel, B., Preuhs, A. and Maier, A., 2021. Deep learning-based ECG-free cardiac navigation for multi-dimensional and motion-resolved continuous magnetic resonance imaging. IEEE Transactions on Medical Imaging, 40(8), pp.2105-2117.
- Simonyan, K. and Zisserman, A., 2014. Very deep convolutional networks for large-scale image recognition. arXiv preprint arXiv:1409.1556.
Figures
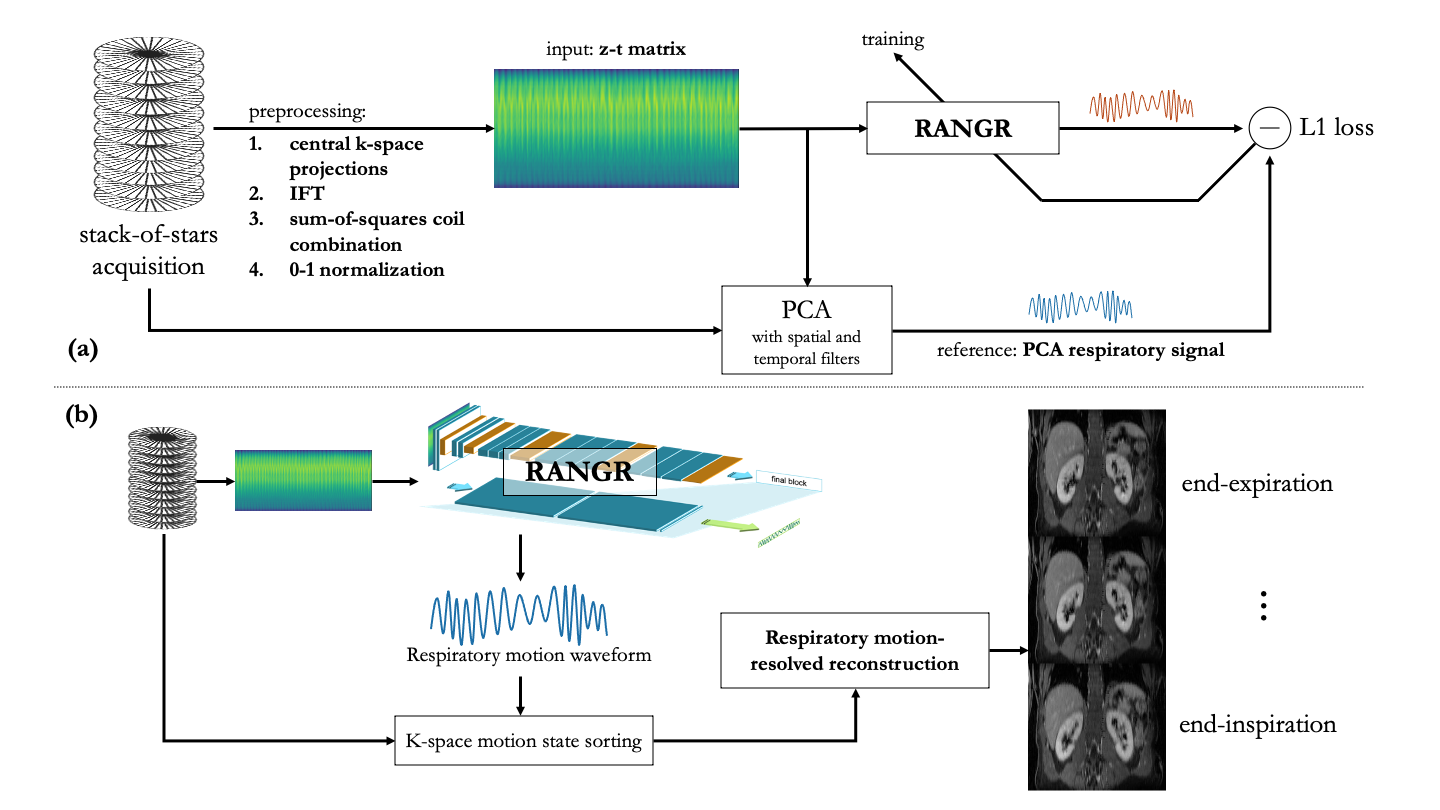
Figure 1: Overall RANGR workflow and motion-resolved reconstruction. (a) 3-D MRI data were acquired using golden-angle stack-of-stars sampling. 1-D projections for each angle/time point were obtained by applying inverse Fourier transform (IFT) along the kz line defined at kx=ky=0. Projections are coil-combined using sum-of-squares and concatenated as a z-t matrix (input to RANGR). The filtering+PCA results served as training reference. (b) For testing, the motion signal from RANGR was used to sort k-space data into motion states and perform motion-resolved reconstruction.